

To describe the type of milk used to feed infants seen in private pediatric practices in Brazil. To evaluate the relationship between breastfeeding, type of delivery, and history of prematurity.
MethodsThis is a cross-sectional and observational study that included 4929 infants in the first year of life seen in private pediatric practices in the five geographic regions of Brazil. Mothers provided information about the type of milk used by their infant, the type of delivery (vaginal or cesarean), and whether the birth was premature.
ResultsBreastfeeding was the only source of milk for 56.1% (1546/2755) of infants in the first six months of life and 32.9% (716/2174) in the second. Of the infants who received other types of milk besides breastfeeding, there was a predominance of infant formula in 98.6% and 93.8% of the infants, respectively, in the first and in the second six months of life. Whole cow's milk was used by 0.7% (20/2755) of infants in the first six months and by 4.1% (90/2174) of infants in the second (p < 0.001). In the first six months of life, breastfeeding as the only type of milk was associated with vaginal delivery (OR = 1.79; p < 0.001) and not having a history of prematurity (OR = 2.48; p < 0.001).
ConclusionBreastfeeding was the only milk source for more than half of infants before 180 days of life. Birth by cesarean section and history of prematurity were negatively associated with breastfeeding as the only source of milk used in infant feeding.
The first 1000 days, starting from conception is a critical period to define the health of the human being throughout all stages of life.1,2 Human milk is the ideal and unparalleled food for newborns and infants. Exclusive breastfeeding must be adopted in the first six months of life. From six months of age, breastfeeding should be maintained in a complementary manner.1,2 In addition to its recognized role in reducing infant mortality, a literature review3 with metanalysis showed that breastfeeding protects children from infections, decreases the frequency of dental malocclusion, positively influences intelligence (evidenced by an increase in the intelligence coefficient), and probably provides a reduction in the future risk of being overweight or having type 2 diabetes.3 In addition to the benefits for the child, breastfeeding provides a longer interval between deliveries.3 For the mother, breastfeeding provides a 7% reduction in the risk of breast cancer, an 18% reduction in the risk of ovarian cancer, and a 32% reduction in the likelihood of developing type 2 diabetes.3
In recent decades, breastfeeding has been promoted not only by the World Health Organization1 but also by government institutions such as the Ministry of Health of Brazil4 and Medical Associations in several countries, including the Brazilian Society of Pediatrics.5
In Brazil, an increase in breastfeeding rates has been observed in the last three decades.6,7 Exclusive breastfeeding up to six months of life was observed in only 2.9% of infants in 1986, 23.9% in 1996, 37.1% in 2006, and 36.6% in 2013. These data were extracted from national population-based surveys in which 4782 children under five were evaluated in 1996, 5461 were under 5 years old in 2006, and 4215 were under 2 years old in 2013. The exact number of infants evaluated in 1986 is not reported.6 Thus, there is a positive and optimistic trajectory for breastfeeding in Brazil. It is also noted that there is still the possibility of increasing these rates.6–8
The scenario is different when considering the type of delivery. In Brazil, especially in the supplementary health system, the prevalence of cesarean delivery is very high and can occur in up to 90% of births, that is, a much higher value than the 15% of cesarean sections that according to the World Organization may be justified by medical indications.9 Cesarean section is considered a factor that can negatively affect breastfeeding, especially when performed before labor begins.10 On the other hand, cesarean rates may be associated with increases in preterm birth rates and iatrogenic prematurity.11,12 Therefore, information about the relationship between breastfeeding, type of delivery and history of prematurity can be a contribution to the planning of programs to promote breastfeeding.13
Thus, the periodic assessment of the types of milk used in infant feeding in different pediatric settings is a matter of great relevance for providing information to improve educational and public policies to increase the Brazilian rate of breastfeeding. This article, with data collected in 2018, aims to describe the frequency of breastfeeding in infants seen in private pediatric practices in the five geographic regions of Brazil. The relationship between breastfeeding, type of delivery and history of prematurity was also evaluated.
Material and methodsA cross-sectional and observational study that included infants in the first year of life seen at pediatric private practices in the five geographic regions of Brazil. Pediatricians' agreement for the survey to be performed in their private offices was previously obtained. The author's invitation for Pediatricians to participate in the survey was distributed by scientific consultants of the company that sponsored this study. The invitation was given to all pediatricians who are visited by scientific consultants independently of the geographic region. Scientific consultants had no participation in the recruitment of mothers and also had no contact with the mothers who were included in the study. Private practices in Brazil provide care to the complementary health system or to patients whose payment for the consultation is made directly to the Pediatrician. As the sole inclusion criterion, all infants aged 12 months or less who underwent a scheduled pediatric consultation were considered. The following exclusion criteria were defined: cardiac, neurological and genetic diseases; history of abdominal surgery; cow's milk allergy; gastroesophageal reflux disease and other serious illnesses. After signing the Informed Consent Form, mothers who agreed to participate in the study filled out the form with general information about the infant and the type of milk used for feeding their baby on the day of the survey. This information is part of a project aimed at assessing the prevalence of functional gastrointestinal disorders in Brazilian infants. The project was evaluated and approved by the Comitê de Ética em Pesquisa do Hospital da Criança Santo Antônio de Porto Alegre in the Rio Grande do Sul (Number: 95930318.3.0000.5683). All Pediatricians and mothers participated voluntarily and received no compensation.
Before the consultation with the Pediatricians, the mothers filled out an individual form with the following questions:
- -
Date of birth and sex of the infant;
- -
Type of delivery (two closed options): vaginal or cesarean delivery;
- -
If the infant was born premature (three closed options): yes, no, I don't know;
- -
Type of milk used for feeding her baby (five closed options): breast milk exclusively, breast milk and infant formula, breast milk and whole cow's milk (powdered or in natura), infant formula, and whole cow's milk (powdered or in natura)
- -
If other foods besides mother's milk, infant formula, or whole cow's milk have already been introduced in infant feeding (two closed options): yes and no.
The information in the individual forms was entered into an Excel spreadsheet (Microsoft, Redmond, USA) using the double-entry technique. Information on 5591 infants was included in the spreadsheet. However, information from 433 (7.7%) infants for whom the date of birth was not filled out correctly and 78 (1.4%) who had diseases that were part of the exclusion criteria was excluded. Another 151 (2.7%) infants whose mothers did not complete the answer about the type of milk used on the day of the survey were also excluded. Thus, the information of 4929 infants was analyzed.
Categorical variables were summarized by the number (n) and percentage (%). A two-sided p-value was used in all tests. A p-value lower than 5% was considered in all analyses. The Chi-square test was used to compare the proportions of independent groups. Relation between categorical variables was evaluated using prevalence ratio (95% confidence interval). Statistical analysis was performed using the Epi-Info 7.2.3.1 (Centers for Disease Control and Prevention, Atlanta, GA, USA) and Stata/SE 15.1 (Stata-Corp, 2017. College Station, TX: StataCorp LLC).
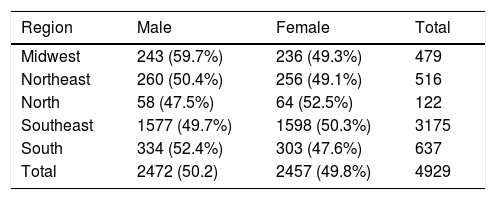
ResultsTable 1 shows the sex and geographic region of the 4929 infants included in the study. There was no statistically significant difference in the distribution by sex in the five geographic regions. Of the 4813 (97.6%) infants for whom information was available, 985 (20.5%) were born by vaginal delivery and 3828 (79.55) by cesarean section. History of prematurity was found in 483 (10.4%) of the 4629 (93.4%) infants for whom this information was obtained. The frequency of cesarean section in infants with a history of prematurity (81.0%; 384/474) was similar to that of other infants (80.0%; 3255/4069; p = 0.559).
Infants included in the study at private pediatric practices according to sex and geographic region of Brazil.
Chi-square test comparing simultaneously the proportion of the five geographic regions: p = 0.730.
Fig. 1 shows the number and percentage of infants, according to age and type(s) of milk(s) used on the day of the survey. In the first 180 days of life, 1546 (56.1%) infants received breast milk as the only milk source while 781 (28.4%) received mixed breastfeeding. In the second semester of life, breast milk was the only milk offered to 32.9% (716/2174) of infants. Of the infants who received other types of milk besides breastfeeding, there was a predominance of infant formula in 98.6% (484/491) of infants in the first six months and 93.8% (1368/1458) in the second semester of life. Whole cow's milk was used by 0.7% (20/2755) of infants in the first six months and by 4.1% (90/2174) of infants in the second semester of life (p < 0.001).
 of the type of milk used to feed infants in the five geographic regions of Brazil according to age.")
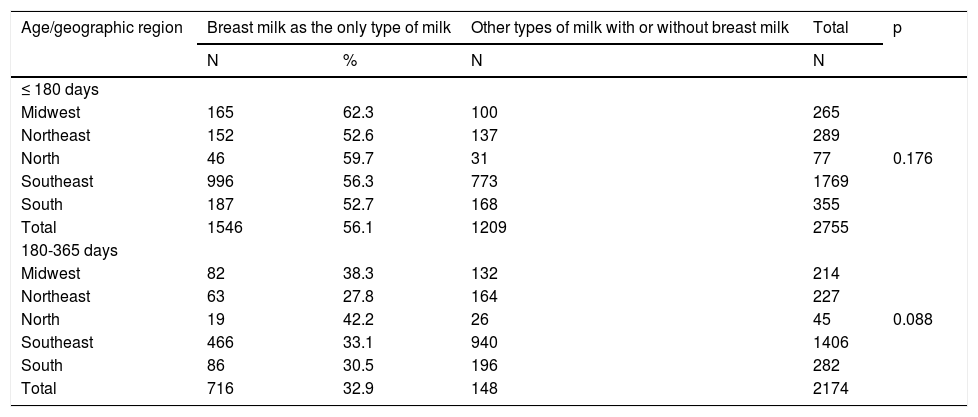
Table 2 shows the prevalence of infants who received only breast milk as the only source of milk according to region and age. The statistical study showed no difference between regions. However, grouping infants from the Midwest and North regions, the prevalence of breast milk as the only milk source was higher than in the set of Northeast, Southeast and South regions, both in the first 180 days (respectively: 61.7%; 211/342; 55.3%; 1335/2413; p = 0.030) as after 180 days of life (respectively: 39.0%; 101/259, 32.1%; 615/1915; p = 0.032).
Breastfeeding as the only type of milk offered to infants at private pediatric practices according to age and geographic region of Brazil.
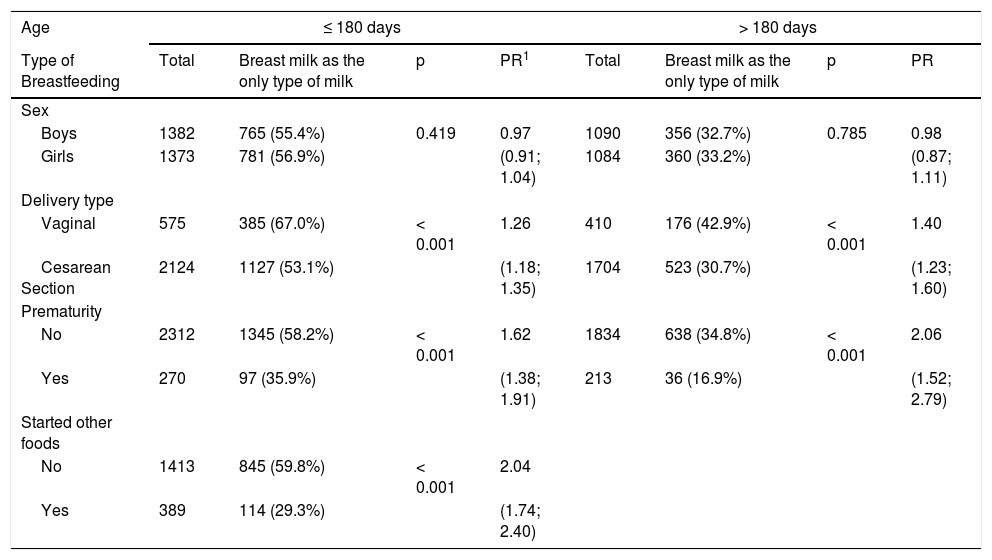
Table 3 analyzes the relationship between consumption of breast milk as the only source of milk and sex, type of delivery, history of prematurity, and onset of non-dairy foods. Statistical analysis included only infants for whom the data of the variable of interest was available. There was no association between infant feeding only with mother's milk and gender. Breast milk as the only type of milk was associated with vaginal delivery and not having a history of prematurity both in the first and second 180 days of life. The introduction of non-dairy food in the first semester of life was associated with not using breast milk as the only source of milk.
Relationship among breastfeeding as the only source of milk with sex, type of delivery, prematurity and introduction of non-dairy foods before 180 days of age.
PR, prevalence ratio.
95% confidence interval in parentheses. Information not available: Type of delivery: 56 aged up to 180 days and 60 aged over 180 days. Prematurity: 173 aged up to 180 days and 127 older than 180 days. Beginning of other foods: 953 aged up to 180 days.
Breastfeeding was the only type of milk used for feeding 56.1% of the infants in the first semester of life studied in private pediatric practices in the five geographic regions of Brazil. This percentage was approximately 7% higher in the Midwest and North regions compared to the other regions of the country. Between 9 and 12 months of age, 58.4% of infants received breast milk with complementary foods and/or other types of milk. Delivery by cesarean section and history of prematurity was associated with a lower chance of feeding infants only with mother's milk.
These data suggest that infants seen in the supplementary or private health system in 2018 are more likely to receive breast milk as the only milk source in the first six months of life than that observed in the country in 2006 and 2013 when breastfeeding rates were, respectively, 37.1% and 36.6% in the first six months of life.6 It should be warned that the comparison must be interpreted carefully considering that the strategy for data collection was not identical in the present and previous studies. In the surveys performed in Brazil in 2006 and 2013, it was assessed whether the infant had received breast milk in the 24 hours prior to the interview and whether he/she was not consuming water, tea and other types of food.6 In the present study, it was questioned whether the infant had already started other foods in addition to breast milk, infant formula or cow's milk. The data in Table 3 show that the introduction of other foods in the first six months of life is a factor associated with a lower likelihood of breast milk being the only type of milk used for infant feeding. However, a recent article highlights that breastfeeding data from the 2013 National Health Survey in Brazil might be imprecise since the interview date was not available preventing the definition of the exact age at the time of the interview.7 In the study's survey, the age of infants was calculated in days from the date of the interview and the date of birth. However, 433 (7.7%) of the 5591 interviews were excluded in which the date of birth was not included. It is interesting to mention that in the data tabulation it was observed that several mothers filled this field with their own date of birth. Despite these differences in methodology, the present study's results can be considered as an optimistic indicator of the positive historical evolution of breastfeeding rates in Brazil.
The use of breast milk as the only milk source for the infant was more frequent in the North and Midwest both in the first and second semesters of life. This regional difference had already been observed in Brazil in 2008 when exclusive breastfeeding was observed in 45.7% of the infants studied in the North, 44.8% in the Midwest, 43.7% in the South, 39.3% in the Southeast, and 36.9% in the Northeast.14 Data in Table 2 shows that the regional differences in this study study were similar to those observed previously.14
The present study showed that delivery of cesarean section was associated with less likelihood of the infant receiving mother's milk as the only milk source in both the first and second semesters of life (Table 3). In Brazil, the concern of the negative effect of cesarean section on the duration of breastfeeding has existed for almost four decades.15 Cesarean section has been shown to be associated with a shorter duration of breastfeeding at 316 and 617 months of life in addition to a lower proportion of newborns receiving breast milk in the first hour of life.18-22 Systematic review with meta-analysis involving more than half a million mothers showed that the onset of lactation before hospital discharge was lower after cesarean section (OR = 0.57).10 Lower rates of breastfeeding, exclusive (OR = 0.81; p = 0.03) or supplemented (OR = 0.86; p = < 0.001), were found at 6 months of age when delivery was by cesarean section.10 However, the rate was different when considering whether cesarean section was indicated before (OR = 0.83; p < 0.00001) or after the start of labor (OR = 1.00; p = 0, 86).10 This important aspect had already been highlighted in a survey conducted in Pelotas in 1993.16 Therefore, it can be inferred that the negative effect of cesarean section on breastfeeding is directly related to the nature of its indication. In this context, it should be noted that a better understanding of the effects of planned and emergency cesarean sections on the physical, psychological and emotional aspects of lactation is necessary to guide measures that mitigate this serious public health problem.13 In the present study, 79.6% of infants were born by cesarean section. According to a World Health Observatory data repository, the birth by cesarean section in Brazil is 55.5%.23 The higher value of cesarean sections in this study, is probably related to the fact that the families of the studied infants had access to complementary health programs in which cesarean sections are most frequently indicated.24,25 Therefore, in this study, it can be speculated that the high frequency of cesarean sections probably depends on indications made before the start of labor that has the most striking negative effect on breastfeeding.10,13,16 In the present study, the prevalence ratio shows that the negative effect of cesarean section on breastfeeding was greater than the systematic review mentioned above. On the other hand, the history of prematurity in the present study was 10.43% (483/4629), which is similar to the rate observed in Brazil.23 The results of the present study showed no statistically significant association between cesarean delivery and prematurity. However, there was less chance of using breast milk as the only food in newborns who were born prematurely. This result may be the result of the particularities of premature infants regarding their development, including feeding, and the care that may have been necessary for the neonatal period. This topic, due to its relevance, should be explored in future studies with a specific design to analyze the issues involved in this process.
Another factor negatively associated with the use of breast milk as the only milk source in the first 180 days of life was the introduction of other foods (Table 3). The cross-sectional nature of the present study does not allow the authtors to define the existence of a relation of causality between these two variables. However, the recommendations are explicit that exclusive breastfeeding provides adequate growth and development in the first six months of life.4,5
The present study (Fig. 1) showed that cow's milk was used for only 107 infants (4.01% of the 2667 infants who received another type of milk besides mother's milk). There are little information on the types of milk used by Brazilian infants.26 A survey performed in 12 Brazilian cities in 2008 evaluated the type of milk used in infant feeding.26 Cow's milk was used in the feeding of 31.1% of infants in the first six months of life and in 83.8% in the second. Mothers were responsible for the decision of introducing cow's milk in infant feeding.26 On the other hand, in the present survey, in private pediatric practices, the number of infants receiving whole cow's milk was much lower respecting the recommendations that whole cow's milk should not be used in the first year of life.4,5
One of the strengths of the present study is the sample size. Although the sample size estimate was directed to another research objective (gastrointestinal symptoms in infants), the number of infants included in the survey is similar to that of other studies conducted in Brazil and allowed the characterization of factors associated with the use of breast milk as the only milk source in the first year of life. The composition of the sample was for convenience, including infants from the offices in which the invited pediatricians agreed to collaborate with the execution of the research. Despite this strategy adopted to compose the sample, the proportion of infants studied in each geographic region approached the distribution of the Brazilian population (41.8% in the Southeast region, 25.5% in the Northeast, 14.3% in the South, 8, 7% in the North and 7.7% in the Midwest) according to data from the Brazilian Institute of Geography and Statistics.27 On the other hand, one of the limitations of the study was the recruitment of infants only in private pediatric practices of the complementary and private Brazilian health system. It should be highlighted that only 20% of the Brazilian population, mostly from the highest socioeconomic strata, are seen in pediatric private practices. Therefore, the results obtained in the present study cannot be extrapolated to Brazilian infants of all socioeconomic statuses. Another limitation refers to the history of prematurity that was informed by the mother and was not confirmed in a specific medical record, however, the rate of premature births was similar to that reported in Brazil.
In conclusion, mother's milk was the only source of milk used in the first six months of life for more than half of the infants. In Brazilian private pediatric practices, whole cow's milk was rarely used in infant feeding both in the first and in the second six months of life. The delivery rate by cesarean section was very high and was associated with a lower likelihood of breastfeeding. History of prematurity was negatively associated with breastfeeding as the only source of milk used in infant feeding.





