

To investigate the association between oral contraceptive use and cardiovascular risks, including metabolic syndrome and their components in Brazilian adolescents.
MethodThis study used data from the Study of Cardiovascular Risks in Adolescents (Estudo de Riscos Cardiovasculares em Adolescentes - ERICA), a nationwide, cross-sectional, school-based study with individuals aged 12-17 years. Sociodemographic variables and OC use were assessed by a self-administered questionnaire. International Diabetes Federation criteria were used to define metabolic syndrome. Descriptive statistics were reported as prevalence and their respective confidence interval of 95% of oral contraceptives according to variables. Logistic regression was performed. Crude and adjusted odds ratios were calculated.
ResultsThis subsample was composed of 22,682 female adolescents, of which 12.65% reported using oral contraceptives and their use was associated with hypertension and hypertriglyceridemia. These associations remained statistically significant after adjusting for age, school region, race, and tobacco use with an increase of 2.68 (1.66 – 4.32) and 3.45 (2.56 – 4.65) times, respectively.
ConclusionThe present study was the first to examine the association between the use of oral contraceptives and cardiovascular risk factors among the largest number of female Brazilian adolescents. This method was significantly associated with hypertension, hypertriglyceridemia. Teenagers using oral contraceptives should be monitored for side effects, including blood pressure measurements and advised to avoid smoking.
The use of the first oral contraceptive (OCs) formulation, in the 1960s, was associated with an increase in the rates of cardiovascular events, especially venous thromboembolism, myocardial infarction, and stroke in premenopausal adult women. Since then, there have been significant changes in the doses and types of hormones used in order to reduce the adverse cardiovascular and metabolic effects caused by these drugs,1 nevertheless, until today there are some reports about the increased risk of these potentially life-threatening vascular experiences in this population.2–5 In adolescents, such outcomes are not observed, however, metabolic changes and risk factors for unwanted future cardiovascular events have been reported, particularly increased blood pressure and dyslipidemia.6–9 Besides that, frequently the beginning of undesirable lifestyle behaviors with risk of cardiovascular diseases such as smoking occur before adulthood.10
Epidemiological data on OCs use during adolescence in Brazil estimated a prevalence of around 25% at the last sexual intercourse.11 In addition to protection against unintended pregnancy, OCs are usually prescribed to this population because confer significant non-contraceptive benefits, like an improvement on heavy menstrual bleeding, dysmenorrhea, cycle regularity, acne, hirsutism, and premenstrual symptom.12,13
There are few contraindications on recommendations for contraceptive use in healthy female non-pregnant adolescents. Considering known preexisting medical conditions, OCs should not be prescribed for teenagers with severe and uncontrolled hypertension or thrombophilia, for example. Smoking is not a contraindication to OC use in adolescents, although it should be discouraged.12,14
In Brazil, multiple cardiovascular and metabolic risk factors during adolescence were accessed previously with a nationwide study. Prevalence of metabolic syndrome (MetS) in Brazilian adolescents was equal to 2.6%, using the International Diabetes Federation (IDF)’s criteria,15 and prevalence of hypertension was 9.6%.16
The aim of the present study was to investigate the association between OC use and cardiovascular risks, including MetS and their components in Brazilian adolescents.
MethodsThis study used data from the Study of Cardiovascular Risks in Adolescents (Estudo de Riscos Cardiovasculares em Adolescentes - ERICA). This was a nationwide, cross-sectional, school-based study with individuals aged 12-17 years, representative of the group of adolescents enrolled in schools in municipalities with more than 100,000 inhabitants at the national and regional level, and of each capital and the Federal District. A detailed description of the sample design has been previously published.17
For the present study, the sample consisted of girls between 12 and 17 years of age who attended schools in the morning shift located in all five Brazilian macroregions. The exclusion criteria comprised pregnant adolescents, those with any disability and those whose anthropometric measurements were not obtained.
The selected students answered self-administered questionnaires using an electronic data collector (Personal Digital Assistant [PDA] model LG GM750Q, LG Electronics, CA, USA) at schools under supervision. Questions included data on age, race, tobacco use, and oral contraceptive use. The race was self-reported as white, mixed-race, black, Asian, and native Brazilian, according to the classification of the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística [IBGE]).18 Adolescents who had smoked on at least one day in the past 30 days were considered smokers. The type of school administration (public or private) and location (urban or rural) was obtained by school information.
Weight was measured using an electronic scale (Líder® P150m, with a capacity of 200 kilograms and precision of 50 grams, São Paulo, Brazil). The adolescents were barefoot and wearing light clothing. Height was measured using a portable stadiometer (Alturexata®, with an extension of up to 213 centimeters, with a 1 millimeter precision, Minas Gerais, Brazil). Two measurements were taken according to the protocol proposed by Lohman et al.19 The average of the two measurements was used to calculate body mass index (BMI) in kilogram per meter square (Kg/m2). Participants were classified into three categories: underweight (wasted and severely wasted), normal weight, excess weight (overweight and obese) by z-score as the criteria proposed by World Health Organization.20
For analysis purposes, some sociodemographic variables were recategorized in binary data. Adolescents were divided into two groups according to age (12 – 14 years and 15 – 17 years). Nutritional status was reclassified into two categories: "without excess weight" (normal weight and underweight) and “excess weight” (overweight and obese). Finally, regarding race, girls were considered as Non-White and White.
To define MetS was used the criteria from the IDF.21 Therefore, waist circumference (WC), blood pressure and biochemical parameters were included. To classify with MetS, the obligatory variable was enlarged WC. Besides that, were necessary two or more alter components.
WC was measured in centimeters using an inelastic measuring tape (Sanny®, with an extension of up to 150 centimeters, with a 1 millimeter variation, São Paulo, Brazil), at the midpoint between the bottom of the last rib and the upper curvature of the iliac crest, with the adolescent in a standing position, arms along the body and with her feet and abdomen relaxed. WC was enlarged when was greater than or equal to 90o percentile for girls under 16 years old and greater than 80 centimeters for those who were 16 or over.
Blood pressure measurements were performed using a device validated for use in adolescents (OMRON 705 CP®, G-Tech International, Republican of Korea). The measurements were performed twice and with an interval of two minutes between them and the average value of the measures was considered to classify. The cutoff points used were greater than or equal to 130 mmHg and to 85 mmHg to consider systolic and diastolic blood pressure high, respectively.
A sample of venous blood was collected after an overnight fast (12 hours) for laboratory analysis. The following tests were analyzed using the colorimetric enzymatic method, kit LABTEST®: high-density lipoprotein cholesterol (HDL-c), triglycerides (TG) and fasting glucose. For classification, were used the cutoff points HDL-c:< 40 mg/dL up16 years old and < 50 mg/dL to 16 and 17 years old; TG: ≥ 150 mg/dL and fasting glucose: ≥ 100 mg/dL.
Descriptive statistics were reported as prevalence and their respective confidence interval of 95% (95%CI) of contraceptive pill use according to age, nutritional status, school´s characteristics, race, Brazilian macro-regions, tobacco use, presence of MetS, and their altered components. Bivariate analyses were performed using logistic regression to verify the association between sociodemographic variables and contraceptive use. References were age group 12 – 14 years; adolescents without excess weight [very low weight, low weight, and normal weight]); public school administration; rural school region; race non-white and non-smokers. The multivariate analysis was performed only with variables that showed p < 0.05 in the bivariate analysis. Subsequently, logistic regression was used to study the association between the presence of MetS and their components and contraceptive pill use. Crude and adjusted for age, school region, race, and tobacco use odds ratios (ORs) and their respective 95% CI were calculated. Analysis was performed using Stata software (Stata 14.0 Statistical Software. College Station, TX, USA), employing statistical routines for complex samples.
All participating students signed an assent form. The study was approved by the Research Ethics Committee of the institution of the Study Coordination Center (IESC/UFRJ – Process 45/2008) and by each Brazilian state involved.
ResultsOf the 102,327 eligible participants registered in the selected schools, a subsample consisting of students from the morning shift who collected blood samples answered the questionnaire, and then underwent anthropometric and blood pressure measurements, which were assessed. This subsample was composed of 37,815 students, 22,682 of whom were female and of these 12.65% reported using OCs (Fig. 1).

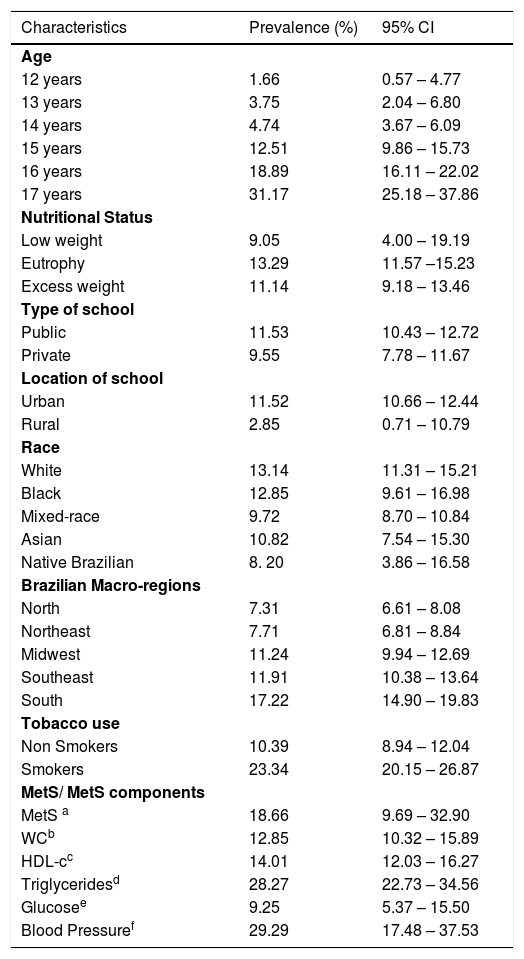
Regarding the prevalence of use of OC according to social demographics characteristics, it was significantly higher in older adolescents with progressive increase with age and among smokers without overlapping of the 95% confidence interval. Considering the location of the school, the prevalence was highest among those studied in urban areas and the South region when compared with North and Northeast regions. The prevalence did not differ by nutritional status, type of school administration and race considering all five possibilities of IBGE's classification. The analysis of the association between the use of OC and the presence of components of MetS showed a high prevalence, almost 30%, among adolescents with altered blood pressure and in those with hypertriglyceridemia, while this rate was much lower, around 10%, in adolescents with altered fasting glucose levels (Table 1).
Prevalence (%) and 95%CI of contraceptive pill use according to age, nutritional status, school's characteristics, race, smoking habit, Brazilian macro-regions, MetS and MetS components. ERICA, Brazil, 2013-2014.
| Characteristics | Prevalence (%) | 95% CI |
|---|---|---|
| Age | ||
| 12 years | 1.66 | 0.57 – 4.77 |
| 13 years | 3.75 | 2.04 – 6.80 |
| 14 years | 4.74 | 3.67 – 6.09 |
| 15 years | 12.51 | 9.86 – 15.73 |
| 16 years | 18.89 | 16.11 – 22.02 |
| 17 years | 31.17 | 25.18 – 37.86 |
| Nutritional Status | ||
| Low weight | 9.05 | 4.00 – 19.19 |
| Eutrophy | 13.29 | 11.57 –15.23 |
| Excess weight | 11.14 | 9.18 – 13.46 |
| Type of school | ||
| Public | 11.53 | 10.43 – 12.72 |
| Private | 9.55 | 7.78 – 11.67 |
| Location of school | ||
| Urban | 11.52 | 10.66 – 12.44 |
| Rural | 2.85 | 0.71 – 10.79 |
| Race | ||
| White | 13.14 | 11.31 – 15.21 |
| Black | 12.85 | 9.61 – 16.98 |
| Mixed-race | 9.72 | 8.70 – 10.84 |
| Asian | 10.82 | 7.54 – 15.30 |
| Native Brazilian | 8. 20 | 3.86 – 16.58 |
| Brazilian Macro-regions | ||
| North | 7.31 | 6.61 – 8.08 |
| Northeast | 7.71 | 6.81 – 8.84 |
| Midwest | 11.24 | 9.94 – 12.69 |
| Southeast | 11.91 | 10.38 – 13.64 |
| South | 17.22 | 14.90 – 19.83 |
| Tobacco use | ||
| Non Smokers | 10.39 | 8.94 – 12.04 |
| Smokers | 23.34 | 20.15 – 26.87 |
| MetS/ MetS components | ||
| MetS a | 18.66 | 9.69 – 32.90 |
| WCb | 12.85 | 10.32 – 15.89 |
| HDL-cc | 14.01 | 12.03 – 16.27 |
| Triglyceridesd | 28.27 | 22.73 – 34.56 |
| Glucosee | 9.25 | 5.37 – 15.50 |
| Blood Pressuref | 29.29 | 17.48 – 37.53 |
95%CI, 95% confidence intervals; MetS, metabolic syndrome; WC, waist circumference; HDL-c, High Density Lipoprotein-cholesterol.
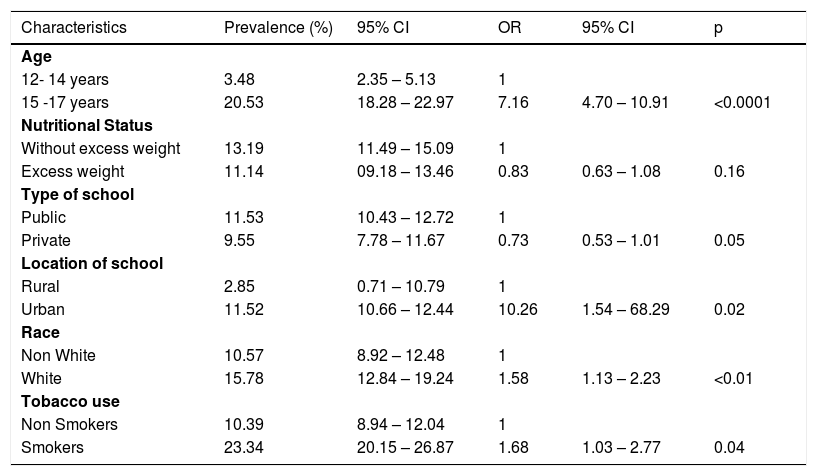
Considering sociodemographic data after recategorization, bivariate analyses were performed by simple logistic regression to obtain the unadjusted OR values. The variables age group, school region, race and tobacco use were significantly associated with the outcome and were used for the adjusted OR (Table 2).
Prevalence (%) and 95%CI and Odds Ratio (OR) of contraceptive pill use according to variables recategorized in binary format. ERICA, Brazil, 2013-2014.
95%CI, 95% confidence intervals; OR, Odds Ratio.
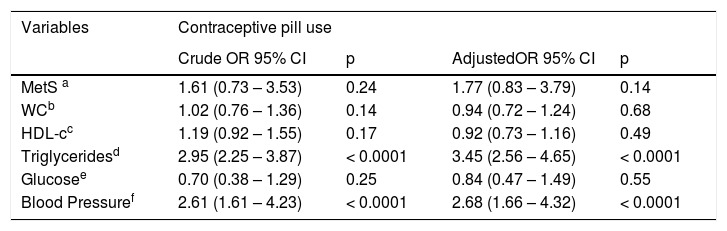
Use of OCs was significantly associated with altered blood pressure and hypertriglyceridemia, with a 2.61- and 2.95 fold increase, respectively. The associations with these two cardiovascular risk factors remained significant, even after adjusting for the sociodemographic variables (Table 2) age, school region, race and tobacco use with an increase of 2.68 and 3.45 times, respectively (Table 3).
Crude and adjusted odds ratio analysis between MetS and MetS components and contraceptive pill use. ERICA, Brazil, 2013-2014.
| Variables | Contraceptive pill use | |||
|---|---|---|---|---|
| Crude OR 95% CI | p | AdjustedOR 95% CI | p | |
| MetS a | 1.61 (0.73 – 3.53) | 0.24 | 1.77 (0.83 – 3.79) | 0.14 |
| WCb | 1.02 (0.76 – 1.36) | 0.14 | 0.94 (0.72 – 1.24) | 0.68 |
| HDL-cc | 1.19 (0.92 – 1.55) | 0.17 | 0.92 (0.73 – 1.16) | 0.49 |
| Triglyceridesd | 2.95 (2.25 – 3.87) | < 0.0001 | 3.45 (2.56 – 4.65) | < 0.0001 |
| Glucosee | 0.70 (0.38 – 1.29) | 0.25 | 0.84 (0.47 – 1.49) | 0.55 |
| Blood Pressuref | 2.61 (1.61 – 4.23) | < 0.0001 | 2.68 (1.66 – 4.32) | < 0.0001 |
CrudeOR, crude odds ratio; AdjustedOR, odds ratio adjusted by age, location of school, race and tobacco use; 95%CI, 95% confidence intervals; MetS, metabolic syndrome; WC, waist circumference; HDL-c, HDL-cholesterol.
The present study was the first to examine the association between the use of OCs and Mets and their altered components among the largest number of female Brazilian adolescents between 12 and 17 years ever assessed in a single study in Brazil, with national and regional representatives who attend schools and live in municipalities with over 100,000 inhabitants.
Almost thirteen percent of female participants in the current study were on OC use. This proportion was similar to the 14% obtained in a Belgian survey with 1,526 adolescents aged 12–17 years8 and it was lower when compared with more recent studies and with older and/or sexually active participants in developed countries. A German survey evaluated 2,699 female adolescents aged between 14 and 19 years with a 86% of OC use prevalence.22 A United States nationally representative sample of public and private schools estimated 23.3% of OC's use prevalence among 3,226 sexually active high school students.23
In the present study, OC use was significantly higher among older, urban, white and adolescents. These results are in agreement with previous school-based surveys.23. Therefore, improving younger, non-white and rural adolescents’ knowledge of, comfort with, and access to the most effective methods of pregnancy prevention is needed.
As previously reported,11 there were significant differences in the prevalence of OC use in the Northern and Northeastern regions in relation to other macro-regions, especially the South region. This can be explained by the heterogeneity in access to health services and contraceptive supplies in a multicultural continental-size country like Brazil.
An important finding was the association between smoking habits and OC's use. In this sample, approximately 23% of the current smokers were OC users compared with 10% among non-smokers. This observation was also noted in other teenagers populations.7,8 During adolescence, physical, cognitive, emotional, and behavioral changes occur and frequently experimentation may include tobacco use and sexual activity, which may be associated with sexual and reproductive health risks such as unintended pregnancy.
In a crude and adjusted model for age, location of the school, color and smoking, use of OC is not associated with excess weight, as observed in a Cochrane review24 with adult women and in a cohort study with adolescents.25 During adolescence, the main reason for avoiding the use of OC is to worry about excessive weight gain.14 Thus, these results from this and the other studies24,25 could be used to encourage the use of this method to prevent unwanted pregnancies in this age group.
Considering the effect of OC, especially estrogenic component, on metabolic and cardiovascular changes,26 the main objective of the present study was to investigate the association between OC use and MetS and their components in Brazilian adolescents. This study found increased odds to MetS without significance statistic and statistically significant association with hypertension and hypertriglyceridemia among OCs users, even after adjusted analysis for age, location of school, race and tobacco use. The result was in agreement with earlier findings in adult women and adolescents,5,7,9,27–29 although an observational, matched cohort study didn't show significant associations between OC use and blood pressure changes in adolescents.25
Among the limitations of the present study was the cross-sectional design, which does not allow the establishment of a causal relation in the observed associations. Second, considering progestin-only contraception seems safe with respect to the risk of cardiometabolic outcomes,2 another limitation was the lack of information about the type of OC's components. Third, cardiovascular risk factors generally accumulate over time and there is not a question about the prior duration of use before the survey. However, the sample size and representativeness and similar previous results increase the importance of these findings.
In summary, this sample shows that OC's use in healthy adolescents was not associated with excess weight and MetS, although was significantly associated with hypertension, hypertriglyceridemia and tobacco use. Improving adolescent access to contraceptive methods is essential to prevent unintended pregnancy and sexually transmitted diseases. Considering this, all physicians should be aware that after starting on OC, patients should be seen for a follow-up to check up on medication adherence and side effects, including monitoring of blood pressure. In addition, preventive actions should target to avoid the combined use of OC and modifiable behavior-related cardiovascular risk factors, as smoking habit, in teenagers in order to prevent later consequences on cardiovascular disease incidence.
FundingBrazilian Ministry of Health (Ministério da Saúde do Brasil).
Study conducted at Universidade do Estado do Rio de Janeiro, Núcleo de Estudos da Saúde do Adolescente, Faculdade de Ciência Médicas, Programa de Pós-Graduação em Ciências Médicas, Rio de Janeiro, RJ, Brazil.





