



To review and discuss the role of an elimination diet in food-allergic children, emphasizing nutritional aspects for a better practical approach.
SourcesNon-systematic review of the literature.
FindingsUnder an elimination diet, food-allergic patients may suffer from growth impairment or obesity and compromised quality of life. Disease phenotype, age, type, number of foods excluded, comorbidities, eating difficulties, economic status, and food availability must be considered for an appropriate diet prescription. Diet quality encompasses diversity and degree of food processing, which may alter immune regulation.
ConclusionsA friendly food elimination diet prescription depends on a multidisciplinary approach beyond macro and micronutrients.
After diagnosing a food allergy (FA), dietary avoidance of the involved allergen is the central pillar in managing these patients to prevent allergic symptoms. However, more active treatments such as allergen-specific immunotherapy and biologicals are emerging possibilities. A temporary elimination diet, followed by reintroduction, either for the child or the breastfeeding mother, can still be helpful as a diagnostic tool, especially for non-IgE mediated manifestations of mild severity, for which other diagnostic auxiliary tools are still lacking.
Food restriction may impose nutritional1 and emotional burdens, not being an easy task, both for the growing and developing child, as well as for the breastfeeding mother and other family members. On the other hand, dietary diversity and quality, especially in the first year of life, is vital to prevent allergies.2
This review aims to discuss the role of an elimination diet in allergic children in its diagnostic and "therapeutic" contexts, emphasizing nutritional aspects.
Elimination diet for diagnostic purposesIn non-IgE-mediated allergies, especially in food protein-induced allergic proctocolitis (FPIAP), the elimination diet is recommended, usually for one to two months, followed by reintroduction.3 An elimination diet for at least two weeks is recommended for IgE-mediated manifestations before the oral food challenge under medical supervision.2
Some food allergies outgrow naturally, so regular reassessment of the allergic status should be considered to avoid unnecessary prolonged food restriction.
More recently, low-dose oral food challenges have been proposed to establish the minimum eliciting dose of a specific protein source. This approach aims to reduce anxiety and possibly unnecessary restriction due to precautionary labeling (“may contain”).4
Elimination diet in the care of food-allergic patientsTo prevent allergic reactions, once the diagnosis of FA is confirmed, food elimination is indicated with appropriate replacement.
It is important to emphasize that, in the case of breastfeeding, this should be stimulated for its numerous benefits, and the food restriction of the maternal diet with adequate substitution is indicated in cases in which the allergic manifestation occurs through breast milk, such as, for example, FPIAP. In the context of IgE-mediated allergic reactions, it is exceedingly rare for symptoms to happen via breast milk, as evidenced by a recent systematic review.5 When there is no reaction via breast milk, it is desirable and recommended not to eliminate the food from the maternal diet, not only because maternal dietary restriction impairs the quality of the produced milk6 but also because breastfeeding may be a route of presentation of the allergen to the child that favors the induction of tolerance,7 especially in those with atopic dermatitis and increased risk of skin sensitization.8
When breastfeeding is not possible in the context of Cow's Milk Allergy (CMA) under two years of age, substitute formulas are indicated:
- -
Soy-based formulas: for children over six months of age for IgE-mediated reactions.
- -
Extensively hydrolyzed formula: infants at any age for all phenotypes.
- -
Amino acid formula: infants with anaphylaxis due to Cow's Milk (CM) and when extensively hydrolyzed formulas are not tolerated.
Noteworthy, milk from other mammals is commonly allergenic to those children because of the high similarity among proteins, and when intestinal symptoms are not present, extensively hydrolyzed formulas containing lactose are a possibility.2
Most CM and egg allergies tolerate processed food associated with a wheat matrix and baked in high temperatures for a prolonged time (180°C for 25 to 30 minutes), which reduces the allergenicity of proteins by denaturing the conformational epitopes present in foods.9 Once the tolerance to baked goods is confirmed through clinical history and/or oral food challenge, the allergens are allowed to be consumed in this way, respecting the conditions of preparation that guarantee their reduced allergenicity. It is noteworthy that not all processing decreases the allergenicity of food and that even some food sources, when processed, induce greater clinical reactivity.10
More recently, allergen-specific oral immunotherapy is sometimes a more active approach to immediate FA. It consists of administering increasing doses of allergen under medical supervision and in a controlled environment, followed by home maintenance to induce tolerance. However, to date, most achieve the status of "sustained non-responsiveness" (tolerance only when submitted to a regimen of controlled and regular dose intake) and not true tolerance (ingestion as much as wanted and when desired).11
Regarding eosinophilic esophagitis (EoE) a meta-analysis including thirty-four studies with 1762 patients showed that the overall rate of histologic remission due to diet management was 53.8% (95% CI, 48.0%–59.6%), and in the individual dietary groups was 61.3% (95% CI, 53.0%–69.3%) for six-food elimination diet, 49.4% (95% CI, 32.5%–66.3%) for four-food elimination diet, 51.4% (95% CI, 42.6%–60.1%) for one-food elimination diet, and 45.7% (95% CI, 32.0%–59.7%) for a targeted elimination diet. Dietary regimen and patient age did not significantly affect rates of histologic remission. The authors concluded that dietary therapy is an effective treatment for EoE patients of any age. The current results could support a trend toward less restrictive dietary regimens as a primary treatment option.12
Diet quality and immune systemAs the main form of treatment for FA is the exclusion of the food involved in allergic reactions, nutrition's role in managing FA has always been central, both to avoid adverse reactions and to prevent nutritional risks.
Until recently, the focus in nutritional therapy for FA was finding a substitute/replenishing nutrients for the excluded food(s) to prevent/treat nutritional deficits. However, with the increase in the persistence and prevalence of FA and the emergence of new evidence regarding the interface between nutrition and the functioning of the immune system, there is growing concern about the quality of the diet of children and adolescents with FA.13
Diet quality encompasses many aspects; among them, one can mention dietary diversity, which emerges as a promising role in the immune system and healthy intestinal microbiota14 and the degree of industrial food processing (ultra-processed foods – UPF, substances resulting from processing, such as advanced glycation end products – AGEs and food additives).15,16
Food diversity and food allergiesAs the name suggests, dietary diversity refers to the number of foods/groups consumed in a period but also includes the nutritional value and frequency with which these foods are consumed.14 Food diversity in children's diets has been associated with allergy prevention, as it is related to reduced childhood allergy outcomes.17
It would not be possible to discuss dietary diversity and not mention complementary feeding in infants with CMA. Some foods that are part of the dietary introduction, such as eggs and fish, are considered most allergenic. Furthermore, essential foods such as fruits and vegetables, not the most common food allergens, have been increasingly linked to allergic reactions.18 Given this, many parents and health professionals delay food introduction to infants with FA or do so very slowly. However, the variety of foods offered in the first year of a child's life appears to be associated with a reduced risk of developing FA in the first ten years.19
It is worth mentioning that the introduction of food to infants with FA must be done as recommended for all infants from 6 months of age (respecting the child's signs of readiness), prioritizing unprocessed and minimally processed foods, including all groups of foods (fruits, vegetables, cereals, roots and tubers, beans, nuts, and animal proteins) and offering them frequently in the infant's diet.20 The only caveat is that for children who have presented symptoms of FA in the first months of life, before introducing foods other than breast milk, it is best to avoid the simultaneous introduction of two or more foods that are protein sources.3
Introducing foods considered more allergenic and a varied diet should be encouraged so infants with FA do not lose the already recognized benefits of a diversified diet.
Consumption of ultra-processed foods in food allergiesUPF consumption has tripled in the last 30 years among adults, and there is much evidence in the literature, including meta-analyses, that its consumption is associated with one or more negative health outcomes.21
In children and adolescents, the most relevant findings demonstrated an association between UPF consumption and overweight and obesity, cardiometabolic comorbidities, worsening of lipid profile, and metabolic syndrome.22-25 Results of a study conducted with 110 Brazilian children and adolescents with FA that evaluated the consumption of UPF26 showed a high consumption among these individuals (average 33% contribution of UPF to the total energy consumed) when compared to individuals healthy between 10 and 18 years old (average 26% UPF contribution to the total energy consumed).27 It was emphasized that there is no safe amount of UPF intake.
UPF are industrial formulations with little fiber, water, micronutrients, and a large amount of added sugar, sodium, saturated fat, and food additives.20 Additionally, the composition and way UPF are produced induces the Maillard reaction (MR - a non-enzymatic reaction between carbohydrates and proteins, also known as glycation), one of the primary mechanisms for forming advanced glycation ends exogenous products (AGEs).15
MR promotes chemical and conformational changes in food proteins, influencing digestibility, bioavailability, immunogenicity, and allergenicity.15 This MR effect may appear to be linked to the structural characteristic of the protein, ionic strength, heating time and temperature, carbohydrate type, pH, and water activity.28
In recent years, it has been postulated that the accumulation of AGEs in the body could influence the persistence and increase of FA (Figure 1).
 inflammation, through the interaction of AGEs with their receptors (RAGEs), which can lead to increased production of pro-inflammatory cytokines; (B) induction of new IgE-binding epitopes; (C) Reduction in the diversity of the intestinal microbiota, which can lead to increase susceptibility to allergies, as well as a delay in acquiring tolerance. AGEs - advanced glycation end products; RAGEs – receptor advanced glycation end products.")
The accumulation of AGEs in the body has been related to the increased prevalence and worsening of FA. Among the proposed mechanisms: (A) inflammation, through the interaction of AGEs with their receptors (RAGEs), which can lead to increased production of pro-inflammatory cytokines; (B) induction of new IgE-binding epitopes; (C) Reduction in the diversity of the intestinal microbiota, which can lead to increase susceptibility to allergies, as well as a delay in acquiring tolerance. AGEs - advanced glycation end products; RAGEs – receptor advanced glycation end products.
Below, the authors list some proposed mechanisms of the interaction of AGEs with FA:
- 1)
Inflammation (receptors present on antigen-presenting cells): Food allergens in the presence of AGEs can trigger the RAGE receptor and cooperate to produce pro-inflammatory cytokines through antigen-presenting dendritic cells and T cell responses. And that has been associated with the development and progression of several diseases. Among them, FA causes allergic sensitization through dendritic cells, antigen-presenting cells, and T-cell responses. Furthermore, the interaction of AGEs with RAGEs appears to activate mast cells, with a possible participation in the pathogenesis of FA.28-30
- 2)
Induction of new IgE binding epitopes (change in protein structure): The alteration of the function of glycated proteins occurs because MR leads to the aggregation of proteins through intermolecular or intramolecular cross-linking between lysine and arginine residues in the creation of shared AGEs. This process can alter the level of IgE and antigen-presenting cell recognition. In other words, proteins modified by AGEs can lead to immunogenic responses.31
- 3)
Reduction in the diversity of the intestinal microbiota: There is evidence that the intestinal microbiota can influence anti- and pro-inflammatory responses in the intestine.2 It has been proposed that the breakdown of the integrity of the intestinal epithelial barrier may allow entry of food allergens, toxins, and other substances that can lead to inflammation.32,33
AGEs have been associated with reduced intestinal microbiota, leading to greater susceptibility to allergies and/or a delay in the acquisition of tolerance in individuals with FA.15 Reduction of butyrate-producing bacteria has been associated with an allergic phenotype,34 as this stimulates the development of regulatory T cells (Treg).35
On the other hand, the participation of some fatty acids in improving the function of the intestinal epithelial barrier has been proposed. It is possible that Lactobacillus derived from 10-hydroxy-cis-12 octadecenoic acid (a metabolite derived from linoleic acid), as well as short-chain fatty acids (acetate and butyrate), favor the maintenance of the intestinal epithelial barrier and, therefore, is a protective factor for FA prevention.36
Furthermore, the hypothesis has recently emerged that phosphorus, a mineral widely found in foods considered more allergenic, such as eggs, fish, milk, oilseeds, peanuts, soybeans, and wheat, when consumed in large quantities and associated with a diet rich in AGEs could harm the immune system.37
Although many mechanisms have been proposed and the adverse health effects of exogenous AGEs are known, it is still unknown whether chronic consumption of AGEs alone is to blame for their negative impact on human health.38,39 Studies need to be carried out to elucidate this binomial. Furthermore, it is pertinent to mention that exogenous AGEs are more related to how the food is cooked. This covers all foods that suffer from MR, including homemade food.40
Another component of interest in the literature on UPF is food additives, which are substances intentionally added to UPF without nourishing but altering these foods' chemical, biological, physical, or sensory characteristics.41 The variety of food additives is vast, as is their applicability. Foods such as processed bread, margarine, and even baby foods such as infant formula may contain food additives such as polysorbate (P20 and P80), carboxymethylcellulose (CMC) and carrageenan (E407). Such additives have been associated with compromised intestinal mucosa and changes in the intestinal microbiota, with consequent inflammation, increased oxidative stress, and changes in the immune system.42-44
Nutrition for healthDiets rich in UPF may increase the risk of developing and worsening FA. On the other hand, evidence is growing regarding the immunomodulatory functions of the nutrients (Figure 2). A diet rich in unprocessed and minimally processed foods should be the basis of a healthy diet, as they are rich in fiber, macro and micronutrients, and antioxidant substances.

Immunomodulatory functions of nutrients. Adapted from Vlieg-Boerstra.2 Adapted from Allergy, volume 78, issue 6, Vlieg-Boerstra, B., Groetch, M., Vassilopoulou, E., Meyer, R., Laitinen, K., Swain, A., Durban, R., Benjamin, O., Bottse, R., Grimshaw, K., Netting, M., O'Mahony, L., de Jong, N., & Skypala, I. J., “The immune-supportive diet in allergy management: A narrative review and proposal”, pages 1441–1458, doi: 10.1111/all.15687, with permission from John Wiley and Sons.
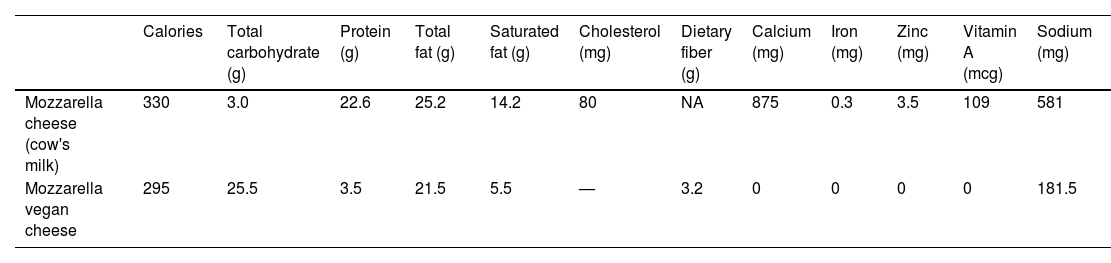
A crucial topic in FA nutritional therapy is appropriate substitution based on the principles proposed by the Dietary Guides.9 There are several publications suggesting substitute foods for the main food allergens. However, it is essential to differentiate between types of substitute foods, as they are not all the same. For better reasoning in nutritional management, the authors suggest classifying them into (i) nutritional substitute (equivalent foods or with some nutrients present in the food allergen source) and (ii) cooking substitute (an ingredient used for cooking that has technological functions like the allergenic source), for example, vegan cheeses. When comparing them with CM-based cheeses, the authors see that the primary nutrients of interest in CM-based cheese, protein and calcium, are not equivalent between these two versions (Table 1), making the vegan cheese unviable for nutritional purposes, although possible as a cooking substitute.
Comparison between cow's milk cheese and vegan cheese (quantity in 100g of food).
Understanding that the formation of AGEs goes beyond the issue of UPF consumption and given the possible harmful effects of AGEs on human health, Uribarri et al.40 published a practical guide to reducing dietary AGEs. The set of measures proposed by the authors ranges from the degree of food processing, including herbs and acids such as lemon and vinegar in meat preparation, to cooking methods (Figure 3). The authors emphasize that there is no safe and ideal intake recommendation to prevent diseases.

Measures proposed by Uribarri et al.40. Reprinted from Journal of the Academy of Nutrition and Dietetics, volume 110, issue 6, Uribarri, J., Woodruff, S., Goodman, S., Cai, W., Chen, X., Pyzik, R., Yong, A., Striker, G. E., & Vlassara, H, “Advanced glycation end products in foods and a practical guide to their reduction in the diet”, pages 911-16.e12, 2010, doi: 10.1016/j.jada.2010.03.018, with permission from Elsevier.
The strict elimination of the responsible food from the diet means removing all forms of it, such as preparations. It can compromise an adequate and balanced diet and lead to nutritional risks.
Studies point to impaired growth in children with FA, especially short stature (height-for-age z-score < -2), affecting around 10% of children.45 Multiple factors contribute to impaired growth and include the elimination diet itself, which impacts the intake of macro and micronutrients; coexistence with eating difficulties; the presence of comorbidities such as atopic dermatitis and asthma; persistent gastrointestinal inflammation affecting nutrient absorption46 and the use of medications such as corticosteroids, which can also affect height growth, and proton pump inhibitors (PPIs).9 PPIs, commonly used in EoE, can also affect micronutrient status. A reduction in gastric acid production potentially impacts the absorption of calcium, phosphorus, iron, and vitamin B12.47 The elimination diet can also cause anxiety and stress (concern about eating, increased responsibility, caution, and fear of accidental exposure), particularly in parents and caregivers, and thus affect the child's and their family's social activities. Family with restrictions on socialization (going to restaurants and traveling), problems adapting to school.
Eating difficulties also contribute to the nutritional risk of children with FA and range from hypersensitivity and/or aversion to different textures and flavors in younger children to ARED (avoidant restrictive eating disorder) in older children, significantly reducing food consumption. The elimination diet reduces the number of food exposures and dietary variety, a traumatic event (i.e., food protein-induced enterocolitis syndrome event or anaphylaxis), and FA symptoms that can lead to abdominal discomfort and pain are all possible contributing factors.48,49
On the other hand, other studies indicate that obesity can also occur in children with FA due to inappropriate substitutions, unbalanced diets, and poor food choices.50
A good diet is based on a varied, balanced, and individualized diet, avoiding consuming ultra-processed industrialized foods, which may be the best model for treating food allergies. The biggest challenge for anyone working in this area is to ensure that the quality and quantity of nutrients are guaranteed, even with one or more exclusions.2 Comprehensive dietary advice should consider individual nutritional needs and appropriate and locally available food alternatives and assess the family's cooking skills and economic status. Furthermore, caregivers should receive guidance on promoting dietary diversity, particularly during complementary feeding, and know the long-term impact of diet on health and disease prevention.
Concerning micronutrients, Meyer et al., analyzing the dietary surveys of 110 children with non-IgE-mediated FA, showed that the children were at risk of inadequate vitamin D, zinc, calcium, and selenium.51 Low concentrations of serum biomarkers such as zinc, iron, selenium, vitamin A, vitamin D, and calcium have also been described in children with FA.9,52 Thomassen et al. studied urinary iodine concentrations in children with CMA and found that a third had levels compatible with iodine deficiency.53
It has been widely established that children with FA who receive nutritional guidance and monitoring from a specialized nutrition professional are at significantly lower risk of developing deficiencies, particularly micronutrient deficiencies.45 Although there are no specific guidelines for routine measurement of serum biomarkers for micronutrients in children with FA, a detailed dietary history can guide the need for measurement and eventual supplementation. The European Society for Pediatric Gastroenterology, Hepatology, and Nutrition has developed a guideline on the accuracy of nutrition-related biomarkers for sick children that may also be useful for those with FA.54
Below, the authors list some aspects that should be considered when assessing the nutritional risk of children with FA:
- 1)
Low age (generally children under two years): due to the intense period of growth and development that must be monitored longitudinally with appropriate curves. Food consumption should be assessed at every consultation to guide nutritional management.
- 2)
Disease phenotype (EoE) or associated allergic diseases (atopic dermatitis or asthma): Children with EoE present symptoms that can limit adequate nutritional intake, such as recurrent vomiting and regurgitation, abdominal pain, lack of appetite, low volume, and/or small variety of foods. Patients with chronic inflammation of the esophagus develop compensatory eating habits (i.e., drinking plenty of fluids during meals, eating slowly, chewing carefully, cutting food into small pieces, lubricating food with sauces or liquids) or avoiding certain foods (meat, crispy bread and hard or fibrous foods such as meat). Furthermore, young children fed liquid formula for a long time do not engage their masticatory muscles and are prone to delayed onset of oral motor skills. Another important aspect is the delay in diagnosis, which can culminate in the presence of esophageal rings and strictures, which further prolongs gastrointestinal symptoms and eating discomfort with the possibility of impaction. Patients with episodes of food impaction may be at high risk of developing anxiety and eating disorders, compromising adequate nutrient intake. Therefore, chronic gastrointestinal symptoms, compensatory eating habits, and eating disorders can complicate the nutritional status of EoE patients, especially if they are children. Finally, poor adherence to therapy is the main reason for therapeutic failure and persistent active inflammation.55
This emerging chronic disease's complexity and clinical heterogeneity imply a multidisciplinary approach, including an allergist, pediatrician, gastroenterologist, nutritionist, and psychologist, to manage these patients. Before starting diet therapy and during the follow-up period, the team must periodically assess the nutritional status of patients and rule out a potential deficiency. The risk of nutritional deficiency and impaired growth increases with the restrictive nature of the diet and the number of foods removed.55
- 3)
Type and number of foods excluded: The exclusion of allergenic foods can lead to deficiencies in macro and micronutrients, such as vitamins, minerals, and fiber, if measures are not taken to ensure appropriate substitution. For example, people allergic to milk may be at risk for calcium deficiency, while those allergic to grains may face a reduction in fiber intake. If left untreated, malnutrition and other nutritional deficiencies progress and can result in inadequate nutrient intake, malabsorption, metabolic changes, and/or increased nutritional needs.56 Christie et al. reported that children who eliminated two or more foods were shorter in height for their age than those who eliminated just one food.57
CM and dairy products contribute to early childhood nutrition for non-breastfed children and are responsible for most allergic reactions at this stage. Children who eliminated CM from their diet had lower protein and lipid intakes than the control group, which resulted in lower energy levels.58
Plant-based drinks have increased in popularity in recent years. While soy-based beverages have been on the market for more than 30 years, consumers now have the option of beverages made from almond, coconut, hazelnut, walnut, macadamia, quinoa, oat, hemp, potato, pea, and rice. Such drinks generally have low energy and protein content; some are supplemented with calcium.59 They do not correspond to the nutritional content of any infant formula. They can only be considered a cooking substitute (food ingredient) after six months and as a drink after two years of age, subject to nutritional monitoring.9
- 4)
Consumption of processed foods: There is an ongoing effort to define limits on allergens in processed foods that would inform the need for precautionary labeling of allergens. A recent position suggested a universal limit of 0.5 mg of protein per 100g of processed food as a universal guideline for food labeling.60 Careful reading and interpretation of labels should be part of the nutritional guidance offered to patients with FA and their families. In current Brazilian legislation, the term “may contain” sometimes confuses families with increased unnecessary consumption restrictions.
How to reduce nutritional risk:
- 1.
Preventing malnutrition and nutritional deficiencies is fundamental in treating FA, as they can lead to sequelae in somatic and cognitive growth and development. Therefore, the importance of a nutritionist in the team who assists children with FA is highlighted.
- 2.
Monitoring anthropometric measurements at each consultation with longitudinal monitoring on appropriate curves.
- 3.
Assess food consumption and, when necessary, request nutritional biomarkers.
- 4.
Encourage, whenever possible, breastfeeding with appropriate guidance on the exclusion diet for the mother.
- 5.
Children under two years of age with CMA who are not breastfed should receive soy-based (over six months and without GI manifestations), extensively hydrolyzed (under six months), or amino acid-based infant formulas (anaphylaxis and non-IgE-mediated forms with poor response to extensively hydrolyzed) as substitutes.
- 6.
Nutritional guidance, including dietary diversity and expanding texture and flavor from the beginning, to avoid eating difficulties.
The elimination diet is fundamental to avoid reactions to food allergies, but it imposes enemies as nutritional risks and emotional burdens, so a multidisciplinary effort is necessary. First, the correct diagnosis of the allergic status is essential. The quality of a friendly elimination diet must consider not only macro and micronutrients but also diversity, food processing, possible eating difficulties, and other comorbidities. Consuming unprocessed and minimally processed foods should be prioritized over UPF as it prevents the development of other chronic diseases and modulates the immune system. When appropriate, allergic status must be reassessed to avoid further unnecessary restrictions.
None.





