
To determine the prevalence of current tobacco use and its association with sociodemographic factors and risk behaviors among adolescents and young students, according to gender.
MethodsThe sample consisted of students from the state public school network aged between 12 and 24 years, who answered the Brazilian version of the Youth Risk Behavior Survey questionnaire. The data were analyzed in SPSS software (v. 20.0), using Poisson regression to evaluate the prevalence ratio (PR) of the independent variables in relation to the outcome. p<0.05 was established as the significance level.
ResultsThe final analysis consisted of 1275 adolescents, of whom 716 (56.2%) were girls and 559 (43.8%) were boys. The prevalence of current tobacco use was 6.6% among girls and 9.7% among boys. In females, consuming alcohol in the last 30 days (3.91 [1.54–9.94]) and being 14 years old or younger (0.50 [0.26–0.96]) influenced current tobacco use. In the male gender, tobacco use in the last 30 days was influenced by current alcohol consumption (2.92 [1.21–7.08]) and involvement in physical fighting in the last 12 months (2.32 [1.32–4.09]).
ConclusionAlthough the prevalence of current tobacco use was low in both genders, the assessed population still presents a risk, since male involvement in physical fighting and current consumption of alcohol in both genders increased the probability of this population becoming regular tobacco users.
Determinar a prevalência de uso atual do tabaco e sua associação com fatores sociodemográficos e comportamentos de risco entre adolescentes e jovens escolares, segundo o sexo.
MétodosA amostra foi composta por estudantes da rede estadual entre 12 e 24 anos, que responderam a versão brasileira do questionário Youth Risk Behavior Survey. Os dados foram analisados no SPSS (versão 20.0), por meio da Regressão de Poisson para avaliar a Razão de Prevalência (RP) das variáveis independentes em relação ao desfecho. Foi adotado p < 0,05.
ResultadosA análise final foi composta por 1.275 adolescentes, dos quais 716 (56,2%) eram meninas e 559 (43,8%) meninos. A prevalência de consumo atual do tabaco foi de 6,6% entre as meninas e 9,7% entre os meninos. No sexo feminino, consumir álcool nos últimos 30 dias (3,91 [1,54 – 9,94]) e ter 14 anos ou menos (0,50 [0,26 – 0,96]) influenciaram o uso atual de tabaco. No sexo masculino, o uso de tabaco nos últimos 30 dias foi influenciado pelo consumo atual de álcool (2,92 [1,21 – 7,08]) e envolvimento em luta corporal nos últimos 12 meses (2,32 [1,32 – 4,09]).
ConclusãoEmbora a prevalência de consumo atual do tabaco tenha sido baixa em ambos os sexos, a população estudada ainda exibe risco, pois o envolvimento em luta corporal no sexo masculino e o consumo atual de álcool em ambos os sexos aumentaram a probabilidade da população se envolver com uso atual do tabaco.
Adolescents and young adults comprise a significant part of the population, totaling approximately 1.8 billion individuals between the ages of 10 and 24 years worldwide.1 The transformations that take place during adolescence involve biological and sociocultural aspects, which make this population a group that is more susceptible to change and experimentation. Thus, the influence of factors such as tobacco, alcohol, sex, drugs, and diet can have negative impacts on health.2
Tobacco ranks second among the substances most consumed by adolescents and young adults, being second only to alcohol.3 According to data from the last Youth Risk Behavior Survey (YRBS) carried out in the United States in 2017, the prevalence of adolescents who have tried cigarette smoking at some point in life was 28.9%.4 National data from the Cardiovascular Risk Study in Adolescents (Estudo de Riscos Cardiovasculares em Adolescentes [ERICA]), carried out in 2013–2014 with students aged 12–17 years, show that 18.8% of boys and 18.3% of girls have already experimented tobacco.5
Exposure to tobacco has several implications for adolescent health, such as respiratory conditions, oral pathologies, and decreased physical capacity.6 Therefore, this population deserves special attention because, in addition to being more vulnerable to the tobacco industry, they also have a higher risk of chemical addiction due to early exposure to nicotine.7 However, health care should also extend to young adults aged 19–24 years, as the transition to adulthood is almost consolidated and the chances that smoking will persist into adulthood increase considerably.8
Studies have shown that tobacco use by adolescents is associated with other risk behaviors, such as the consumption of alcohol and other drugs,9,10 early sexual activity, multiple sexual partners and inconsistent condom use,11 violent behavior,12,13 mental health problems,14 and suicide ideation.15
Due to the greater vulnerability related to tobacco use in adolescence and the negative effects tobacco use has on the health of adolescents and young adults, knowing the prevalence and the factors that permeate this behavior is fundamental, since the habits acquired at this age range can persist into adulthood. It is expected that the results of the present study will help identify groups at risk and serve as a reference subsidy to guide strategies and policies aiming to promote and protect the health of adolescents and young adults.
It is worth mentioning that the development of studies aiming to investigate this subject is important for the Northeast of Brazil, especially in the countryside, where investigations are scarce. Therefore, the aim of the study was to verify the prevalence of current tobacco use and its association with sociodemographic, economic factors, and risk behaviors among adolescents and young students from the municipality of Petrolina, state of Pernambuco, Brazil, according to gender.
MethodsThis was an epidemiological, school-based study with a cross-sectional design,16 carried out in elementary and high schools of the state public school network of the municipality of Petrolina, from March to July 2014, after approval by the Research Ethics Committee of the Universidade de Pernambuco under CAAE: 24288213.2.0000.5207. The research complied with all the provisions of Resolution 466/12 of the National Health Council, and the guidelines of the Brazilian Child and Adolescent Statute.
The studied population consisted of adolescents and young adults (aged 12–24 years) who attended the aforementioned public schools. The authors considered a total population of 25,635 students in the elementary and high schools of the state public school network of Petrolina.
The inclusion criteria for study participation were as follows: be an adolescent or young adult, of both genders; be properly enrolled in elementary or high school institutions located in the urban area of the municipality of Petrolina that were included in the study; know how to read and write in Portuguese.
Adolescents with a medical diagnosis of neurological pathologies or alterations in physical, behavioral, and/or psychological status that made it impossible for them to fill out the data collection tool and those who did not correctly answered the questionnaire were excluded from the study.
The distribution was made according to school size and the students’ enrollment period, aiming to guarantee the sample proportionality. The schools were classified into three categories: small (less than 200 students); medium-sized (200–499 students); and large (500 students or more).16 Students enrolled in the morning and afternoon periods were grouped into a single category (daytime students).
The random sampling procedure was used to select the sample, with two-stage cluster sampling, in which “school” and “class” represented the sample units, respectively, in the first and second moments. All 29 schools in the state public school network of the urban area of Petrolina were considered eligible for study inclusion. After all the stages, the total number of nine elementary and high schools selected was reached, representing 31.03% of the state schools in the municipality of Petrolina.
The WinPepi program (WinPepi program (PEPI-for-Windows: computer programs for epidemiologists) was used for sample quantification; considering a population of 25,635 students, a 95% confidence interval, maximum tolerable error of 5%, and sample loss of 20%; the estimated prevalence was 50% and the design effect was 2.0, totaling 948 adolescents. A minimum of 17 students per class was considered; thus, 1326 adolescents were assessed.
The Brazilian version of the Youth Risk Behavior Survey (YRBS) was used to assess risk behaviors. This tool was developed by the Centers for Disease Control and Prevention (CDC) and applied every two years to representative samples of students from all over the United States, aiming to monitor health risk behaviors among adolescents and young adults.4 The questionnaire consists of 87 questions subdivided into six domains related to risk behaviors: (1) unintentional injuries and violence; (2) use of tobacco; (3) consumption of alcoholic beverages and other drugs; (4) sexual behavior directed at unwanted pregnancies and sexually-transmitted diseases; (5) eating habits; and (6) practice of physical activity.4
The validation of the Brazilian version was performed by Guedes and Lopes17 and showed a Kappa agreement index between moderate and significant with a mean value of 68.6%, indicating the quality of the psychometric properties of the YRBS-2007. The following domains of the questionnaire were used for this study: tobacco use (kappa: 64.9–86.4); unintentional injuries and violence (kappa: 43.6–100); alcoholic beverages (kappa: 49.4–66.7); physical activity (kappa: 37.2–79).
The questions used were: current tobacco use, cigarette smoking in the last 30 days, cigarette experimentation, age when you started cigarette smoking, smoking cigarettes at school in the last 30 days, number of cigarettes smoked a day in the past 30 days, how you obtained cigarettes in the last 30 days, daily cigarette smoking, attempt to quit smoking in the last 12 months, feeling excessively sad almost every day for two or more weeks in the last 12 months, suicide ideation/planning/attempt in the last 12 months, involvement in physical fighting in the last 12 months, alcohol consumption in the last 30 days, having gotten drunk in the last 30 days, and being physically active in the last seven days.
Aiming to test the tool's applicability, make corrections, and identify possible biases and limitations when performing the research, a pilot study was carried out at a school in the state public school network of elementary and high schools of Petrolina, with a sample of 80 adolescents.
The data were processed in the Microsoft Excel program (Microsoft®, WA, USA) with double entry of data and analyzed using SPSS, (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY, USA). Descriptive statistics were initially performed, presenting the absolute and relative frequencies of the analyzed variables, whereas the prevalence rates were estimated with their respective 95% CIs. The possible associations between the independent variables and the outcome (current use of tobacco) were calculated using Pearson's chi-squared test or Fisher's exact test.
The variables that showed a significance level of p≤0.20 in the chi-squared test were included in the Poisson regression analysis with robust variance stratified by gender, and the prevalence ratios used in the crude and adjusted analyses were calculated, remaining in the analysis only the variables that were associated with the outcome with a p-value <0.05.
ResultsOf the 1326 adolescents who took part in the study, 51 were excluded because their questionnaires contained filling errors; therefore, 1275 adolescents were included in the final analysis. The sample consisted of 716 (56.2%) girls and 559 (43.8%) boys. Most of the study population was aged between 15 and 24 years old, self-reported their ethnicity as mixed-race, declared that they had a religion, were single, and had no children. Regarding the information about parents’ level of schooling and monthly family income, it was verified that 18.3% (n=222) of the students did not know about the maternal level of schooling, 27.3% (n=330) did not know about the paternal level of schooling, and 34.1% (n=392) did not know the monthly family income.
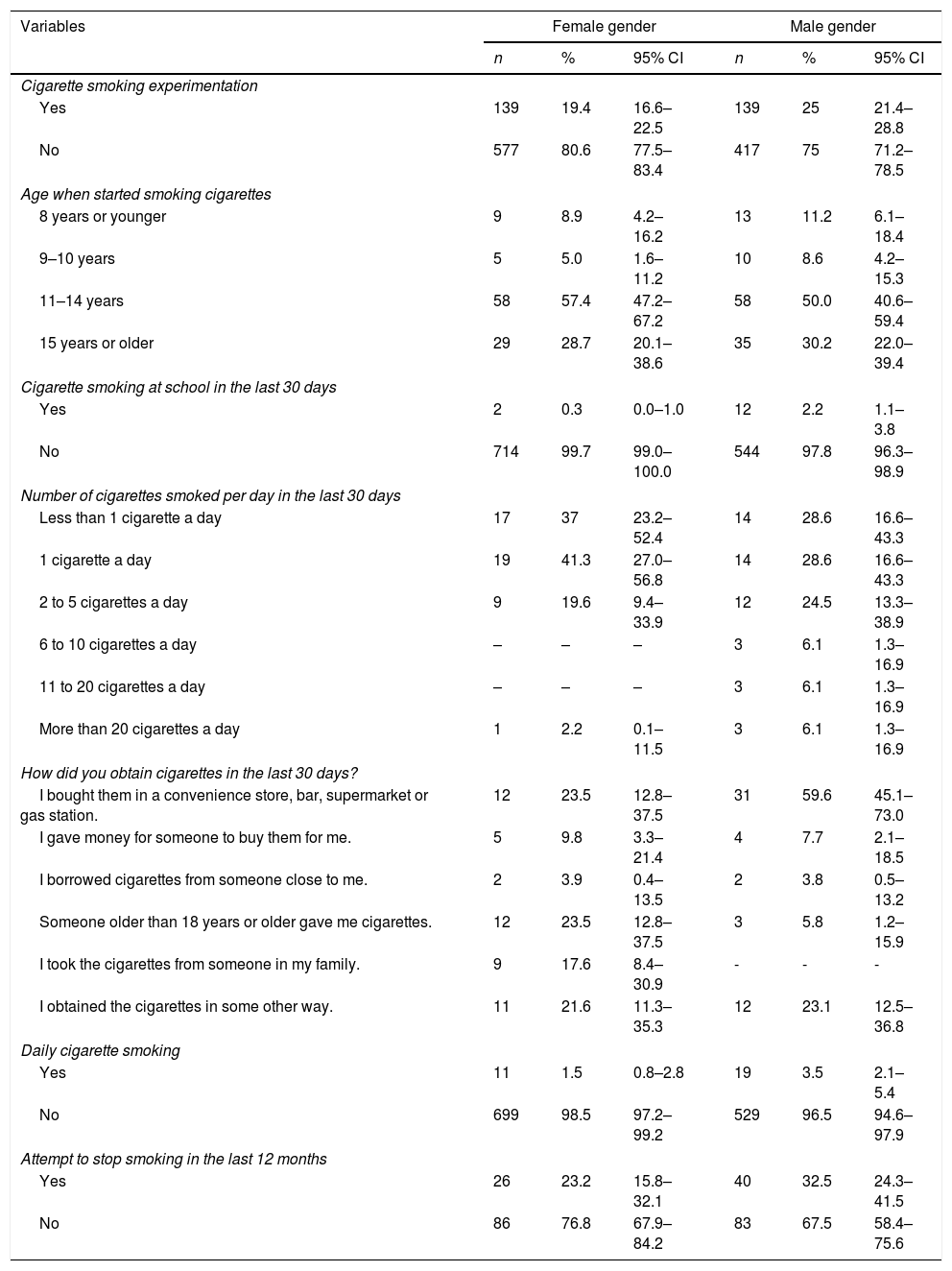
Table 1 shows the variables related to tobacco use, according to the adolescents’ gender. It is worth mentioning that the questions refer to tobacco consumption at some point in life, meaning the adolescent did not necessarily maintain the habit of smoking. It was verified that only 7.9% (n=101) of the sample reported having smoked in the last 30 days. Of these, 54 (9.7% [95% CI: 7.34–12.42]) were males and 47 (6.6% [95% CI: 4.86–8.63]) were females. The prevalence of cigarette experimentation, current, and daily consumption of cigarettes were similar in relation to the gender of the adolescents; however, the consumption of cigarettes in the last 30 days at school was higher among boys. The most prevalent age group in both genders for the start of cigarette smoking was 11–14 years, and more than 50% of the sample started the habit before 15 years of age. The most frequently reported manner to obtain cigarettes was to purchase them at convenience stores, bars, supermarkets, or gas stations. Moreover, most students reported they did not try to quit smoking in the last year.
Distribution of tobacco consumption among adolescents and young adults. Petrolina – PE, Brazil, 2014.
| Variables | Female gender | Male gender | ||||
|---|---|---|---|---|---|---|
| n | % | 95% CI | n | % | 95% CI | |
| Cigarette smoking experimentation | ||||||
| Yes | 139 | 19.4 | 16.6–22.5 | 139 | 25 | 21.4–28.8 |
| No | 577 | 80.6 | 77.5–83.4 | 417 | 75 | 71.2–78.5 |
| Age when started smoking cigarettes | ||||||
| 8 years or younger | 9 | 8.9 | 4.2–16.2 | 13 | 11.2 | 6.1–18.4 |
| 9–10 years | 5 | 5.0 | 1.6–11.2 | 10 | 8.6 | 4.2–15.3 |
| 11–14 years | 58 | 57.4 | 47.2– 67.2 | 58 | 50.0 | 40.6–59.4 |
| 15 years or older | 29 | 28.7 | 20.1–38.6 | 35 | 30.2 | 22.0–39.4 |
| Cigarette smoking at school in the last 30 days | ||||||
| Yes | 2 | 0.3 | 0.0–1.0 | 12 | 2.2 | 1.1–3.8 |
| No | 714 | 99.7 | 99.0–100.0 | 544 | 97.8 | 96.3–98.9 |
| Number of cigarettes smoked per day in the last 30 days | ||||||
| Less than 1 cigarette a day | 17 | 37 | 23.2–52.4 | 14 | 28.6 | 16.6–43.3 |
| 1 cigarette a day | 19 | 41.3 | 27.0–56.8 | 14 | 28.6 | 16.6–43.3 |
| 2 to 5 cigarettes a day | 9 | 19.6 | 9.4–33.9 | 12 | 24.5 | 13.3–38.9 |
| 6 to 10 cigarettes a day | – | – | – | 3 | 6.1 | 1.3–16.9 |
| 11 to 20 cigarettes a day | – | – | – | 3 | 6.1 | 1.3–16.9 |
| More than 20 cigarettes a day | 1 | 2.2 | 0.1–11.5 | 3 | 6.1 | 1.3–16.9 |
| How did you obtain cigarettes in the last 30 days? | ||||||
| I bought them in a convenience store, bar, supermarket or gas station. | 12 | 23.5 | 12.8–37.5 | 31 | 59.6 | 45.1–73.0 |
| I gave money for someone to buy them for me. | 5 | 9.8 | 3.3–21.4 | 4 | 7.7 | 2.1–18.5 |
| I borrowed cigarettes from someone close to me. | 2 | 3.9 | 0.4–13.5 | 2 | 3.8 | 0.5–13.2 |
| Someone older than 18 years or older gave me cigarettes. | 12 | 23.5 | 12.8–37.5 | 3 | 5.8 | 1.2–15.9 |
| I took the cigarettes from someone in my family. | 9 | 17.6 | 8.4–30.9 | - | - | - |
| I obtained the cigarettes in some other way. | 11 | 21.6 | 11.3–35.3 | 12 | 23.1 | 12.5–36.8 |
| Daily cigarette smoking | ||||||
| Yes | 11 | 1.5 | 0.8–2.8 | 19 | 3.5 | 2.1–5.4 |
| No | 699 | 98.5 | 97.2–99.2 | 529 | 96.5 | 94.6–97.9 |
| Attempt to stop smoking in the last 12 months | ||||||
| Yes | 26 | 23.2 | 15.8–32.1 | 40 | 32.5 | 24.3–41.5 |
| No | 86 | 76.8 | 67.9–84.2 | 83 | 67.5 | 58.4–75.6 |
Note: The total number may be different due to missing values.
95% CI, 95% confidence interval.
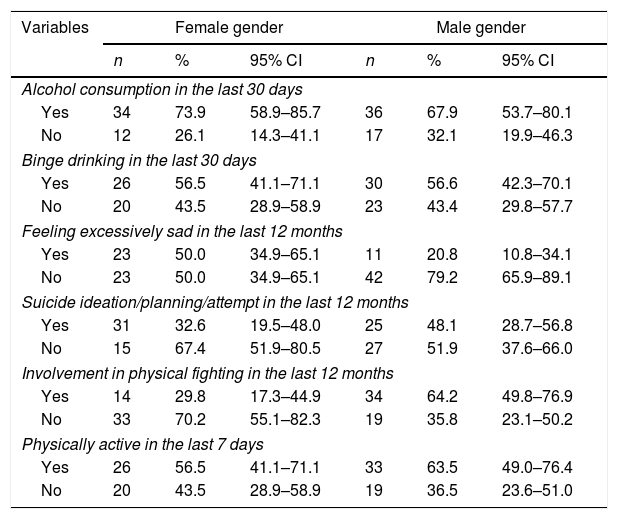
Table 2 shows the prevalence rates of risk behaviors among the students who used tobacco, according to the gender of adolescents. It can be observed that the most prevalent behavior among girls and boys was alcohol consumption in the last 30 days.
Distribution of risk behaviors among adolescents and young adults with current tobacco use according to gender. Petrolina – PE, Brazil, 2014.
| Variables | Female gender | Male gender | ||||
|---|---|---|---|---|---|---|
| n | % | 95% CI | n | % | 95% CI | |
| Alcohol consumption in the last 30 days | ||||||
| Yes | 34 | 73.9 | 58.9–85.7 | 36 | 67.9 | 53.7–80.1 |
| No | 12 | 26.1 | 14.3–41.1 | 17 | 32.1 | 19.9–46.3 |
| Binge drinking in the last 30 days | ||||||
| Yes | 26 | 56.5 | 41.1–71.1 | 30 | 56.6 | 42.3–70.1 |
| No | 20 | 43.5 | 28.9–58.9 | 23 | 43.4 | 29.8–57.7 |
| Feeling excessively sad in the last 12 months | ||||||
| Yes | 23 | 50.0 | 34.9–65.1 | 11 | 20.8 | 10.8–34.1 |
| No | 23 | 50.0 | 34.9–65.1 | 42 | 79.2 | 65.9–89.1 |
| Suicide ideation/planning/attempt in the last 12 months | ||||||
| Yes | 31 | 32.6 | 19.5–48.0 | 25 | 48.1 | 28.7–56.8 |
| No | 15 | 67.4 | 51.9–80.5 | 27 | 51.9 | 37.6–66.0 |
| Involvement in physical fighting in the last 12 months | ||||||
| Yes | 14 | 29.8 | 17.3–44.9 | 34 | 64.2 | 49.8–76.9 |
| No | 33 | 70.2 | 55.1–82.3 | 19 | 35.8 | 23.1–50.2 |
| Physically active in the last 7 days | ||||||
| Yes | 26 | 56.5 | 41.1–71.1 | 33 | 63.5 | 49.0–76.4 |
| No | 20 | 43.5 | 28.9–58.9 | 19 | 36.5 | 23.6–51.0 |
Note: The total number may be different due to missing values.
95% CI, 95% confidence interval.
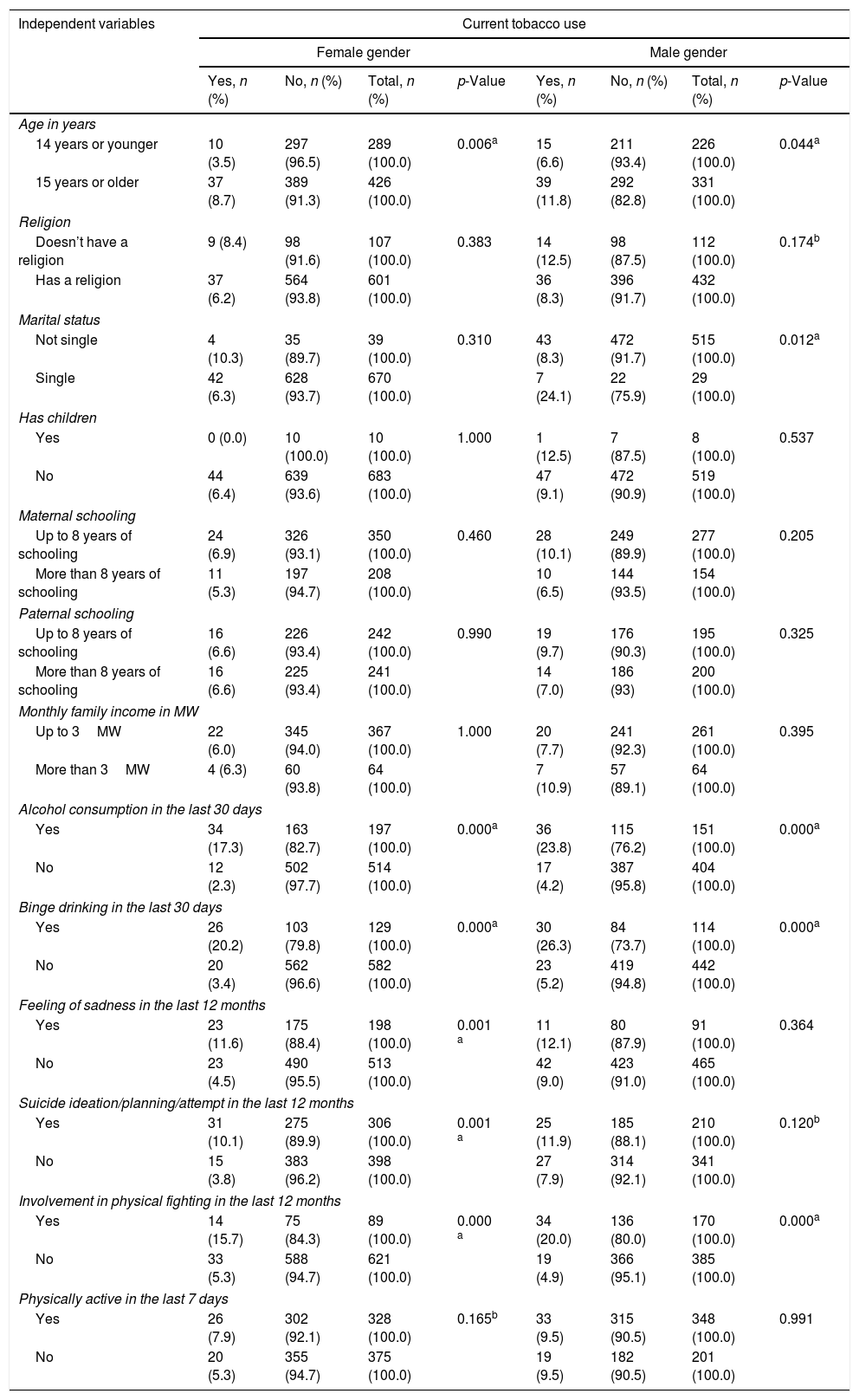
Table 3 shows the chi-squared test according to the gender of the adolescents. For the regression model of the female gender, the variables age in years, alcohol consumption in the last 30 days, binge drinking in the last 30 days, feeling sad in the last 12 months, suicide ideation/planning/attempt in the last 12 months, involvement in physical fighting in the last 12 months, and being physically active in the last seven days were selected, because they showed p≤0.20.
Association between current tobacco consumption and the independent variables assessed in adolescents and young adults, according to gender. Petrolina – PE, Brazil, 2014.
| Independent variables | Current tobacco use | |||||||
|---|---|---|---|---|---|---|---|---|
| Female gender | Male gender | |||||||
| Yes, n (%) | No, n (%) | Total, n (%) | p-Value | Yes, n (%) | No, n (%) | Total, n (%) | p-Value | |
| Age in years | ||||||||
| 14 years or younger | 10 (3.5) | 297 (96.5) | 289 (100.0) | 0.006a | 15 (6.6) | 211 (93.4) | 226 (100.0) | 0.044a |
| 15 years or older | 37 (8.7) | 389 (91.3) | 426 (100.0) | 39 (11.8) | 292 (82.8) | 331 (100.0) | ||
| Religion | ||||||||
| Doesn’t have a religion | 9 (8.4) | 98 (91.6) | 107 (100.0) | 0.383 | 14 (12.5) | 98 (87.5) | 112 (100.0) | 0.174b |
| Has a religion | 37 (6.2) | 564 (93.8) | 601 (100.0) | 36 (8.3) | 396 (91.7) | 432 (100.0) | ||
| Marital status | ||||||||
| Not single | 4 (10.3) | 35 (89.7) | 39 (100.0) | 0.310 | 43 (8.3) | 472 (91.7) | 515 (100.0) | 0.012a |
| Single | 42 (6.3) | 628 (93.7) | 670 (100.0) | 7 (24.1) | 22 (75.9) | 29 (100.0) | ||
| Has children | ||||||||
| Yes | 0 (0.0) | 10 (100.0) | 10 (100.0) | 1.000 | 1 (12.5) | 7 (87.5) | 8 (100.0) | 0.537 |
| No | 44 (6.4) | 639 (93.6) | 683 (100.0) | 47 (9.1) | 472 (90.9) | 519 (100.0) | ||
| Maternal schooling | ||||||||
| Up to 8 years of schooling | 24 (6.9) | 326 (93.1) | 350 (100.0) | 0.460 | 28 (10.1) | 249 (89.9) | 277 (100.0) | 0.205 |
| More than 8 years of schooling | 11 (5.3) | 197 (94.7) | 208 (100.0) | 10 (6.5) | 144 (93.5) | 154 (100.0) | ||
| Paternal schooling | ||||||||
| Up to 8 years of schooling | 16 (6.6) | 226 (93.4) | 242 (100.0) | 0.990 | 19 (9.7) | 176 (90.3) | 195 (100.0) | 0.325 |
| More than 8 years of schooling | 16 (6.6) | 225 (93.4) | 241 (100.0) | 14 (7.0) | 186 (93) | 200 (100.0) | ||
| Monthly family income in MW | ||||||||
| Up to 3MW | 22 (6.0) | 345 (94.0) | 367 (100.0) | 1.000 | 20 (7.7) | 241 (92.3) | 261 (100.0) | 0.395 |
| More than 3MW | 4 (6.3) | 60 (93.8) | 64 (100.0) | 7 (10.9) | 57 (89.1) | 64 (100.0) | ||
| Alcohol consumption in the last 30 days | ||||||||
| Yes | 34 (17.3) | 163 (82.7) | 197 (100.0) | 0.000a | 36 (23.8) | 115 (76.2) | 151 (100.0) | 0.000a |
| No | 12 (2.3) | 502 (97.7) | 514 (100.0) | 17 (4.2) | 387 (95.8) | 404 (100.0) | ||
| Binge drinking in the last 30 days | ||||||||
| Yes | 26 (20.2) | 103 (79.8) | 129 (100.0) | 0.000a | 30 (26.3) | 84 (73.7) | 114 (100.0) | 0.000a |
| No | 20 (3.4) | 562 (96.6) | 582 (100.0) | 23 (5.2) | 419 (94.8) | 442 (100.0) | ||
| Feeling of sadness in the last 12 months | ||||||||
| Yes | 23 (11.6) | 175 (88.4) | 198 (100.0) | 0.001 a | 11 (12.1) | 80 (87.9) | 91 (100.0) | 0.364 |
| No | 23 (4.5) | 490 (95.5) | 513 (100.0) | 42 (9.0) | 423 (91.0) | 465 (100.0) | ||
| Suicide ideation/planning/attempt in the last 12 months | ||||||||
| Yes | 31 (10.1) | 275 (89.9) | 306 (100.0) | 0.001 a | 25 (11.9) | 185 (88.1) | 210 (100.0) | 0.120b |
| No | 15 (3.8) | 383 (96.2) | 398 (100.0) | 27 (7.9) | 314 (92.1) | 341 (100.0) | ||
| Involvement in physical fighting in the last 12 months | ||||||||
| Yes | 14 (15.7) | 75 (84.3) | 89 (100.0) | 0.000 a | 34 (20.0) | 136 (80.0) | 170 (100.0) | 0.000a |
| No | 33 (5.3) | 588 (94.7) | 621 (100.0) | 19 (4.9) | 366 (95.1) | 385 (100.0) | ||
| Physically active in the last 7 days | ||||||||
| Yes | 26 (7.9) | 302 (92.1) | 328 (100.0) | 0.165b | 33 (9.5) | 315 (90.5) | 348 (100.0) | 0.991 |
| No | 20 (5.3) | 355 (94.7) | 375 (100.0) | 19 (9.5) | 182 (90.5) | 201 (100.0) | ||
Chi-squared test.
Note: The total number may be different due to missing values.
MW, minimum wages.
The variables that showed p≤0.20 in the male gender and entered the regression analysis were age in years, religion, marital status, alcohol consumption in the last 30 days, binge drinking in the last 30 days, suicide ideation/planning/attempt in the last 12 months, and involvement in physical fighting in the last 12 months.
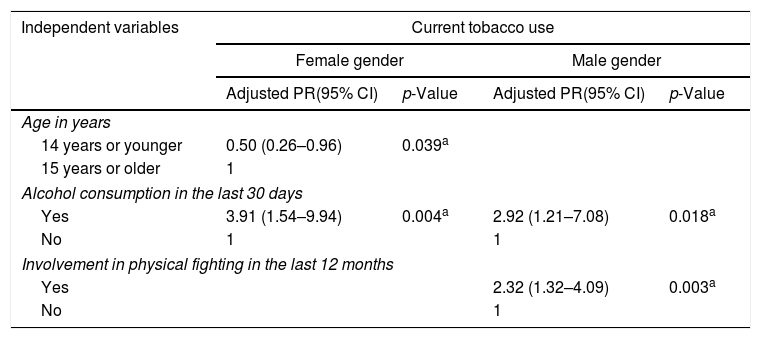
Table 4 depicts Poisson regression, showing the independent variables that remained associated with current tobacco use, after being stratified by gender. The variables that remained associated in the final model for the female gender were age of 14 years or younger and alcohol consumption in the last 30 days, whereas in the final model for the male gender they were alcohol consumption in the last 30 days, and involvement in physical fighting. The statistical model validity was observed, with a significant Omnibus test value in the analyses (p<0.001).
Poisson regression between current tobacco consumption and the independent variables stratified by the gender of adolescents and young adults. Petrolina – PE, Brazil, 2014.
| Independent variables | Current tobacco use | |||
|---|---|---|---|---|
| Female gender | Male gender | |||
| Adjusted PR(95% CI) | p-Value | Adjusted PR(95% CI) | p-Value | |
| Age in years | ||||
| 14 years or younger | 0.50 (0.26–0.96) | 0.039a | ||
| 15 years or older | 1 | |||
| Alcohol consumption in the last 30 days | ||||
| Yes | 3.91 (1.54–9.94) | 0.004a | 2.92 (1.21–7.08) | 0.018a |
| No | 1 | 1 | ||
| Involvement in physical fighting in the last 12 months | ||||
| Yes | 2.32 (1.32–4.09) | 0.003a | ||
| No | 1 | |||
95% CI, 95% confidence interval; PR, prevalence ratio.
Reference variable: Current tobacco use.
Variables with p<0.20 that remained in the regression model, according to gender.
The prevalence of current tobacco use was 9.7% in males and 6.6% in females, with no difference regarding the socioeconomic profile and consumption between the genders. Current alcohol consumption influenced the current use of tobacco in both genders; involvement in physical fighting increased the likelihood of tobacco use in the last 30 days in males, whereas being 14 years or younger reduced this probability in females. However, these data should be analyzed with caution, as it is not possible to establish the causality for these findings with a cross-sectional study.
Thus, it is worth highlighting the importance of the present study concerning the description of smoking in the population of adolescents and young adults. The prevalence of current tobacco use among boys observed in this study was higher than that reported in the last Brazilian National Survey of School Health (Pesquisa Nacional de Saúde do Escolar [PeNSE]) among 9th grade students18 and in the last survey carried out through ERICA with students aged 12–17 years,5 which showed that percentages for males were only 5.8% (95% CI: 5.4–6.3) and 6.0% (95% CI: 5.5–6.7), respectively. However, the prevalence observed in the present study for the female gender is similar to the results found in these national surveys, in which 5.4% (95% CI: 4.9–5.8) of 9th grade female students currently used tobacco in the PeNSE survey and 5.3% (95% CI: 4.8–5.8) in the ERICA survey.
Tobacco smoking in adolescence is closely related to the environment in which the adolescent lives, being for the most part socially and culturally determined.19 Therefore, it is possible to explain the higher prevalence of current tobacco use in male adolescents found in the current study when compared to the other national surveys, because socially, some risk behaviors, such as tobacco use and alcohol consumption, are more often tolerated or even encouraged in males at an early age than in females in the countryside of the Northeast region of Brazil. Although adolescents have a variable pattern of consumption,5 gender is a factor that can interfere with the consumption, the reasons, and the pattern of use of these substances. The historical, familial, cultural, and social contexts establish different patterns of contact with psychoactive substances in each of the genders, and this is associated with the factors involved in the historical construction of the concepts and social models of masculine and feminine behaviors.20
The proportions of tobacco experimentation found according to gender in the current study were higher than those found in a study carried out in the northeast region, which showed values of 15.7% (95% CI: 13.7–18.0) and 14.6% (95% CI: 13.3–16.0) in boys and girls, respectively.5 Not all adolescents and young individuals who try cigarettes become smokers, but experimentation is the first step toward future adherence to regular tobacco use.21
The majority of the sample started smoking before the age of 15, as corroborated by other studies.22,23 These results constitute a matter of concern, because although initially the sensation of taking a pull from a cigarette may be unpleasant, there is an adaptation to the taste after the experimentation and the sensation of pleasure appears, encouraging a new experience with the drug,24 and the earlier the first contact with tobacco is registered, the greater the chance of adolescents becoming addicted to nicotine.7
These findings indicate that the anti-smoking policies employed in the country remain important, but it reveals the need for actions directed at the studied public, since even with the measures aimed at reducing smoking, they tend to be more effective or better applied in the capitals and large urban centers, making adolescents from the countryside more vulnerable. Compliance with the laws that restrict the sale and consumption of cigarettes, increasing the legal age for buying tobacco products, promoting healthy lifestyles, including the family in smoking prevention programs, increasing the price, implementing anti-smoking programs in the school environment, and guaranteeing treatment for smokers are some of the actions that could be adopted.25
Regarding risk behaviors, alcohol consumption in the last 30 days was the most prevalent behavior among students who reported current tobacco use, and it was the factor that increased the probability for current tobacco use for both boys (PR=2.92) and girls (PR=3.91), suggesting that these behaviors are similar, regardless of gender. This finding corroborates the data found by other authors.9,10
In a study carried out by Elicker et al.,23 it was observed that alcohol consumption in the last 30 days increased the probability of students from Porto Velho, state of Rondônia, Brazil of becoming regular tobacco users by approximately 6.7-fold. The coexistence of these risk behaviors is due to the multiplier effect that the consumption of psychoactive substances is capable of producing, in which the use of one substance increases the risk of consumption of others.26 Another factor that explains the association between alcohol consumption and tobacco use is the easy access to these licit drugs in places where adolescents can usually be found, such as parties, bars, or in their own homes.27 Thus, the existence of places where young individuals can go to consume such drugs without detection, will expose them to the consumption of other substances, as well as involvement with other problematic behaviors.11
In the present study, involvement in physical fighting in the last 12 months differed between the genders, being a more prevalent behavior among boys who currently used tobacco than among girls. Kelishadi et al.12 developed a survey with students from Iran and found that involvement in physical fighting increases the chances of being an active smoker. Another study carried out with schoolchildren in South Africa concluded that nicotine dependence is associated with high levels of violence in adolescents.11 The association between physical fighting and tobacco can be explained by the fact that the consumption of psychoactive substances results in a stimulating effect that makes adolescents more aggressive and gets them more involved in situations of violence.28 However, due to the study design, it is not possible to infer the causality between the variables smoking and physical fighting.
In the present study, the association between physical fighting and current tobacco use was found only in males. This can be explained by the fact that violent behaviors are more socially acceptable in males, thus because boys do not perceive a strong deterrent and because they feel that violence is a tolerable behavior, they become more involved in fights.29
One factor that reduced the likelihood of girls getting involved with current tobacco use was being 14 years of age or younger. Malbergier et al.30 found that male adolescents aged between 13 and 18 years were more likely to consume alcohol, tobacco, and illicit drugs, than those between the ages of 10 and 12, but the situation was observed in females only regarding the consumption of alcohol and illicit drugs. Usually, tobacco consumption increases with age5,9,15,19 i.e., younger ages confer a protective factor on recent tobacco use, regardless of the adolescents’ gender.31
The information obtained in this study is relevant, because it depicts the local reality and can be used as a parameter for comparison with studies developed with adolescents and young adults from other places. Moreover, it indicates the need to develop further studies on the subject, mainly in the countryside of the Northeast of Brazil. Also, it can be used as a reference for the development of strategies in programs that aim at health actions at school, such as the School Health Program, a national policy created with the aim of bringing health closer to the education environment and promoting a population of healthier schoolchildren.32
However, the obtained data should be considered with caution, given the limitations associated to a population restricted to students from public schools in a city in the countryside of the state of Pernambuco, which may not correspond to the reality of adolescents who do not attend school, who usually are the most vulnerable, and of schoolchildren from other locations. Another limitation refers to the fact that a self-applied tool was used, which may contain information biases. In addition, the questionnaire does not provide information about other situations that may influence tobacco consumption, such as consumption by parents, peers and friends, and the relationships in the family and work environments, among others.
Moreover, some variables of the population were impaired by the loss of information about the adolescents and the low prevalence of the outcome in some subgroups, thus reducing the power to detect associations. Because this is a cross-sectional study, it is impossible to determine the causality of the evaluated risk behaviors.33,34 Thus, it is suggested that studies with a longitudinal design be carried out to analyze students from private and public schools, adolescents, and young adults living in the state capital and in the countryside. Future studies will help increase the knowledge on the topic, elucidate the profile of the population at risk, and guide educational and health actions aimed at the population of adolescents and young adults.
FundingThis study was funded by the Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco (FACEPE).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Cunha SB, Araújo RC, Oliveira JV, Mola R, Pitangui AC. Factors associated with current tobacco use among adolescents and young students. J Pediatr (Rio J). 2020;96:447–55.





