


To investigate the association of blood pressure and body mass index, waist circumference, waist-to-height ratio and triceps skinfold, in children and adolescents in Curitiba, state of Paraná, Brazil.
MethodsCross-sectional study with a random sample of 1,441 students from public schools, aged from 10 to 16 years (655 boys and 786 girls). The following indicators were assessed: weight, height, waist circumference, triceps skinfold, systolic and diastolic blood pressures, pubertal stage, and socioeconomic status. Pearson correlation tests and multivariate logistic regression were used, considering p<0.05.
ResultsWe found weak correlations among all the anthropometric parameters and systolic and diastolic levels, with coefficients values ranging from 0.18 to 0.28 (p<0.001). In multivariate analysis, only body mass index [odds ratio (OR)=2.9; 95% confidence interval (95%CI) 1.9-4.5] and triceps skinfold (OR=1.9; 95%CI 1.3-3.1) were found as predictors of high blood pressure, regardless of abdominal adiposity, sexual maturation and socioeconomic status.
ConclusionTotal body adiposity seems to be a better predictor of high blood pressure risk than abdominal fat in this population.
Investigar a relação entre pressão arterial e índice de massa corporal, circunferência abdominal, razão cintura/estatura e dobra cutânea tricipital em crianças e adolescentes.
MétodosEstudo epidemiológico transversal, do qual participaram 1.441 escolares de 10 a 16 anos de idade (655 meninos e 786 meninas), selecionados por amostragem aleatória sistemática. Avaliaram-se a massa corporal, a estatura, a circunferência abdominal, a espessura da dobra cutânea tricipital, as pressões arteriais – sistólica e diastólica – o estágio maturacional e a classe econômica. Utilizaram-se os testes de correlação parcial de Pearson e a regressão logística multivariada, considerando-se p<0,05.
ResultadosTodos os indicadores antropométricos demonstraram fracas correlações com os níveis sistólicos e diastólicos, com coeficientes (r) variando de 0,18 a 0,28 (p<0,001). Na análise multivariada, os únicos preditores antropométricos associados ao risco de pressão arterial elevada foram o índice de massa corporal (OR=2,9; IC95%: 1,9-4,5) e a dobra cutânea tricipital (OR=1,9; IC95%: 1,3-3,1), independentes da adiposidade abdominal, maturação sexual e nível econômico.
ConclusãoNesta faixa etária, a adiposidade corporal total parece ser melhor determinante do risco de elevação da pressão arterial do que a adiposidade abdominal.
Obesity and excessive central fat are changes that precede the increase in blood pressure in children and adolescents, according to epidemiological investigations that used high-precision technologies for estimating body adiposity.1 However, due to the high cost, limited feasibility and the risks of radiation exposure provided by these resources, researchers investigate the predictive ability of anthropometric indicators, aiming to use methods that are simpler, practical, and cost effective in assessing the risk of high blood pressure in children and adolescents.
Since the 70s, several studies showed body mass index (BMI) as the best predictor of high blood pressure in childhood and adolescence.1–4 Further investigations also considered BMI an important marker in the relationship between blood pressure and central adiposity indicators.5,6 On the other hand, the accumulation of adipose tissue in the central region of the body has been considered as a better determinant for the development of high blood pressure than total adiposity.7
Currently, however, there is no consensus on the choice of anthropometric predictor of high blood pressure in this population. Anthropometric indicators such as BMI, waist circumference, triceps skinfold and, more recently, the waist-to-height ratio, have been investigated for validity in predicting the risk for high blood pressure in the pediatric population.3,8 Therefore, this study aimed to investigate the best anthropometric determinants of high blood pressure in children and adolescents.
MethodsThis cross-sectional epidemiological research was conducted in 2008 and 2009, after a pilot study. The sample was extracted from school children attending 5th to 8th grades distributed into five regionals administered by the Municipal Secretariat of Education of Curitiba (n=8,140), and was selected by systematic sampling, in two stages:
- 1)
Selection (draw) of one school in each regional;
- 2)
Invitation of all school children and explanations about the study.
The sample size calculation (Epi-Info version 3.5.1) resulted from the sum of the samples calculated for each regional (n=1,523), for which we considered: number of students enrolled in each regional; unknown prevalence (50%); level of confidence of 95% (95%CI); and sampling error of 5%. The evaluations were performed only on students who agreed to participate and who presented the informed consent signed by parents/guardians (n=1,497). Out of these, 46 individuals were excluded for the following reasons:
- 1)
age different from 10 to 16 years;
- 2)
not having performed all assessments;
- 3)
use of drugs and/or presence of disease that could alter the levels of blood pressure.
The final sample was composed of 1,441 children and adolescents, 655 boys and 786 girls. The sampling error in each regional, calculated a posteriori, ranged from 1.2 to 1.5, below the level established a priori (5%).
The assessments were performed during the school period, by trained evaluators and using calibrated equipment. The techniques to measure body mass and triceps skinfold were obtained according to international norms,9 considering valid the average of three measurements. Height was measured with a wall stadiometer (Wiso®, Brasil) with a resolution of 0.1cm, and body mass was measured in digital scale, (Plenna®, Sport, Brazil) with a maximum capacity of 150kg and a resolution of 100 grams. The assessed student wore only the school uniform, without coats or objects in the pockets.
BMI (kg/m2) was used to classify students as having adequate weight and overweight.10 Data from children with low birth weight (1.2%; n=18) were included in the adequate weight category.
Subcutaneous adiposity was estimated by triceps skinfold thickness, using scientific plicometer (Cescorf®, Brazil) with a resolution of 0.1mm. Its classification was based on the reference curve and National Health and Nutrition Examination Survey I (NHANES I)11 and considered high (obese) when corresponded to values equal or above the 90th percentile.12
Waist circumference was obtained with the use of flexible and inextensible tape measure (Gullik®, Brazil), with resolution of 0.1cm, applied immediately above the iliac crests. For classification of abdominal obesity, we used the cutoff for all ethnicities (waist circumference ≥ 75°).13 Abdominal obesity was also diagnosed by waist-to-height ratio (waist circumference/height), with cutoff values equal to or greater than 0.5.14
The determination of pubertal stage was based on self-assessment of pubic hair (P1-P5),15 once it is more reliable than genital self-assessment, in both genders, besides avoiding embarrassment and presenting greater operational convenience in relation to direct assessments.16 Schoolchildren were classified as pre-pubertal (no hairiness or P1), pubertal (hairiness P2-P4) and post-pubertal (hairiness P5). For the classification of post-pubertal stage in girls, reports of menarche were prioritized. The measure of blood pressure was performed according to the recommended techniques,17 using a mercury column sphygmomanometer (Wan Med®, Brazil). Three measures were obtained with a minimum interval of 2minutes between them, considering valid the mean value of the last two measures. High blood pressure was characterized by the values of systolic an/or diastolic blood pressure greater than or equal to the 90th percentile or to 120mmHg and/or 80mmHg.18
The economic class was identified by the Brazilian criteria of economic classification.19 Due to the low percentage of students in classes A (5.5%) and D (1.5%) and none in class E, the eight economic classes were grouped into classes A/B (classes A1, A2, B1 and B2), and C/D (classes C1, C2 and D).
In statistical analysis, the normality of data was confirmed by the Bivariate Correlation Test (MatLab, version 6.1), and the existence of disparate elements (outliers) through Boxplots. The outliers were included in the analysis because they corresponded to the data of obese or overweight subjects, which mattered for the study.
To compare the anthropometric and hemodynamic characteristics between genders, Student's t test was used for independent samples, investigating homogeneity of variances between groups using Lèvene's test.
In order to analyze the relation of the following variables: BMI, waist circumference, waist-to-height ratio and triceps skinfold thickness, among them and with arterial blood pressure (systolic and diastolic), Pearson's partial correlation test was used with adjustments for gender, age and sexual maturation.
Exploratory analysis of the data showed no linear relationship between x and y, from a certain point of its distribution, assuming logistic curve in S. We conducted, thus, the multivariate binary logistic regression, determining the odds ratio (OR) and the respective 95%CI, in order to examine the independent association of high blood pressure (dependent variable) with the categories od BMI, waist circumference, waist-to-height ratio, and triceps skinfold thickness (independent variables). The models were built by the method of unconditional retrograde probability and adjusted for all measures of adiposity, maturational stage and socioeconomic status (intervening variables).
All variables were dichotomized, and the criterion for inclusion of independent variables in the multivariate model was a level of association of p≤0.20 with the dependent variable, by the chi-square test.
Analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 13.0, considering p<0.05. This study was approved by the Research Ethics Committee of the Department of Health Sciences, Universidade Federal do Paraná, under protocol CEP/SD: 403.083.07.07, in accordance with the Declaration of Helsinki, and approved by the Municipal Education Secretariat of Curitiba, state of Paraná, PR.
ResultsBoys showed higher mean age, height, systolic and diastolic pressure than girls (p<0.05), which had higher average waist-to-height and triceps skinfold thickness (p<0.05). Mean body weight, BMI and waist circumference were similar between genders (Table 1).
General characteristics of the sample.
| Variables | Boys (n=655)Mean ± SD | Girls (n=786)Mean ± SD | Total (n=1441)Mean ± SD | p |
|---|---|---|---|---|
| Decimal age (years) | 12.7±1.5 | 12.5±1.4 | 12.59±1.4 | 0.001a |
| Body mass (kg) | 48.1±12.5 | 47.1±12 | 47.54±12.2 | 0.13a |
| Height (m) | 1.55±0.1 | 1.53±0.1 | 1.54±0.1 | < 0.001a |
| Body mass index (kg/m2) | 19.8±3.5 | 20±3.9 | 19.9±3.7 | 0.21a |
| Waist circumference (cm) | 69.9±9.2 | 70.6±9.2 | 70.3±9.2 | 0.137b |
| Waist-to-height ratio | 0.45±0.1 | 0.46±0.1 | 0.46±0.1 | < 0.001b |
| Triceps skinfold (mm) | 14.7±6.9 | 18.7±6.6 | 16.9±7 | < 0.001b |
| Systolic blood pressure (mmHg) | 107±12 | 105±13 | 106±12 | 0.003a |
| Diastolic blood pressure (mmHg) | 61±10 | 59±10 | 60±10 | 0.015a |
p, statistical significance; SD, standard deviation.
In the assessment of sexual maturation (n=1,439), prepubertal (3.8%, n=55), pubertal (64.1%, n=923) and post-pubertal (32%, n=461) students were identified. Comparing males (n=653) and females (n=786), there were higher proportions of prepubertal (5.2 vs. 2.7%) and pubertal (91 vs. 41.9%) between boys and more post pubertal among girls (3.8 vs. 55.5%) (chi-square=437.020, p=0.000).
Analyzing the relationship between the variables studied, it was found that all anthropometric indicators were strongly correlated (r=0.81 to 0.92, p<0.001), indicating collinearity between them. Anthropometric variables showed weak correlations with systolic and diastolic pressures, with coefficients ranging from 0.18 to 0.28 (Table 2).
Pearson (r) partial correlation for the studied variables, with adjustments for age, gender, and sexual maturation in school children from municipal schools in Curitiba, PR, Brazil.
| Variables | BMI | WC | WHR | TSF | SBP | DBP |
|---|---|---|---|---|---|---|
| BMI | - | 0.89a | 0.89a | 0.81a | 0.28a | 0.26a |
| WC | 0.89a | - | 0.92a | 0.82* | 0.26a | 0.24a |
| WHR | 0.89a | 0.92a | - | 0.83* | 0.19a | 0.19a |
| TSF | 0.81a | 0.82a | 0.83a | - | 0.22a | 0.18a |
BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure; TSF, triceps skinfold; WC, waist circumference; WHR, waist-to-height ratio.
From the multivariate analysis, it was found that the model with the highest predictive validity included BMI variables, waist circumference, triceps skinfold thickness, sexual maturation, and economic status (adjustment index from the Hosmer & Lemeshow model= 0.989), with ability to explain 83.3% of cases of adequate blood pressure, but not the cases of high blood pressure (17.3%).
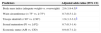
Then it was observed that the only variables associated with high blood pressure levels were BMI (p<0.001) and triceps skinfold (p=0.003), independently of abdominal obesity, sexual maturation and economic status. High BMI increased by almost three times the risk of high blood pressure among overweight schoolchildren (OR=2.9, 95%CI 1.9 to 4.5) when compared to normal weight children. On the other hand, the increased thickness of the triceps skinfold doubled the risk of high blood pressure (OR=1.9, 95%CI 1.3-3.1) compared to students with adequate thickness. Waist circumference, waist-to-height ratio, sexual maturation, and socioeconomic status were not associated with risk of high blood pressure (Table 3).
Multivariate odds ratio for risk of high blood pressure, adjusting for sexual maturation and economic status in school children from Curitiba, PR.
| Predictors | Adjusted odds ratios (95% CI) |
|---|---|
| Body mass index (adequate weight vs. overweight) | 2.9 (1.9-4.5)a |
| Waist circumference (< 75° vs. ≥ 75°) | 0.7 (0.5-1.2) |
| Triceps skinfold (< 90° vs. ≥ 90°) | 1.9 (1.3-3.1)b |
| Sexual maturation (P1 vs. ≥ P2) | 0.7 (0.3-1.4) |
| Economic status (A/B vs. C/D) | 0.9 (0.7-1.2) |
CI, confidence interval.
The prevalence of systemic blood hypertension in the juvenile population has increased around the world,20 with the highest proportion of hypertension observed in obese schoolchildren.21 Many studies were conducted to identify the best anthropometric determinant of high blood pressure in children and adolescents, but the results were divergent.2,6,22 The present study aimed to better clarify this issue, by examining the relationship between blood pressure and various anthropometric indicators of obesity.
The results showed weak correlations among all anthropometric parameters and systolic and diastolic levels, which has been observed previously3,23 regardless of gender, age and maturational stage. The strength of correlations may have been affected by several factors such as the multicollinearity observed in the data set, the multiple etiology of high blood pressure, influenced both by environmental and genetic factors,5 as well as by the logistic behavior of data.
The multivariate model, however, was able to explain only the cases of adequate blood pressure and not the changes, perhaps because of the largest percentage of adequate blood pressure (82.7%) compared to high blood pressure (17.3%) in the sample studied, which decreased strength in the explanation of changed data. It is noteworthy that the pressure measurements were taken on one occasion only, characterizing a limitation of this study and a possible classification bias.
This study showed that the only anthropometric indicators independently associated with blood pressure above the 90th percentile were triceps skinfold thickness and BMI, the latter being the most important determinant and independent of subcutaneous adiposity. Children and adolescents who are overweight were nearly three times more likely to have high blood pressure than eutrophic ones.
There is evidence that obesity increased the risk of pressure changes in children and adolescents24 and that BMI is the best anthropometric parameter to predict this risk.1–5 In clinical practice, however, there is no consensus on the use of BMI in monitoring cardiovascular risk factors, once besides body adiposity, BMI may represent different elements of the body composition.25
In this research, however, there was a strong relationship between BMI and peripheral (r=0.81, p<0.001) and central body fat (r=0.89, p<0.001), which may be due to a supposedly not very significant lean mass in the study population, judging by the high percentage of students in pre-pubertal (3.8%) and pubertal phases (64.1%). This relationship may have reflected on the superiority of BMI in predicting high blood pressure of school children in relation to other indicators analyzed. In other studies that identified BMI as the best determinant of high blood pressure in children and adolescents, its predictive ability was higher than that of skinfold measurements.2,3
It is believed that the use of critical values for the classification of national BMI10 gave greater credibility to the analyzes of this study, because these cutoff points exhibited greater accuracy in the determination of high blood pressure in boys and girls from 10 to 17 years compared to international references.26
Regarding the association between high blood pressure and triceps skinfold thickness observed in this study, the literature is sparse and divergent. In this study, the risk of high blood pressure was almost twice as high in children with triceps skinfold thickness above the 90th percentile than those with adequate subcutaneous adiposity. Other studies of systematic review23 and meta-analysis27 also confirmed the association between these variables. However, triceps skinfold in the upper quartile was not associated with risk of high blood pressure in children and adolescents of Belo Horizonte.2
Controversies between the results may also be explained by the different cutoffs used, causing differences regarding the classification of triceps skinfold thickness. Moreover, the shortage of studies on skinfold assessments in Brazilian schoolchildren, as well as the tendency to use the triceps skinfold thickness in combination with subscapular skinfold thickness22,23,25 are aspects that make it difficult to compare studies on the relationship between subcutaneous adiposity and cardiovascular risk factors.
An important aspect of this analysis was the observation that the triceps fold, alone, is able to predict the risk of high blood pressure. This finding is relevant in the context of epidemiological studies, because while the validity of subscapular skinfold for screening cardiovascular risk factors is recognized, there are some operational difficulties to obtain it, because it requires isolated environment to remove the girls’ shirts.
About the lack of association between blood pressure and waist circumference, some criticisms about the cutoff point used in this study may be highlighted, which may have distorted the risk estimates of high blood pressure.16 It is claimed that these are not sufficiently sensitive and specific for detecting high levels of blood pressure in Brazilian children and adolescents, due to the strong mixing characteristics of this population, which requires specific critical values, i.e., that are derived from references that have no ethnic distinction, such as in the international propositions.28
Some researches showed the superiority of waist circumference in detecting the variation on the values of blood pressure and proposed new cutoffs.23,29 However, their analyses were performed in populations of a different age group.
Regarding the waist-to-height ratio, the fact that it is not associated to blood pressure in this research differs from significant associations mentioned in literature.3,25,29 The reason may be the cutoff used in these studies, which was adequate to the studied sample (tertiles or quartiles), unlike the present study, which used the critical value currently recommended.
Recent research has recognized the cutoff point of 0.44 for predicting lipid abnormalities in children and adolescents.4 Perhaps the ideal cutoff limit for the detection of blood pressure increase is also smaller than the current one, because this has not been validated for the diagnosis of abdominal obesity in the juvenile population.14 Therefore, it is possible that we have underestimated the cases of abdominal obesity, masking the relationship of blood pressure with waist-to-height ratio.
Despite discussions about the validity of its cut-off point, the waist-to-height ratio was associated with several cardiovascular risk factors such as high blood pressure.7,30 It is an index that is representative of visceral fat,7 its classification is independent of age, gender, and ethnicity, and it has the advantage of considering the effect of height on the variation in waist circumference during the growth period and throughout childhood and adult life.14
However, it is essential that new studies seek to investigate the use of waist-to-height ratio during the growth spurt, because increased waist circumference cannot keep up with the rapid height gain in pubertal stage, hindering the diagnosis of abdominal obesity when the measure of waist is corrected by height.
The lack of association between high blood pressure and abdominal adiposity indicators in this study does not rule out their relevance in the context of juvenile hypertension because they were correlated with systolic and diastolic levels, suggesting a predictive potential. The period to which the students were exposed to excessive abdominal adiposity may not have been sufficiently prolonged to the point of causing increases in blood pressure levels, which may explain the present results. The validation of their cutoffs in the pediatric population is needed, because it will allow further studies with more reliable reference values.
BMI and triceps skinfold thickness were the best determinants of risk of high blood pressure, regardless of abdominal adiposity, sexual maturation stage, and socioeconomic status. The need for routine measurement of blood pressure within the school environment comes across difficulties such as having adequate equipment and mastering the measurement techniques. Therefore, the estimation of high blood pressure by anthropometric predictors in cross-sectional studies allows the stratification of this risk in a simpler and no less reliable way. Considering the easy technique required to obtain the measures of weight and height and the low cost they involve, the use of BMI seems to be the best option in this context.
FundingCoordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Programa de Apoio a Planos de Reestruturação e Expansão das Universidades Federais (REUNI) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Conflicts of interestThe authors declare no conflicts of interest.
We thank the financial support received from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Programa de Apoio a Planos de Reestruturação e Expansão das Universidades Federais (REUNI) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Please cite this article as: Moser DC, Giuliano IC, Titski AC, Gaya AR, Coelho-e-Silva MJ, Leite N. Anthropometric measures and blood pressure in school children. J Pediatr (Rio J). 2013;89:243–9.





