

To analyze the impacts of climate change on the development of immature respiratory and immune systems in children.
Source of dataThe authors of the present study performed a non-systematic review of English, Spanish, and Portuguese articles published in the last five years in databases such as PubMed, EMBASE, and SciELO. The terms used were air pollution OR climate changes OR smoke, AND children OR health.
Synthesis of dataThe increase in the prevalence of some diseases, such as allergic ones, is attributed to the interactions between genetic potential and the environment. However, disordered growth combined with inadequate waste management has caused problems for the planet, such as heatwaves, droughts, forest fires, increased storms and floods, interference in food crops and their nutritional values, changes in the infectious disease pattern, and air pollution resulting from the continuous use of fossil fuels. Children, beings still in the development stage with immature respiratory and immune systems, are the primary victims of the climate crisis.
ConclusionsThe authors documented that prenatal and postnatal exposure to ambient air pollutants will accelerate or worsen the morbidity and mortality of many health conditions, including allergic diseases. Ambient air pollutants change the microbiota, interfere with the immune response, and take direct action on the skin and respiratory epithelium, which facilitates the penetration of allergens. Understanding how the children and adolescent health and well-being are affected by climate change is an urgent matter.
Climate change is one of the main concerns of humankind due to social, economic and health impacts on the population.1 Although air quality has improved in many regions in recent decades, levels of certain air pollutants still exceed those established by the World Health Organization (WHO) guidelines in most countries, 90% of people on Earth breathe polluted air.2
There is evidence that indicate an increase in the prevalence of some diseases, such as allergic ones, is attributed to the interactions between genetic potential and the environment. This review aimed to assess the relationship between exposure to climate change and pollution in the development and/or worsening of allergic diseases in children and adolescents.
Climate change and air pollution are closely related. The burning of fossil fuels is the main contributor to air pollution. Human activities and reliance on fossil fuels have led to increased concentrations of natural and anthropogenic greenhouse gas emissions. Climate change brings together heatwaves and drought, which facilitate forest fires, increased intensity of storms and floods, affecting crops and food quality, changes in the pattern of infectious diseases, and air pollution from the continuous use of fossil fuels. These changes can induce stress, mental problems, food-borne, water-borne, or vector-borne diseases, respiratory diseases, malnutrition, illnesses brought on by excessive heat poverty, and displacement.2,3
Children, beings still in the development stage with immature respiratory, immune, and other systems, are the primary victims of the climate crisis.3 During the warmer season, they are generally exposed to higher temperatures for longer when playing outdoors, and because they are less able to maintain the ideal indoor temperature, they are at risk of experiencing thermal stress. As such, understanding how children and adolescent health and well-being could be affected by climate change is an urgent matter.4
It is impossible to predict the impact of climate change on future generations. However, the various adverse health outcomes from prenatal and postnatal exposure will likely have a combined effect that will accelerate or worsen morbidity and mortality of many health conditions, including allergic diseases.5
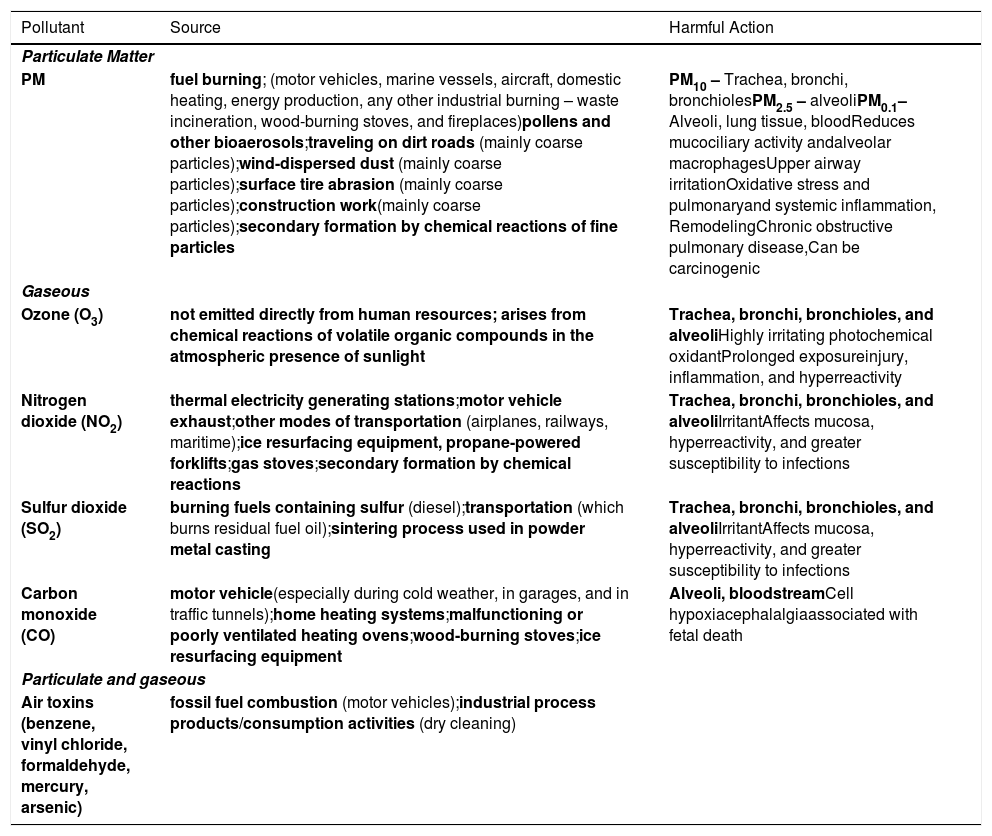
Environmental pollutantsAir pollutants can be classified as primary or secondary. Primary pollutants are emitted directly by sources such as CO, SO2, and particulate matter (PM), while secondary pollutants form in the atmosphere due to chemical and physical reactions (O3, NO2, sulfates, and ultra-fine particulates).6 They can be classified as gaseous or PM, depending on their composition. O3, nitrogen oxides (NOx), CO, CO2, volatile organic compounds (VOC), polycyclic aromatic hydrocarbons (PAH), and heavy metals are among the gaseous compounds.6
The PM (solid and liquid particles) can be subdivided by taking its aerodynamic diameter into account in: PM10 (< 10 µm), PM2.5 (< 2.5 µm), and PM0.1 (ultra-fine particulates; < 0.1 µm).5 PM's gaseous compounds negatively affect the airways, and it has a significant impact on the respiratory system (Table 1).6
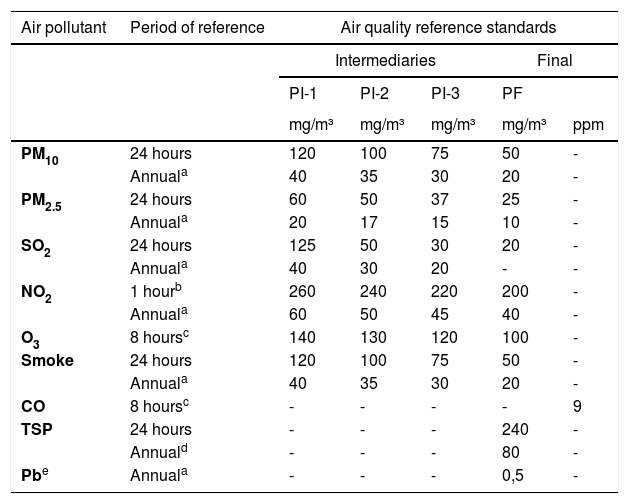
In the last decades, many countries have developed projects to reduce the emission of pollutants into the atmosphere, where many of these have not been fulfilled or are in the early stages of implementation. As the case of developing countries that still need industrialization to grow are seeing air pollution levels increase. Thus, 80% of individuals living in urban areas are exposed to air pollution levels that exceed WHO guidelines.7Table 2 shows the air quality standards in Brazil, according to the countrys National Council for the Environment (CONAMA) – 2018.8
Air quality standards in Brazil according to the National Environmental Council (CONAMA) – 2018.8
| Air pollutant | Period of reference | Air quality reference standards | ||||
|---|---|---|---|---|---|---|
| Intermediaries | Final | |||||
| PI-1 | PI-2 | PI-3 | PF | |||
| mg/m³ | mg/m³ | mg/m³ | mg/m³ | ppm | ||
| PM10 | 24 hours | 120 | 100 | 75 | 50 | - |
| Annuala | 40 | 35 | 30 | 20 | - | |
| PM2.5 | 24 hours | 60 | 50 | 37 | 25 | - |
| Annuala | 20 | 17 | 15 | 10 | - | |
| SO2 | 24 hours | 125 | 50 | 30 | 20 | - |
| Annuala | 40 | 30 | 20 | - | - | |
| NO2 | 1 hourb | 260 | 240 | 220 | 200 | - |
| Annuala | 60 | 50 | 45 | 40 | - | |
| O3 | 8 hoursc | 140 | 130 | 120 | 100 | - |
| Smoke | 24 hours | 120 | 100 | 75 | 50 | - |
| Annuala | 40 | 35 | 30 | 20 | - | |
| CO | 8 hoursc | - | - | - | - | 9 |
| TSP | 24 hours | - | - | - | 240 | - |
| Annuald | - | - | - | 80 | - | |
| Pbe | Annuala | - | - | - | 0,5 | - |
Ppm, part per million; PM10, particulate matter with a diameter less than 10 µm; PM2.5, particulate material with a diameter less than 2.5 µm; SO2, sulfur dioxide; NO2, nitrogen dioxide; O3, ozone; CO, carbon monoxide; TSP, total suspended particles; Pb, lead.
The leading pollutants inside the home are released by burning solid fuels (SF) and tobacco smoke. It is thought that between 2.5 to 3 billion people in the world (about 50% of the world's population) and up to 90% of families living in rural areas use SF to cook, heat, and light their homes.9
Burning SF (biomass and coal) for heating and cooking is considered the dominant source of indoor air pollution in rural areas, a common practice given the lack of modern energy sources. The inefficient and incomplete burning of SF by using traditional methods (stoves and open fireplaces in environments without adequate ventilation) leads to higher levels of several pollutants: PAH, heavy metals, VOC, black carbon, PM, SO2, CO, and NO.10 Incomplete SF combustion is one of the primary sources of intra-household PM and mainly releases fine and ultra-fine (<1 mm in diameter) particulates.10
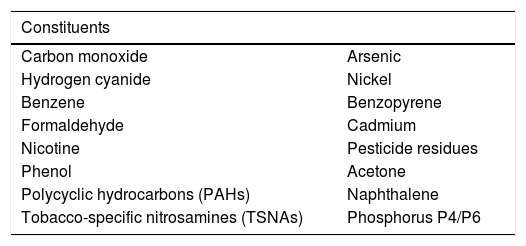
Most cigarettes' basic components are tobacco, chemical additives, a filter, and paper packaging. Smokers are exposed to a toxic mixture of more than 7,000 chemicals and up of more than 60 known carcinogens compound when they inhale cigarette smoke (Table 3), and the United States Food and Drug Administration has listed 93 of them.11
Main chemicals and chemical compounds identified as harmful and potentially harmful constituents in tobacco products and tobacco smoke.11
Besides the compounds found in tobacco leaves, artificial industrial additives are also incorporated to add flavor, reduce the irritation smoke causes in the respiratory tract, and enhance the effects of nicotine. Nicotine is considered a stimulant as it excites many brain cells. It is not as harmful as tar and CO, but it is addictive. The amount of nicotine varies depending on the cigarette, but the amount the smoker inhales is what matters. Smoking one cigarette results in the uptake of 1 to 2 mg of nicotine, which is reflected in mean arterial plasma concentrations of about 0.03 mg/L (30 ng/mL).11
Health impactAir pollutants exert their most harmful action on the respiratory system after inhalation. Both gaseous components (O3, VOC, CO, and NOx) and PM are well-established inflammatory stimuli to the mucosa of the respiratory tract. Depending on the aerodynamic diameter of PM, its action can occur at different points in the respiratory tract: PM10 is deposited in the nasal cavity and central airways.
Exposure to air pollutants can increase the adaptive immune response of T helper type 2 (Th2) and Th17 lymphocytes as in asthma and disrupt the antiviral immune response.12
Particle matter (PM)The role of PM in understanding the damage of respiratory epithelial cells occurs via a toll-like receptor (TLR) 4 pattern recognition and/or TLR2 activation via NFk-B signaling and NLRP3 inflammasome resulting in induced production of the pro-inflammatory mediators – interleukin (IL)-1a, IL-1b, IL-6, CXCL8, and colony-stimulating factor (GM-CSF).6,12 The PM10s and PM2.5s lead to the activation of the NLRP3 inflammasome via the production of reactive oxygen substances (ROS) and, consequently, alveolar macrophages, neutrophils, and dendritic cells.6,12 Once processed by dendritic cells, the antigens will be introduced to T lymphocytes and, depending on co-stimulatory molecules released by dendritic cells, a Th1- or Th2-type immune response will be established. Thus, in short, PM will lead to airway inflammation (Figure 1).12

Interaction between particulate matter and immune system cells involved in respiratory tract homeostasis – Adapted from Glencross et al., 2020.12
Additionally, exposure to fine particulate matter (PM2.5) was linked to altered methylation of most CpG sites for the important immunoregulatory genes FOXP3, IL-4, IL-10, and IFNγ. Their dysregulation has a high potential to cause loss of epithelial barrier integrity, DNA damage, oxidative stress, mitochondrial damage, changes associated with pulmonary fibrosis.13,14 Exposure to PM, even subchronic, in mice leads to alterations in both the lung and intestinal microbiome (dysbiosis), leading to lung and intestine damage and systemic inflammation impact the development of allergic disease over the lifespan.13-16
O3 exposure's direct action on the respiratory epithelium induces the release of cytokines and arachidonic acid metabolites, the leukotrienes formed from the cycloxygenase and lipoxygenase activity, which impairs mucociliary depuration and increases the production of free radicals.17
Climate change and microbiomeClimate change and environmental air pollution also determine changes in the environmental microbiota, which in turn is reflected in the infant's colonization and, consequently, in its microbiota: cutaneous, respiratory, intestinal, among others.18 This dysbiosis can be followed by significant changes in the infant's immune system, such as altered TLR expressions, altered T-cell function, altered antiviral responses, and altered allergic sensitization.18 Many of these changes are believed to be due to epigenetic changes, acquired in utero and transmitted to subsequent offspring, and by co-exposure to allergenic and non-allergenic stimuli. The airway microbiota has acute and long-term effects on respiratory health, while the intestinal microbiota influences airway health indirectly through the gut-lung axis.18
The gastrointestinal tract can also be involved with air pollution, just like the respiratory and cardiovascular tracts, although there is controversy among researchers. Experimental studies with animals that received high doses of urban PM by gavage showed increased intestinal permeability due to loss of tight junctions between enterocytes, increased IL-6 expression, and apoptosis of colon epithelial cells. Prolonged exposure to PM10, in addition to the previous alterations, determined alterations in the intestinal microbiota and in the homeostasis of fatty acids. Furthermore, PAHs, components of air pollutants, can significantly interfere in the balance between aryl hydrocarbon receptor (AhR) ligands derived from commensal bacteria in the gastrointestinal tract and from regulatory Th cells and epithelial Th17,12 a critical step for the onset of inflammatory bowel disease and food allergy.19
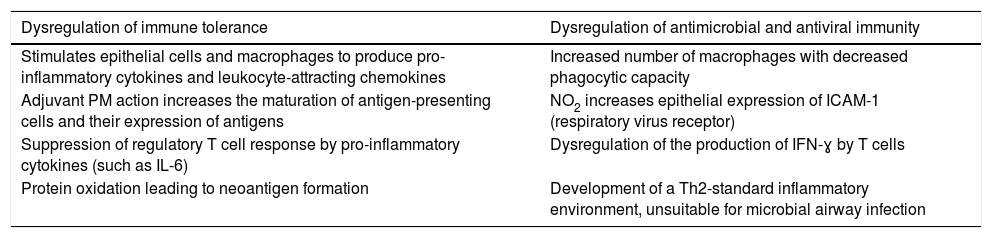
The action pollutants have on the cells of the immune system compromises the immune tolerance mechanisms and the antiviral and antibacterial defense mechanisms, making infections by respiratory agents more frequent (Table 4).12
Changes in immune tolerance and antimicrobial response due to air pollution.12
PM, particulate matter; NO2, nitrogen dioxide; ICAM-1, intercellular adhesion molecule 1; IL-6, interleukin 6; IFN-ɣ, interferon gamma.
Genetic predisposition combined with environmental exposure to inhaled substances that affect the airways is the strongest risk factor for developing asthma. In recent years, robust epidemiological evidence has shown that air pollution not only affects patients with pre-existing asthma but can also act to initiate it.20 Furthermore, a given individual subjected to the set of all exposures to the external environment from preconception onwards will suffer the consequences of these exposures at the cellular and organ level.21
Prenatal exposureThe impacts of exposure to air pollution during the prenatal period can affect organogenesis and the development of organs (i.e., the lungs), which can lead to long-term complications, affecting respiratory health in different manners.22
Recent studies have shown the accumulation of black carbon on the fetal side of the placenta, suggesting that environmental particulates can be transported to the fetus and represents a potential mechanism that could explain the detrimental health effects of pollution from early in life.23
Exposure during pregnancy (24th to 36th weeks) at 2 μg/m3 or more than PM2.5 during the saccular phase of lung growth was associated with a 1.29-fold higher risk of asthma (95%CI: 1.06-1.58), current asthma (RR: 1.27; 95%CI: 1.04-1.54), but not current wheezing.24,25 Impaired lung development also contributes to infant mortality.22-26
Exposure to PM10 from heavy road traffic during pregnancy was associated with significant reductions in lung function.23 Maternal exposure to traffic-related NO2, especially in the first trimester of pregnancy, has been associated with an increased risk of developing asthma, rhinitis, and eczema in children.27
Components of cigarette smoke are potentially toxic to the developing fetus, including lead, nicotine, cotinine, cyanide, cadmium, mercury, CO, and PAH. CO reduces the fetus's supply of O2, leading to hypoxia since it binds to hemoglobin with an affinity 200 times greater than O2 and makes it difficult to release the O2 to the cells. Chronic mild hypoxia of fetal tissue may persist for five to six hours after the mother has stopped smoking.28
A recent meta-analysis evaluated the deleterious effects of exposure to tobacco smoke during pregnancy, associated with harmful effects on the fetus and the newborn in the first two years of life.29 Regarding the respiratory system, exposure during pregnancy and passive exposure after birth was associated with increased risk of wheezing in children under two years of age, higher frequency of respiratory tract infections in children under two years (including bronchiolitis, pneumonia, bronchitis, pulmonary tuberculosis, otitis media), and increased risk of developing asthma.29 It is thought that at the epigenetic level, exposure to tobacco smoke during pregnancy may alter DNA methylation and messenger RNA expression in placental tissue, which may determine alterations in the expression of genes that affect the development of health conditions in the offspring.30
Early life exposureExposure to PM has been associated with impaired lung function in children, documented by the decrease in peak expiratory flow rates and forced expiratory volume in the first second, especially among asthmatic children, and clinically externalized by the increase in the number of exacerbations, visits to emergency rooms, hospitalizations, and child deaths.31,32
Exposure to PM10 and NO2 has been associated with reduced eosinophilic and neutrophilic inflammation of the respiratory mucosa in children with no wheezing. On the other hand, prolonged exposure to PM10 has been associated with eosinophilic inflammation in children with wheezing, suggesting that it may contribute to developing asthma, inflammation, and promoting airway remodeling.33
Passive exposure to tobacco smoke or nicotine-releasing devices has been associated with an increased risk of wheezing and asthma in children.29
c) Pollution and allergic sensitizationThe increase in global warming-related to climate change is associated in changes in pollen seasons, making them longer.34 Scientific evidence shows that components of air pollution may also interact with airborne allergens and enhance the risk of atopic sensitization and exacerbation of symptoms in sensitized individuals. PM, O3, CO2, Diesel Exhaust Particles, SO4, and NOX have been shown to enable the release of pro-inflammatory mediators that can accelerate IgE-mediated sensitization and allergy of susceptible subjects. Additionally, air pollution has been shown to increase pollen allergenicity.35,36
Although house dust mites (HDMs) and fungal spores are important sources of allergens inducing asthma and rhinitis, which are very sensitive to microenvironment modifications. Therefore, global or regional changes in temperature, humidity, air pollution, or other environmental conditions could modify natural HDMs and molds growth, survival, and allergen production.37 Consequently, sensitization to HDMs and molds has increased in some regions of the world, especially in the subtropical and tropical areas.38,39 The synergistic effects between extreme heat and aeroallergens intensify the toxic effect of air pollutants, which in turn increases the allergenicity of aeroallergens.39
Allergic rhinosinusitisEnvironmental air pollution has been one of the causes indicated by the increased prevalence of allergic rhinosinusitis (AR). Norbäck et al. studies point out that prenatal exposure to high levels of NO2 is associated with increased prevalence of AR in offspring.40
Prenatal and postnatal exposure to elevated levels of NO2 and PM10 were associated with an increased prevalence of rhinitis and a lower frequency of wheezing remission. Having mold, humidity, and cockroaches in the home was associated with an increase in the prevalence of wheezing, and cooking using gas was associated with an increase in the appearance of rhinitis.40
Exposure to indoor and outdoor allergens is a well-established risk factor for developing AR and more severe forms, especially indoor exposure.17 On the other hand, exposure to traffic-related air pollution (TRAP) for inducing oxidative stress and affecting the dendritic-T-cell epithelial cell axis towards a Th immune response2 justifies the relationship between these types of exposure and the development of AR.41
Atopic dermatitisHuman skin acts as a protective biological shield against pro-oxidant chemicals and air pollutants. As the largest organ in the body, it is constantly exposed to compounds in the surrounding environment. The evidence relates exposure to many environmental factors, either in high concentrations or for a long time, such as ultraviolet (UV) radiation, ambient air pollutants (PAH, VOC, MP, heavy metals, gas pollutants [CO, NOx, SO2, O3]) and indoor air pollutants (consumption of solid fuels, tobacco smoke) to the loss of the barrier function exerted by the skin.42,43
Damage to the skin barrier also appears to be closely related to increased production of reactive oxygen species (ROS), induction of oxidative stress, activation of the AhR, and inflammatory cytokines associated with precocious extrinsic aging and increased incidence of psoriasis, acne, atopic dermatitis, and skin cancer.42,43 VOCs have been associated with a higher prevalence of atopic dermatitis.43
The mechanism by which air pollution contributes to the development and exacerbation of atopic dermatitis is still unknown. An experimental study on mice with atopic dermatitis documented an accentuation of the skin condition when exposed to ovalbumin and PM10. There was an increase in clinical severity scores, transepithelial water loss, and epidermal thickness compared to the group without intervention. Several genes associated with cutaneous inflammation were detected for regulation. According to the authors, PM10 induced/aggravated skin inflammation due to the differential expression of genes controlling the integrity of the skin barrier and immune response.44
Eye allergyAlthough the respiratory system is the main one affected by the harmful effects of air pollutants, the ocular surface is also affected because it is directly exposed to various environmental factors and pollutants, internal and external.45 The dense innervations on the ocular surface are very sensitive to environmental chemicals, and only a thin teary film protects human eyes, often insufficient for preventing the development of symptoms of conjunctivitis or dry eyes following exposure.45
The correlation between exposure to high levels of O3 and an increase in ambient temperature with the presentation pattern of the recent ocular allergy and an increase in its prevalence has been documented.46
Besides affecting allergic diseases, the inflammatory response associated with air pollution may contribute to other conditions such as cardiovascular disease, hypertension, malignancy, Alzheimer's disease, dementia, cognitive impairment, and stroke.47,48
ConclusionsThe advances achieved in the Anthropocene period (from the 1950s onwards) have taken a heavy toll on us, given the climate changes it generated. These changes will undoubtedly have profound, acute, and long-term detrimental effects on children today and in the future. Pediatricians could play a relevant role in a series of actions, such as implementing and promoting educational strategies for children and their caregivers. As pediatricians, we have a moral responsibility to ensure the health of children today and those born in future generations.
Study conducted at the Universidade Federal de São Paulo, São Paulo, SP, Brazil.




