

Sleep deprivation in adolescents has lately become a health issue that tends to increase with higher stress prevalence, extenuating routines, and new technological devices that impair adolescents’ bedtime. Therefore, this study aimed to assess the excessive sleepiness frequency and the factors that might be associated to it in this population.
MethodsThe cross-sectional study analyzed 531 adolescents aged 10–18 years old from two private schools and one public school. Five questionnaires were applied: the Cleveland Adolescent Sleepiness Questionnaire; the Sleep Disturbance Scale for Children; the Brazilian Economic Classification Criteria; the General Health and Sexual Maturation Questionnaire; and the Physical Activity Questionnaire. The statistical analyses were based on comparisons between schools and sleepiness and non-sleepiness groups, using linear correlation and logistic regression.
ResultsSleep deprivation was present in 39% of the adolescents; sleep deficit was higher in private school adolescents (p<0.001), and there was a positive correlation between age and sleep deficit (p<0.001; r=0.337). Logistic regression showed that older age (p=0.002; PR: 1.21 [CI: 1.07–1.36]) and higher score level for sleep hyperhidrosis in the sleep disturbance scale (p=0.02; PR: 1.16 [CI: 1.02–1.32]) were risk factors for worse degree of sleepiness.
ConclusionsSleep deficit appears to be a reality among adolescents; the results suggest a higher prevalence in students from private schools. Sleep deprivation is associated with older age in adolescents and possible presence of sleep disorders, such as sleep hyperhidrosis.
A privação de sono na adolescência é um importante problema de saúde na atualidade e só tende a se agravar com o aumento do estresse, da rotina extenuante e do advento de novos aparelhos tecnológicos que parecem refletir negativamente no início do sono em adolescentes. O estudo objetiva avaliar a frequência da sonolência excessiva e quais fatores podem estar associados à ela nesta população.
MétodosO estudo transversal avaliou 531 adolescentes de 10 a 18 anos em duas escolas de ensino privado e uma de ensino público, aplicando para cada adolescente cinco questionários: Cleveland Adolescent Sleepiness Questionnaire; Sleep Disturbance Scale for Children; Critério de Classificação Econômica Brasil; Questionário geral de saúde e maturação sexual; Questionário de atividade física. Realizou-se comparações entre as escolas e entre grupos com e sem sonolência por meio de correlação linear e regressão logística.
ResultadosObservou-se privação de sono em 39% dos adolescentes, débito de sono maior para escolares do ensino privado (p<0,001) e correlação positiva entre idade e débito do sono (p<0,001; r=0,337). Na regressão logística, apontou-se como fatores para pior grau de sonolência maior faixa etária dos escolares (p=0,002; RP: 1,21[IC:1,07-1,36]) e maior escore na variável hiperidrose do sono do questionário de distúrbios do sono (p=0,02; RP: 1,16[IC:1,02-1,32]).
ConclusõesConclui-se que o déficit de sono é uma realidade na população estudada, apresentando-se pior em escolares do ensino privado. A privação de sono está relacionada com a maior faixa etária dos adolescentes e possível presença de distúrbios do sono, como a hiperidrose do sono.
Sleep is extremely important for appropriate physical growth, emotional stability, behavior, and maintenance of cognitive function in adolescents.1,2 Physiological studies have shown that adequate sleep is also important for memory consolidation, which has serious implications on school success in this age group.2,3 A good quality night sleep will reflect in better school performance and increased motivation to study.3 Several studies suggest that this population requires an average of eight to nine hours of sleep per night to adequately perform everyday activities and absorb the physical and mental benefits of sleep.4,5
Although this is the goal for a good-quality sleep, it is known that adolescents have been sleeping for shorter periods than necessary.6 The upgrading and launching of increasingly more attractive videogames and virtual reality simulators and the broad presence of Internet through chat groups, and social networks are aggravating factors for inadequate sleep.7 The presence of TVs, video game consoles, and computers in bedrooms7–9 are related to greater sleep deprivation. With the advent and popularization of handheld devices, more studies should be performed to evaluate their effects on sleep, as adolescents have the habit of taking them to bed at bedtime, consequently delaying sleep onset. Moreover, the current hectic lifestyle, especially in large cities, negatively affects adolescents, making them victims of anxiety, aggression, stress, social and school burdens, with possible damage to an adequate sleep.2,10
Sleep deprivation, more than previously thought, is not restricted to psychosocial alterations. Recently, associations were observed between sleepiness and obesity.11 Overweight adolescents appear to have a shorter and more disturbed sleep,11,12 and overweight is also a risk factor for sleep-disordered breathing, such as obstructive sleep apnea syndrome (OSAS).13
What is known so far is that both internal factors, such as sexual maturity, age, gender, and obesity, as well as external factors, such as school shift, use of technology and drug use, can influence the sleep.5,7 However, Brazil still lacks large studies that demonstrate this scenario in the country.
Thus, to evaluate sleepiness in this population, an alternative is the use of questionnaires. One of the most often used, the Pediatric Daytime Sleepiness Scale (PDSS),14 shows as limitation a restrict age group for adolescents. The Modified Epworth Sleepiness Scale (ESS),15 in turn, is an adaptation of the Epworth Sleepiness Scale, containing few questions in its evaluation and also restricted age group. Thus, as it addresses questions from four areas (sleepiness at school, alert in school, sleepiness in the evening, and sleepiness during transport), the Cleveland Adolescent Sleepiness Questionnaire (CASQ)16 is one of the most complete questionnaires to assess excessive sleepiness in that population, even though it does not have a cutoff point for the classification of presence or not of sleepiness. Although it is a new questionnaire to assess sleepiness, other questionnaires commonly applied to children and adolescents are used in smaller populations and have limited national application.
Given this reality, the aim of this study was to verify the frequency of excessive daytime sleepiness in adolescents, as well as the effect of several variables on excessive sleepiness.
MethodsThis was a prospective study and the assessment was performed using specific questionnaires applied to a population of 545 adolescents aged 10–18 years from three schools (two private and one public) in the city of São Paulo and adjacent towns, chosen by convenience during the second half of 2013. For inclusion, the adolescents were invited to participate in the study through an explanatory lecture. Adolescents aged between 10 and 18 years old from schools who agreed to participate were recruited. Participants had to have the informed consent form and the adolescent term of agreement duly signed. Adolescents who had some degree of mental deficit or other disability that prevented them from appropriately answering the questionnaires were excluded. Those who were chronic users of drugs that could influence the sleep–wake cycle were also excluded. The study was approved by the Research Ethics Committee of Universidade Federal de São Paulo in 2013, under registration number 15925613.4.0000.5505.
The studied variables were age, gender, degree of sexual maturation, ethnicity, body mass index (BMI), school shift, economic status, physical inactivity, presence of chronic diseases and continuous use of drugs, economic status, presence of excessive sleepiness, sleep disorders, and hours of sleep.
The assessment of these variables was carried out through five questionnaires, distributed by a single researcher and filled out at home. One of them was the Portuguese (Brazil) version of the Cleveland Adolescent Sleepiness Questionnaire (CASQ)16 containing 16 questions, which assesses the sleepiness degree of adolescents and its limit values are 16–80 points, without a cutoff point for the classification of the presence or absence of sleepiness. The adaptation of the CASQ to the Portuguese language was performed after the authorization from the original author of the study and two individuals, fluent in English and Portuguese, translated it independently. As the first versions were obtained, the next step was to translate them back into English, which was performed by two native English speakers, both bilingual. The two translations were assessed together and changes were made until a consensus was reached, with only one version remaining. Then, this translated version was analyzed by experts in the field and changes were made again to achieve a single decision. This second version was tested with 15 adolescents who, after reading the questions, explained their understanding of the questions and whether they had interpretation doubts. The 16 questions were understood by at least 80% of the adolescents. The questions that led to comprehension doubts by over 10% of the adolescents were rewritten, resulting in the third version of the translation, defined as the final version.
Another questionnaire was the validated version into the Brazilian Portuguese (Ferreira et al.)17 of the Sleep Disturbance Scale for the Children (SDSC), developed by Bruni et al.18 This questionnaire evaluates, in 26 questions, six groups of frequent sleep disorders in children (disorders of initiating and maintaining sleep, sleep-disordered breathing, disorders of arousal, sleep–wake transition disorders, disorders of excessive somnolence, sleep hyperhidrosis). There are no cutoff points for the classification, and values can vary from 26 to 130 in total. One more question was added to the questionnaire about hours of sleep on the weekend for the calculation of sleep deficit.
The socioeconomic status questionnaire Brazilian Economic Classification Criteria, formulated by the Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa), which classifies the population in social classes from A to E according to the existing items at home and educational level of the head of family, was also applied to the adolescents.
A general questionnaire evaluated the remaining variables: the degree of sexual maturation was assessed by self-report, according to the drawings of Tanner's maturation stages for genital, breast, and hair development.19 Two versions were used, according to gender. Nutritional assessment was accomplished using the more recent self-reported measures of weight and height to calculate body mass index, and the diagnosis of the nutritional status was based on BMI Z-score according to the growth curves of the World Health Organization.20 Obesity was defined as the BMI Z-score >two standard deviations (>+2SD).
The physical activity questionnaire included three questions about the frequency of physical activity and sedentary activities developed by the adolescents, adapted to the Brazilian reality from the original questionnaire developed by the Pediatric Sleep Center for Sleep Disorders of the University of Chicago.21 The questionnaire classifies as active students who perform more than 30min of exercise more frequently than three times a week. At the end, they also answered two questions in this questionnaire regarding the presence of chronic diseases and use of continuous medication.
In the study, the qualitative variables were represented as the number of observations and percentage, whereas the quantitative variables were represented as mean and standard deviation. Sleep deprivation was considered when the sleep deficit, number of mean hours slept during the weekend subtracted from the number of mean hours of sleep during the week, was ≥2h. The authors compared the several variables between the two groups, public school and private school, using the Student's t-test for numerical variables (age, CASQ score, SDSC value by group of sleep disorders and hours of sleep, and medication) and the chi-squared test for categorical variables (gender, sexual maturation). The remaining variables were also compared for the presence of excessive daytime sleepiness through CASQ, the dependent variable, having as cutoff the categorical CASQ value (median, 38 points), and as independent variables: age, gender, type of school (private vs. public), school shift (morning vs. afternoon), obesity, physical activity, chronic disease, sleep deficit, sleep complaints (hours of sleep during the week, hours of sleep on weekends, and value per groups of the SDSC questionnaire). Subsequently, using Pearson's correlation coefficient, the dependent variable CASQ was compared with the previously obtained statistically significant variables. The age variable was also compared with CASQ and sleep deficit. To evaluate the effect of several variables on the quality of sleep, a multivariate logistic regression analysis between the categorical CASQ and significant variables was performed. A p-value <0.05 was considered significant for all analyses.
ResultsThe study included a total of 545 questionnaires, of which 14 were delivered unfilled, resulting in 531 valid questionnaires. Of these, 368 students (69%) fully answered all questionnaires. An active search was carried out with 163 adolescents with incomplete questionnaires to have them completed, but it was unsuccessful. However, the usable data were accepted, as long as they did not impair the study.
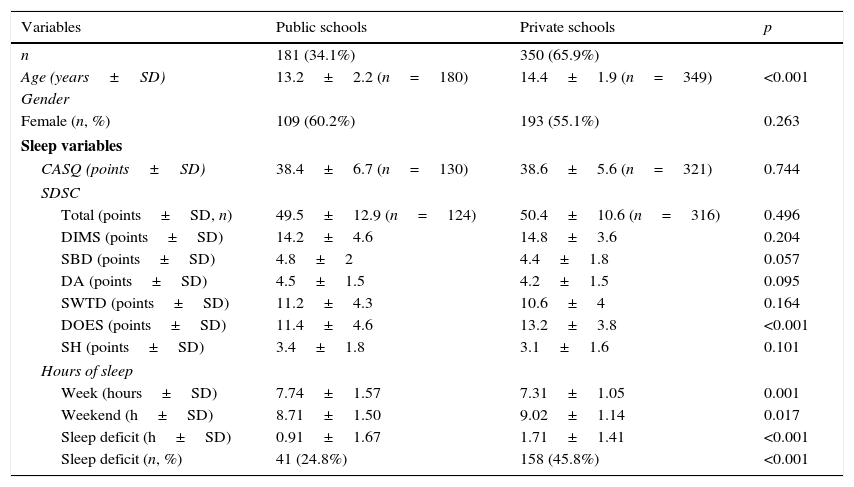
Table 1 shows the most important demographic and sleep characteristics of the assessed sample of adolescents, comparing students from private and public schools. The three schools were divided into two groups, with regard to private education and public education. Among the assessed students, the majority (65.9%) came from private schools. The mean age of the population was 13.9±2.1 years (n=529), and students of private schools had a higher mean age than those from public school (p<0.001). The sample consisted mostly of females (302; 56.9%), with no difference in gender distribution between private and public schools. With regard to socio-economical class, the difference was significant (p<0.001), with a predominance of class A in private schools and classes B and C in public schools. Sexual maturity showed significant differences (p<0.001), which were compatible with the age difference of the groups, and the daily use of medication was significantly more frequent in the private school students (p=0.003).
Characteristics of the sample of adolescents according to the school type.
| Variables | Public schools | Private schools | p |
|---|---|---|---|
| n | 181 (34.1%) | 350 (65.9%) | |
| Age (years±SD) | 13.2±2.2 (n=180) | 14.4±1.9 (n=349) | <0.001 |
| Gender | |||
| Female (n, %) | 109 (60.2%) | 193 (55.1%) | 0.263 |
| Sleep variables | |||
| CASQ (points±SD) | 38.4±6.7 (n=130) | 38.6±5.6 (n=321) | 0.744 |
| SDSC | |||
| Total (points±SD, n) | 49.5±12.9 (n=124) | 50.4±10.6 (n=316) | 0.496 |
| DIMS (points±SD) | 14.2±4.6 | 14.8±3.6 | 0.204 |
| SBD (points±SD) | 4.8±2 | 4.4±1.8 | 0.057 |
| DA (points±SD) | 4.5±1.5 | 4.2±1.5 | 0.095 |
| SWTD (points±SD) | 11.2±4.3 | 10.6±4 | 0.164 |
| DOES (points±SD) | 11.4±4.6 | 13.2±3.8 | <0.001 |
| SH (points±SD) | 3.4±1.8 | 3.1±1.6 | 0.101 |
| Hours of sleep | |||
| Week (hours±SD) | 7.74±1.57 | 7.31±1.05 | 0.001 |
| Weekend (h±SD) | 8.71±1.50 | 9.02±1.14 | 0.017 |
| Sleep deficit (h±SD) | 0.91±1.67 | 1.71±1.41 | <0.001 |
| Sleep deficit (n, %) | 41 (24.8%) | 158 (45.8%) | <0.001 |
CASQ, Cleveland Adolescent Sleepiness Questionnaire; SDSC, Sleep Disturbance Scale for Children; DIMS, disorder of initiating and maintaining sleep; SBD, sleep breathing disorders; DA, disorders of arousal; SWTD, sleep–wake transition disorder; DOES, disorder of excessive somnolence; SH, sleep hyperhidrosis.
For the CASQ sleepiness questionnaire, the mean value obtained (n=451) was 38.6±6. There was no difference between students from public and private schools: the mean in the public school was 38.4±6.7 and in the private school, 38.6±5.6 (Table 1).
As for the SDSC score, the mean of the total population (n=440) was 50.1±11.3. Considering only the students from public schools, the mean was 49.5±13, and of private schools, 50.4±10.6 and the difference was not statistically significant. However, a higher prevalence of disorders of excessive somnolence (SDSC score) was observed in students from private schools (p<0.001).
Students from public schools had longer time of sleep during the week than their private school peers (p=0.001), and the latter had a longer time of sleep on weekends (p=0.017). As for the sleep pattern, sleep deprivation was considered when sleep deficit was ≥2h. Thus, 199 adolescents (39%) reported a mean of two or more hours of sleep on weekends when compared with the mean number of hours of sleep on weekdays. The sleep deficit for students from the public schools was 0.91h versus 1.71h for private school students (p<0.001), and the percentage of sleep-deprived private school students was higher that observed in public school students (45.8% vs. 24.8%; p<0.001).
There was a statistically significant positive correlation between sleep deficit and age (p<0.001), of moderate degree (r=0.337), showing a gradual increase in sleep deficit as age increased (Fig. 1). When considering age, the value of CASQ increased gradually with age: 36±5.7 for 10-year-olds and 41.3±6.2 for 17-year-olds, showing a correlation between the variables age and the CASQ value (p<0.001) of mild degree (r=0.244). The sample of adolescents aged 18 years was not shown as it was not representative (n=8).

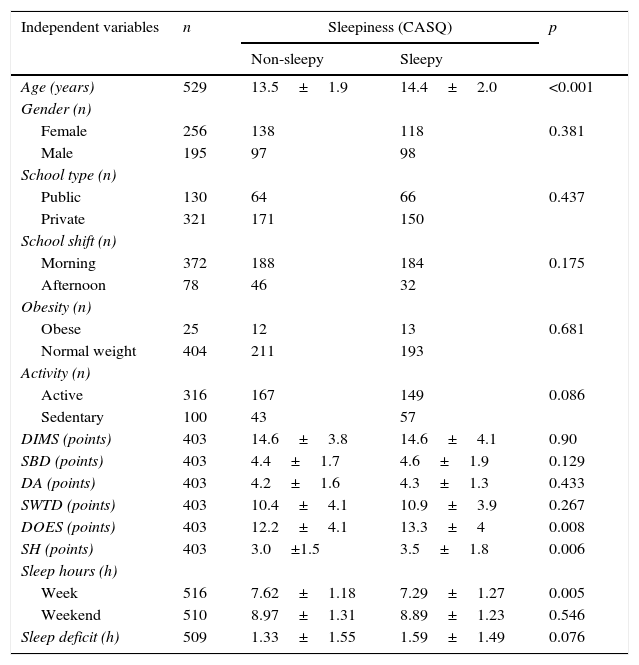
To assess sleepiness, the authors chose to use the CASQ as the dependent variable. The mean score achieved by the students in CASQ, 38 points, was used as the cutoff value for the division between groups with presence or absence of sleepiness. Numerical variables were compared with the six variables that compose the SDSC questionnaire, in addition to the hours of sleep during the week, hours of sleep on weekends, sleep deficit, and age. There was a significant association between higher values of the SDSC questionnaire score for disorders of excessive somnolence (p=0.008) and sleep hyperhidrosis (p=0.006), increased sleep restriction during the week (p=0.005), and older age (p<0.001) in the group with excessive sleepiness. The assessed categorical variables were school (public vs. private), school shift, gender, obesity and physical activity. None of the variables showed significant difference between the two groups (Table 2). The presence of chronic diseases (p=0.34) was not significant.
Comparison of the sample according to sleepiness (CASQ).
| Independent variables | n | Sleepiness (CASQ) | p | |
|---|---|---|---|---|
| Non-sleepy | Sleepy | |||
| Age (years) | 529 | 13.5±1.9 | 14.4±2.0 | <0.001 |
| Gender (n) | ||||
| Female | 256 | 138 | 118 | 0.381 |
| Male | 195 | 97 | 98 | |
| School type (n) | ||||
| Public | 130 | 64 | 66 | 0.437 |
| Private | 321 | 171 | 150 | |
| School shift (n) | ||||
| Morning | 372 | 188 | 184 | 0.175 |
| Afternoon | 78 | 46 | 32 | |
| Obesity (n) | ||||
| Obese | 25 | 12 | 13 | 0.681 |
| Normal weight | 404 | 211 | 193 | |
| Activity (n) | ||||
| Active | 316 | 167 | 149 | 0.086 |
| Sedentary | 100 | 43 | 57 | |
| DIMS (points) | 403 | 14.6±3.8 | 14.6±4.1 | 0.90 |
| SBD (points) | 403 | 4.4±1.7 | 4.6±1.9 | 0.129 |
| DA (points) | 403 | 4.2±1.6 | 4.3±1.3 | 0.433 |
| SWTD (points) | 403 | 10.4±4.1 | 10.9±3.9 | 0.267 |
| DOES (points) | 403 | 12.2±4.1 | 13.3±4 | 0.008 |
| SH (points) | 403 | 3.0±1.5 | 3.5±1.8 | 0.006 |
| Sleep hours (h) | ||||
| Week | 516 | 7.62±1.18 | 7.29±1.27 | 0.005 |
| Weekend | 510 | 8.97±1.31 | 8.89±1.23 | 0.546 |
| Sleep deficit (h) | 509 | 1.33±1.55 | 1.59±1.49 | 0.076 |
CASQ, Cleveland Adolescent Sleepiness Questionnaire; DIMS, disorder of initiating and maintaining sleep; SBD, sleep breathing disorders; DA, disorders of arousal; SWTD, sleep–wake transition disorder; DOES, disorders of excessive somnolence; SH, sleep hyperhidrosis.
When the correlation between the different variables and sleepiness (CASQ) was assessed, there was a positive correlation with disorders of excessive somnolence (r=0.25, p<0.001), sleep hyperhidrosis (r=0.23, p<0.001), age (r=0.24, p<0.001) and sleep deficit (r=0.11, p=0.02). There was a negative correlation between sleepiness and the amount of sleep in hours during the week (r=−0.21, p<0.001) and there was no correlation between sleepiness and amount of sleep on weekends (r=−0, 08, p=0.10).
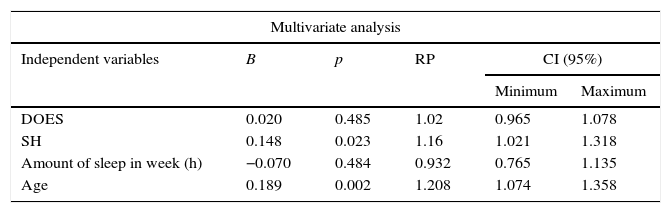
Multivariate logistic regression was performed to investigate the factors associated with sleepiness in adolescents. Statistically significant values indicate the older age of students and higher scores on the SDSC sleep hyperhidrosis variable as factors for worse degree of excessive sleepiness (Table 3).
Factors associated with sleepiness in adolescents in the city of São Paulo, Brazil.
| Multivariate analysis | |||||
|---|---|---|---|---|---|
| Independent variables | B | p | RP | CI (95%) | |
| Minimum | Maximum | ||||
| DOES | 0.020 | 0.485 | 1.02 | 0.965 | 1.078 |
| SH | 0.148 | 0.023 | 1.16 | 1.021 | 1.318 |
| Amount of sleep in week (h) | −0.070 | 0.484 | 0.932 | 0.765 | 1.135 |
| Age | 0.189 | 0.002 | 1.208 | 1.074 | 1.358 |
DOES, disorders of excessive somnolence; SH, sleep hyperhidrosis.
Based on the present results, age and sleep hyperhidrosis had a statistically significant effect on daytime sleepiness in the studied adolescent population. The values found when applying the CASQ in Brazilian adolescents (38.6±6) showed to be slightly higher than those found by Spilsbury et al.16 in the United States at the questionnaire validation (35.2±11) and in 314 Indian adolescents, in whom the mean value obtained was 36±9.22
An alarming finding was that 39% of these adolescents had a sleep deficit greater than 2h and, therefore, were subject to numerous complications of sleep deprivation.23 These sleep deprivation values followed the trend of Portuguese data,24 in which 74% of the assessed individuals slept less than 8h on weekdays and 33% did so on weekends. There is also a direct association between age and daytime sleepiness (Fig. 1). The authors speculate that, with increasing age, the adolescents, despite the little sleep, prioritize social and leisure activities, in addition to losing precious time during displacement in the urban environment.7,25 Also, the finding of increased sleep deficit in private school students appears to be associated with the fact that the private school sample have students mostly attending the morning shift. The importance of sleep deprivation has been demonstrated not only in the West,26 but also in recent data from China,27 where an intervention took place in a primary school with a delay in the start of school activities of 30 and 60min, resulting in better performance of students.
Another associated factor, sleep hyperhidrosis, is a complaint that interferes with the quality of sleep, thus contributing to sleepiness. It can be described in a large number of differential diagnoses, from infectious diseases to neuroendocrine disorders,28 but it is also a very common complaint in patients with OSAS28,29 and other respiratory diseases in childhood.30
The study has limitations due to the absence of sample size calculation, but the linear correlations between age, excessive sleepiness, and sleep deficit (CASQ) with a sample of 450, two-tailed p of 5%, and r=0.37, evidenced a power of 99%. The unbalanced sample between the public and private schools also creates paradoxes in the findings, and may not represent the general Brazilian adolescent population. The sample size without sufficient statistical power to find differences can justify the fact that some associations were not statistically significant. The horizontal study design also does not allow for the determination of the cause-and-effect association, but was enough to show some factors associated with sleepiness in adolescents. Another point is the use of questionnaires, which in addition to not being as sensitive as interviews, has the disadvantage of losses and does not consider the individuality of the population to which they are applied. The CASQ, for instance, was developed for English-speaking adolescents who study full-time. However, this information is not as relevant, considering that over 80% of the present study sample studied in the morning and wake up early. The choice of translating a questionnaire and using it for the first time in the country can also be a limitation; however, the CASQ is one of the best questionnaires to assess sleepiness and the only one that can address the entire age group of this study.
The study conclusion is that excessive sleepiness is related to increasing age; an association with the presence of sleep hyperhidrosis was also observed. Sleep deficit was very frequent in the assessed population of adolescents and, therefore, the effort to develop a better quality of sleep should be primarily focused on better sleep hygiene, thus preventing this population from suffering the damages caused by sleep deprivation from an early age. Future studies should focus on intervention strategies to reduce sleep deprivation.
FundingFundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) – Thiago S. Vilela (Process 2012/20503-4).Associação Fundo de Incentivo à Pesquisa (AFIP) – no process number.
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) – Lia Rita A. Bittencourt (Process 300674 2013-9); Sergio Tufik (Process 301974/2011-0).
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to express their sincere appreciation to the funders of the study, which allowed it to be performed. Additionally, they would like to thank the three schools involved in this study, whose participation was fundamental from the sample selection to the inclusion of the study in their extracurricular activities, encouraging in their students, from an early age, an interest in scientific research. The authors would also like to thank the teachers, coordinators and principals, who gave the access to the target population, and especially to all adolescents who spontaneously answered the questionnaires, thus allowing the study to be carried out.
Please cite this article as: Vilela TS, Bittencourt LR, Tufik S, Moreira GA. Factors influencing excessive daytime sleepiness in adolescents. J Pediatr (Rio J). 2016;92:149–55.




