
To analyze and correlate the audiometric findings of high frequencies (9–16kHz) in adolescents with their hearing habits and attitudes, in order to prevent noise-induced hearing loss.
MethodThis was a descriptive cross-sectional study, which included 125 adolescents in a sample of normal-hearing students, at a state school. The subjects performed high-frequency audiometry testing and answered a self-administered questionnaire addressing information on sound habits concerning the use of personal stereo devices. The sample was divided according to the exposure characteristics (time, duration, intensity, etc.) and the results were compared with the observed thresholds, through the difference in proportions test, chi-squared, Student's t-test, and ANOVA, all at a significance level of 0.05.
ResultsAverage high-frequency thresholds were registered below 15dB HL and no significant correlation was found between high frequency audiometric findings and the degree of exposure.
ConclusionThe prevalence of harmful sound habits due to the use of personal stereo devices is high in the adolescent population, but there was no correlation between exposure to high sound pressure levels through personal stereos and the high-frequency thresholds in this population.
Analisar e correlacionar os achados audiométricos de altas frequências (9–16 kHz) em adolescentes com seus hábitos e atitudes de audição para prevenir perda auditiva induzida por ruído.
MétodoEste é um estudo transversal descritivo que incluiu 125 adolescentes em uma amostra de alunos ouvintes em uma escola estadual. Os indivíduos foram submetidos a testes de audiometria de altas frequências e responderam a um questionário autoadministrado abordando informações sobre hábitos sonoros com relação ao uso de MP3 players. A amostra foi dividida de acordo com as características de exposição (tempo, duração, intensidade, etc.) e os resultados foram comparados aos limites observados, por meio do Teste de Diferença de Proporções, Qui-quadrado, teste T de Student e análise de variância (ANOVA), todos em um nível de significância de 0,05.
ResultadosFoi registrada média de limiares de altas frequências abaixo de 15dB HL e não foi encontrada nenhuma correção significativa entre os achados audiométricos de altas frequências e o grau de exposição.
ConclusãoA prevalência de hábitos sonoros prejudiciais devido ao uso de MP3 players é alta na população adolescente, porém não houve correlação entre a exposição a altos níveis de pressão sonora por meio de MP3 players e os limiares de altas frequências nessa população.
Studies related to the recreational habits with exposure to high sound pressure levels (SPL), especially through stereos for personal use, have proved to be recurring in different adolescent populations, with prevalent data at over 90%.1,2
Considering that technological development has provided increasing quality and power of earphones and headsets, with amplifiers that reach 130dB SPL without sound intensity distortion,3,4 and coupled with personal stereo products that are inexpensive, highly portable, store large volumes of music, and have long-life batteries, there has arisen a situation in which the personal stereo (PS) has become particularly prevalent and harmful among the young urban population.4,5
Some possible explanations for such exposure involve: the need for self-worth and social acceptance, leading to the adoption of fads in order to become a member of a group6; customization potential of a sound environment leading to personal isolation4; and even experimentation with pleasure and euphoria that may arise from the release of endorphins due to the physiological defense reaction that accompanies exposure to sound levels above 80dB SPL.7
Although music has been considered less harmful to the human hearing system than an equivalent industrial noise, given the former's intermittent nature, allowing for a hearing recovery period, a lower dominant frequency, and more discreet alert reactions due to personal interpretation of whether it is a pleasant sound6; one must highlight the irreversible characteristic of high SPL induced hearing loss (HSPLIHL), greater susceptibility of cochlear damage in the youngest populations,8 and the increase in the predisposition to develop hearing loss in adulthood when there is early exposure to high noise levels.9
Traditionally, the diagnosis of HSPLIHL, as well as its monitoring and verification, are performed by subjective audiometric threshold testing observed through pure tone audiometry (PTA) and objective audiological evaluations, such as auditory brainstem response (ABR) and otoacoustic emissions (OAE) testing, especially distortion product (DPOAE).10
However, in view of the recognized early elevation of hearing thresholds for high frequencies, compared to normal thresholds, in light of potentially harmful conditions for the cochlear system such as exposure to occupational noise and/or ototoxic drugs, certain systemic and ontological diseases, as well as during the process of auditory aging. High-frequency audiometry (HFA) has been indicated as an instrument in the early diagnosis of hearing loss when compared to PTA and OAE.11–15
This study aimed to analyze HFA findings in adolescents and correlate them with their use of PSs.
MethodThis was a cross-sectional descriptive study approved by the Research Ethics Committee recorded under No. 2576.183/2011-08. All participants signed an informed consent authorizing the use of data collected after clarification regarding the research objectives and procedures.
The subjects invited to participate in the study were all adolescent students of both genders enrolled in a state school in the city of Curitiba, Brazil and present during evaluation days. Established inclusion criteria were: signing the informed consent, a normal otorhinolaryngological examination, evaluations for acoustic impedance, and pure tone audiometry (n=134). Excluded from the final body of research were students who had no habit of listening to music on PSs (n=9).
The evaluation, performed by otorhinolaryngologist, paid special attention to nasal and sinus structures and structures of the outer and middle ear, cleaning the external auditory canal when needed.
In the audiological evaluation, normal thresholds were considered to be up to 25dB HL per classification by Lloyd and Kaplan (1978),16 and obtained through pure tone audiometry (500–8000Hz), performed with an Otometrics brand device (Madsen Itera II®, Taastrup, Denmark), with TDH39® headphones (MedRx, Inc., RD, USA), calibrated in a sound enclosure in accordance with the standards required by the Brazilian Federal Speech Council.16 To measure acoustic impedance, an Interacoustics brand middle ear analyzer was used, AT22® model (Otometrics®, Middelfart, Denmark), and normal results were considered to be those compatible with a type A tympanogram, according to Jerger.16
Students included in the selection criteria were invited to answer a self-administered questionnaire composed of open and closed questions, addressing sound habits regarding the use of PSs, including information on exposure characteristics (exposure time in years, days per week, and hours per day, insertion or earmuff phones, habit of sleeping with the unit turned on, habit of talking while using the device, and commonly used intensity) and symptoms associated with exposure. A visual analog scale was employed for estimating the volume range commonly used by the study subjects. Any questions raised by the subjects were clarified by the research team.
Next, an audiometric evaluation of high frequencies was carried out under the acoustic conditions described above, with the aforementioned audiometer, using KOSS HV/PRO (KOSS®, USA) headphones, at thresholds expressed in dB HL, at the frequencies of 9000, 11,200, 12,500, 14,000, and 16,000Hz.
The results were statistically analyzed by the Chi-squared test, difference in proportions test, Student's t-test, and ANOVA; the 0.05 significance level was utilized.
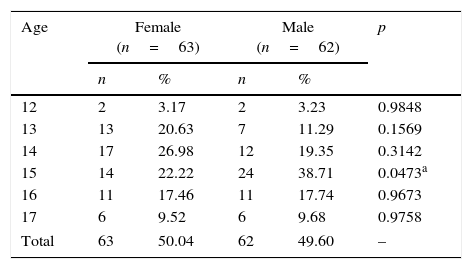
ResultsUpon establishing inclusion criteria using perspectives both from clinical and audiological normality (n=134) as well as PS use (n=125), a prevalence of PS use was found among normal hearing teenagers (93.28%). A comparison of the sample by age and gender is shown in Table 1.
Description of sample by age and gender.
| Age | Female (n=63) | Male (n=62) | p | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| 12 | 2 | 3.17 | 2 | 3.23 | 0.9848 |
| 13 | 13 | 20.63 | 7 | 11.29 | 0.1569 |
| 14 | 17 | 26.98 | 12 | 19.35 | 0.3142 |
| 15 | 14 | 22.22 | 24 | 38.71 | 0.0473a |
| 16 | 11 | 17.46 | 11 | 17.74 | 0.9673 |
| 17 | 6 | 9.52 | 6 | 9.68 | 0.9758 |
| Total | 63 | 50.04 | 62 | 49.60 | – |
Note: Difference of proportions test, significance level of 0.05.
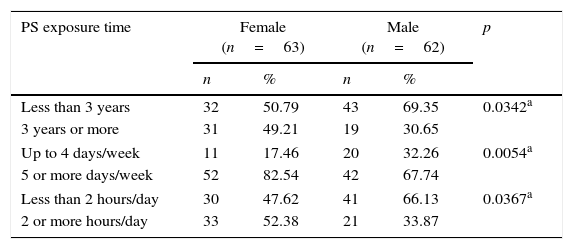
Analyzing the sample by time of exposure to PS, it was found that 58.4% (n=73) of individuals made daily use of their devices, with equivalent answers from both genders. However, using the Chi-squared test at a significance level of 0.05, it was observed that there was significantly longer PS use by females, per Table 2.
Description of sample by habits of PS use.
| PS exposure time | Female (n=63) | Male (n=62) | p | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Less than 3 years | 32 | 50.79 | 43 | 69.35 | 0.0342a |
| 3 years or more | 31 | 49.21 | 19 | 30.65 | |
| Up to 4 days/week | 11 | 17.46 | 20 | 32.26 | 0.0054a |
| 5 or more days/week | 52 | 82.54 | 42 | 67.74 | |
| Less than 2 hours/day | 30 | 47.62 | 41 | 66.13 | 0.0367a |
| 2 or more hours/day | 33 | 52.38 | 21 | 33.87 | |
Note: Chi-squared test, significance level of 0.05.
PS, personal stereo.
Also, using the Chi-squared test, more harmful habits were identified among females for the following variables: habit of sleeping with the PS turned on (p=0.0037), and perceived volume by others (p=0.0458). Moreover, through the difference in proportions test, a preference was shown for insertion-type earphones (p=0.0150), with both tests at the 0.05 significance level.
It was observed that almost 40% of adolescents (n=49) had experienced at least one otological symptom due to the use of PSS, with tinnitus prevalence of 21.6%, followed by ear pain, ear fullness, itching, dizziness, and hearing loss. Attempting to correlate the prevalence of otologic complaints with the habitual use of PSS by applying the chi-squared test and the difference of proportions Test, at a significance level of 0.05, no significant difference was found between those subjects more and less exposed.
Evaluating the results of hearing thresholds for the high frequencies tested, mean values were obtained below 15dB HL, with slightly better results for females from 11,200Hz. With regard to inequalities between the ears, there was no statistically significant difference, although slightly better answers for the right ear, only among females, were observed.
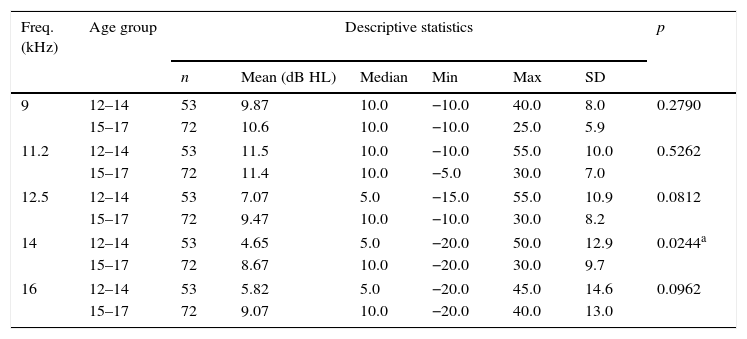
Considering both age groups, there was an average of higher thresholds in the older group for all frequencies tested except at 11,200Hz. However, there was only a significant difference at 14,000Hz, with Student's t-test at the 0.05 significance level. The characterization of the high frequency thresholds age is shown in Table 3.
Description of hearing thresholds in decibels at frequencies of 9000–16,000Hz, by age group.
| Freq. (kHz) | Age group | Descriptive statistics | p | |||||
|---|---|---|---|---|---|---|---|---|
| n | Mean (dB HL) | Median | Min | Max | SD | |||
| 9 | 12–14 | 53 | 9.87 | 10.0 | −10.0 | 40.0 | 8.0 | 0.2790 |
| 15–17 | 72 | 10.6 | 10.0 | −10.0 | 25.0 | 5.9 | ||
| 11.2 | 12–14 | 53 | 11.5 | 10.0 | −10.0 | 55.0 | 10.0 | 0.5262 |
| 15–17 | 72 | 11.4 | 10.0 | −5.0 | 30.0 | 7.0 | ||
| 12.5 | 12–14 | 53 | 7.07 | 5.0 | −15.0 | 55.0 | 10.9 | 0.0812 |
| 15–17 | 72 | 9.47 | 10.0 | −10.0 | 30.0 | 8.2 | ||
| 14 | 12–14 | 53 | 4.65 | 5.0 | −20.0 | 50.0 | 12.9 | 0.0244a |
| 15–17 | 72 | 8.67 | 10.0 | −20.0 | 30.0 | 9.7 | ||
| 16 | 12–14 | 53 | 5.82 | 5.0 | −20.0 | 45.0 | 14.6 | 0.0962 |
| 15–17 | 72 | 9.07 | 10.0 | −20.0 | 40.0 | 13.0 | ||
Note: Student's t-test, significance level of 0.05.
To describe and analyze the results by gender, there was a statistically significant difference in frequencies starting at 12.5 KHz for the 15–17 year-old age group, with the worst average being among males.
The analysis of audiometric thresholds in terms of PS exposure showed no significant difference in any frequently tested, whether for PS-use duration variables in years, days per week, or hours per day, using Student's t-test; nor for intensity variables or type of earphone using the ANOVA test, with both tests at the 0.05 significance level. There was some higher average in all tested frequencies, for both ears, among those who used PS for five or more days per week.
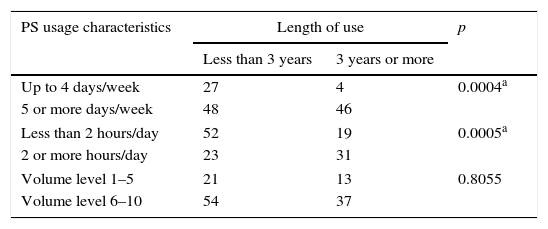
Correlations on exposure are described in Table 4, in which less PS use was demonstrated in days per week and hours per day for the subjects who started using PSs more recently. A preference for higher sound level intensity (volume) was also observed among those who made use of the devices at least five days per week.
Relationships among length of PS use and usage characteristics (in number of days per week, number of hours per day, and volume level).
| PS usage characteristics | Length of use | p | |
|---|---|---|---|
| Less than 3 years | 3 years or more | ||
| Up to 4 days/week | 27 | 4 | 0.0004a |
| 5 or more days/week | 48 | 46 | |
| Less than 2 hours/day | 52 | 19 | 0.0005a |
| 2 or more hours/day | 23 | 31 | |
| Volume level 1–5 | 21 | 13 | 0.8055 |
| Volume level 6–10 | 54 | 37 | |
Note: Chi-squared test, significance level of 0.05.
PS, personal stereo.
The popularization of the use of PSs, particularly in younger populations, and the lack of regulation on the maximum sound output intensity of devices, have contributed to increasing recreational exposure to sound at high intensity in this age group.4 The high prevalence of habitual PS use observed (93.28%) has been repeated in studies involving adolescent populations on different continents, reaching 95.6% of subjects in some samples.1,2,7
The PS usage profile (Table 2), use for at least five days a week, at least two hours per day, although for less than three years, reflects the presence of positive attitudes toward noise in the adolescent population. This is a pattern of device misuse that has been identified in several studies.4,6,17–19
However, differently from what is commonly referred to in studies,20,21 the observation of more deleterious habits in the female group might be explained by the greater need for isolation and a prevalence of symptoms related to anxiety and depression among girls.22,23
Given the knowledge of the deleterious potential of high SPL in hearing health, it is estimated that about 10–30% of PS users are at risk of noise-induced hearing loss (NIHL) after five or more years of use, due to exposure to high-intensity noise over a long period of time.1 Since the occurrence of otological symptoms can signal temporary or permanent subclinical hearing damage, the high prevalence of otological complaints (39.2%) among the present subjects stands out, although some studies have shown results up to 67.2%.5
Comparing the presence of tinnitus among more and less exposed groups, no difference in the prevalence of otological symptoms was observed, coinciding with other studies,21 although some authors have identified a positive correlation with PS abuse when the subject has been exposed for a longer time,5,22 at higher intensities, and using insertion-style earphones.2
Average thresholds below 15dB HL were identified for both genders in all frequencies tested, supporting the suggestion of adopting such values as parameters of normality for the adolescent population.24 The identification of slightly better results in the female group starting at 11,200Hz has also been recurrent in high frequency studies, demonstrating the dependence of auditory thresholds with males already in adolescence.25,26 The observation of a notch at the frequency of 11,200Hz for the results in boys finds no reference in the literature, although Sulaiman et al.21 have observed positive correlation between PS volume used and thresholds at 11.2 and 14kHz.
With regard to the disparity between ears, no differences between the thresholds were found, although slightly better responses were seen in the right ear in the male group. This finding is quite controversial in the literature and, although some authors present results similar to those identified,27 there is no consensus on this issue, including findings of worse thresholds on the right.28 The absence of agreement on this variable in the HFA may result from a lack of specification and statistical processing of interaural thresholds found in some studies.
The characterization of high frequency thresholds by age group (Table 3) shows worse responses in the older age group, except at the frequency of 11.2kHz, reinforcing the direct relation of age on the HFA results in adolescence25,29; however, studies show no agreement on the exact period of the beginning of this decrease.24,26
The analysis of audiometric thresholds related to exposure characteristics (duration of PS use, type of earphone, volume used, gender, etc.) showed no significant difference in any frequency tested. Nonetheless, it was observed that in both ears, at all frequencies, there were worse responses in the group with habitual usage for five or more days per week, although with no significant difference.
Some studies have identified thresholds up to 6dB HL greater in subjects with at least five years of PS use when compared to unexposed subjects.25 In addition, although these studies demonstrated a positive correlation, although weak, regarding PS use and increased responses at 11.2 and 14kHz,23 other authors failed to identify such a correlation.30
In addition to methodological and sample group differences among several studies, the possibility exists that subjects with high SPL exposure who were investigated in this research have not shown hearing damage due the recent start of PS use (60% with use for less than three years). Moreover, the correlations related to exposure characteristics have shown that users with longer time of use also have more weekly hours of use, and with greater intensity (volume) among regular users.
Finally, during the analyses, it was realized that some factors may have limited this study; the homogeneity of the sample, despite the random selection of subjects, did not allow for groups with major differences in exposure.
Thus, further studies should be conducted with young people, but in broader age ranges and including a larger sample size. The authors also recommend longitudinal and cross-sectional studies between exposure groups in order to clarify or reduce conflicting results.
It was found that the HFA findings were successfully analyzed, with emphasis on the observation at thresholds below 15dB HL, likely to function as normal reference values for adolescence with a positive relationship to age in males starting from 15 years old.
In parallel, there was high prevalence of harmful sound habits regarding the use of PS. However, although no correlation was observed between exposure to high SPL and thresholds of high frequencies in the population studied, given the irreversible nature of NIHL, audiological monitoring and educational measures to contain such habits and attitudes are important.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Silvestre RA, Ribas Â, Hammerschmidt R, de Lacerda AB. High-frequency profile in adolescents and its relationship with the use of personal stereo devices. J Pediatr (Rio J). 2016;92:206–11.
This article was written as part of the thesis of the main author for a Master's degree.




