
Suspicion of early anterior fontanel (AF) closure is a common reason for referral to a pediatric neurosurgeon because of the suspected increased risk of developing craniosynostosis (CS) in spite of the absence of evidence in the literature. The aim of this study was to analyze the association between AF closure and the diagnosis of non-syndromic CS in Brazilian children.
MethodsAn observational and case-cohort study was conducted to compare the incidence of closed AF between healthy children (group 1) and children diagnosed with non-syndromic CS (group 2) at a pediatric neurosurgery referral center. The accuracies of completely closed AF and diagnosis of CS were assessed.
ResultsHigh-resolution three-dimensional reconstruction computed tomography scans were obtained for 140 children aged < 13 months, of whom 62.9% were boys and 37.1% were girls (p < 0.001). The most common types of non-syndromic CS were trigonocephaly (34, 48%) and scaphocephaly (25, 35.7%). Closed fontanel (27, 38.6%) was observed in both groups, and a sensitivity of 36.1%, specificity of 72%, the positive predictive value of 59%, and negative predictive value of 51% were observed in the patients diagnosed with CS when AF closure occurred before the age of 6 months.
ConclusionThe results of this comparative study of AF closure and CS diagnosis suggest that early AF closure does not imply a diagnosis of CS. Pediatricians should be aware of the risk of misdiagnosis of CS in cases with a widely open AF in spite of the presence of CS.
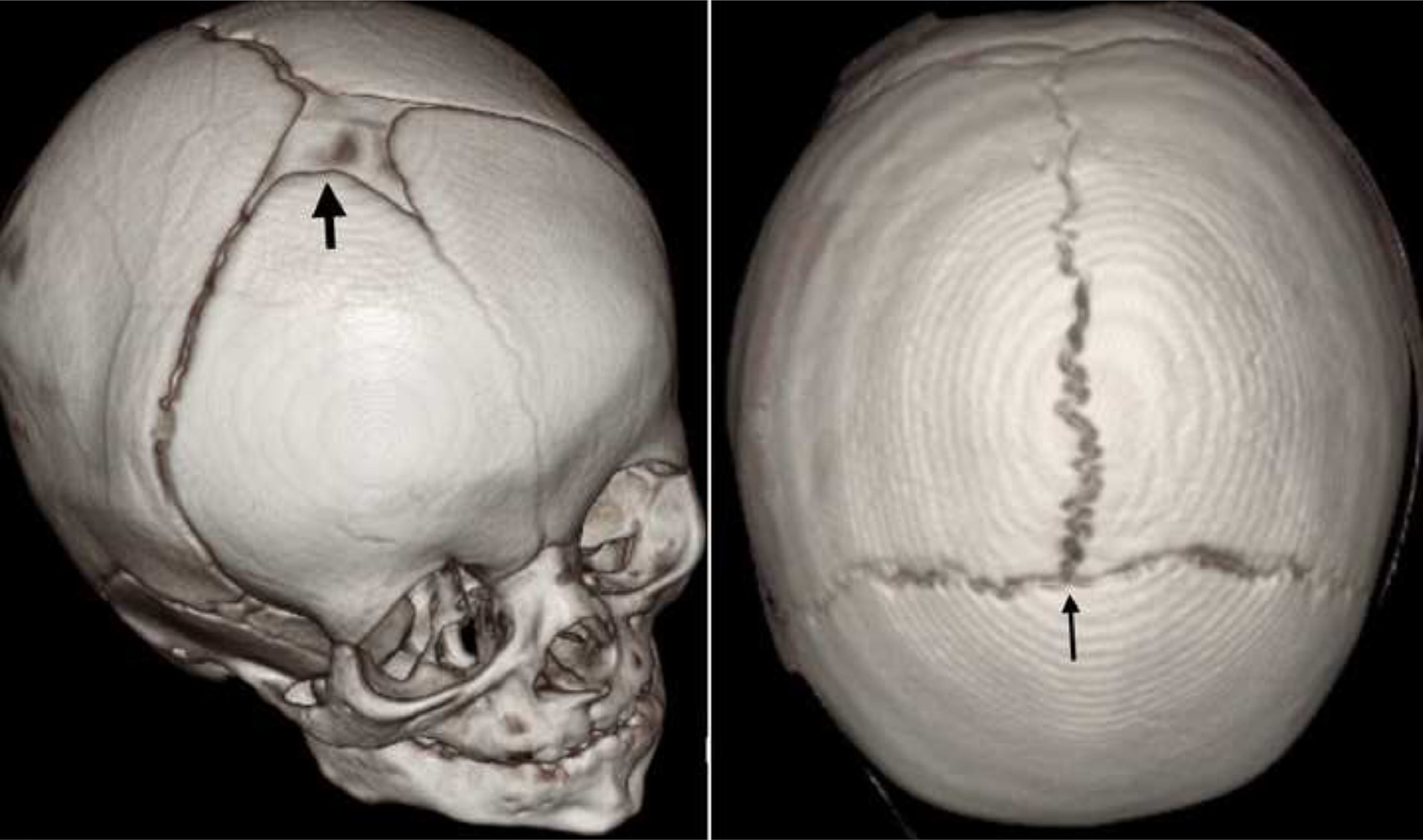
The anterior fontanel (AF) is the largest and most important of the six fontanels in the newborn skull. Embryologically, it is composed of a connective tissue derived from the neural crest, that is, the ectomeninx, which has membranous remnants.1,2 Anatomically, AF is described as a diamond-shaped structure on the cranial vault at the convergence of the metopic, sagittal, and coronal sutures (Figure 1).3,4 Traditionally, the primary function of the fontanels is to allow the overlap of the cranial vault bones during birth, but the fontanels play no role during skull growth. This function has been attributed to the sutures of the skull, whose early fusion could lead to craniosynostosis (CS). CS is classified as either syndromic if associated with craniofacial syndromic conditions such as Crouzon and Apert syndrome and commonly presents with skull base restriction and midface hypoplasia (incidence: 1 in 30,000 live births) or non-syndromic if no such syndromes are identified (incidence: 1 in 2,000 live births).5-7
 or closed or fused (thin black arrow) in a 4-month-old boy (right).")
Although AF closure before six months of age has been considered rare in several reports and is an indication of abnormal conditions such as hyperthyroidism, aberrant cerebral development, microcephaly, and even CS, no strong evidence of the association between CS and early AF closure has been obtained thus far. The judgment of fontanel abnormality in such patients is a common reason for referral to a pediatric neurosurgeon, which could lead to unnecessary radiation exposure due to computed tomography (CT) scanning.8-12 Furthermore, AF closure is dependent on factors such as ethnicity and sex, and several studies have considered it to occur during the first 24 months after birth, more specifically within 13 and 16 months of age.10,13-15 By contrast, other studies found healthy children with AF closure at ages < 76 days.15,16 Thus far, the association between CS and AF closure has not been proven in large series, and no study has examined this yet.
Therefore, the aim of this study was to examine the relationship between AF closure and CS diagnosis in the Brazilian population in the state of Minas Gerais.
Materials and methodsStudy designData for this single-institution retrospective observational study were obtained from a prospectively maintained database and hospital charts and images of patients who attended a reference institute for pediatric neurosurgery in Nova Lima, Minas Gerais, Brazil between January 2020 and January 2021. This study was approved by the institutional ethics board and received appreciation from the government of Brazil (Plataforma Brasil; CAAE: 30620120.7.0000.5134). Furthermore, the manuscript adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.17
Eligibility criteriaChildren aged <13 months who were assessed at the institution between January 2020 and January 2021 were included in the study and divided into two groups. Group 1 was composed of children with no CS and no suspected diseases (e.g., microcephaly, hyperthyroidism, infection, hypoxia-ischemia sequelae, metabolic disorders, achondroplasia, osteogenesis imperfecta, intracranial hemorrhage, epilepsy, malnutrition, and oncological diseases) who have undergone neurosurgical procedures and were evaluated in the emergency department because of accidental mild head trauma and elected for CT scan in accordance with the protocol adopted for mild head trauma.18 All CT scans were of high resolution. Three-dimensional reconstruction images were obtained to rule out skull fractures, and the intracranial compartment was examined to exclude intracranial bleeding due to trauma. Group 2 included patients with non-syndromic CS who underwent skull reconstructive neurosurgery procedures during the study period by the same pediatric neurosurgery team and a CT scan with three-dimensional (3-D) reconstruction at the same institution.
For patients with suspected syndromic CS due to classical physical features such as exorbitism and maxillary hypoplasia, abnormalities of the ears, and syndactyly or fusion of multiple sutures on CT imaging or even early fusion of single sutures more likely associated with mutations such as anterior coronal and bicoronal CS, a consultation with the geneticist and evaluation for gene mutations were required. If any mutation was identified, the patient was excluded from the study even without physical features of syndromic forms. Therefore, patients with classical syndromic forms such as Crouzon, Apert, Pfeiffer, and Saethre-Chotzen syndromes and other syndromes were excluded. Furthermore, patients with brain disorders such as hydrocephalus, other brain malformations, or skull fractures and Wormian bones in the AF were excluded.8
Data collectionThe authors of the present study assessed data from the medical records of the hospital and private clinic where the interventions of the patients with CS ensued, such as age at attendance, sex, and those that warrant no exclusion factors. In addition, the patients’ images were obtained in the DICOM format and transferred to the OsiriX imaging program (OsiriX, Geneva, Switzerland),19 which was validated using ANVISA to ensure the use of the medical findings. The images were assessed by the senior author of this study, who assessed the normality of the brain and analyzed the skull surface using the 3-D reconstruction images in accordance with the following parameters: (1) if the AF was open or closed (open, all visible AFs independent of the size; closed, completely ossified or no fontanel in spite of all the sutures remaining open) and (2) the type of CS (Figure 1 and 2).
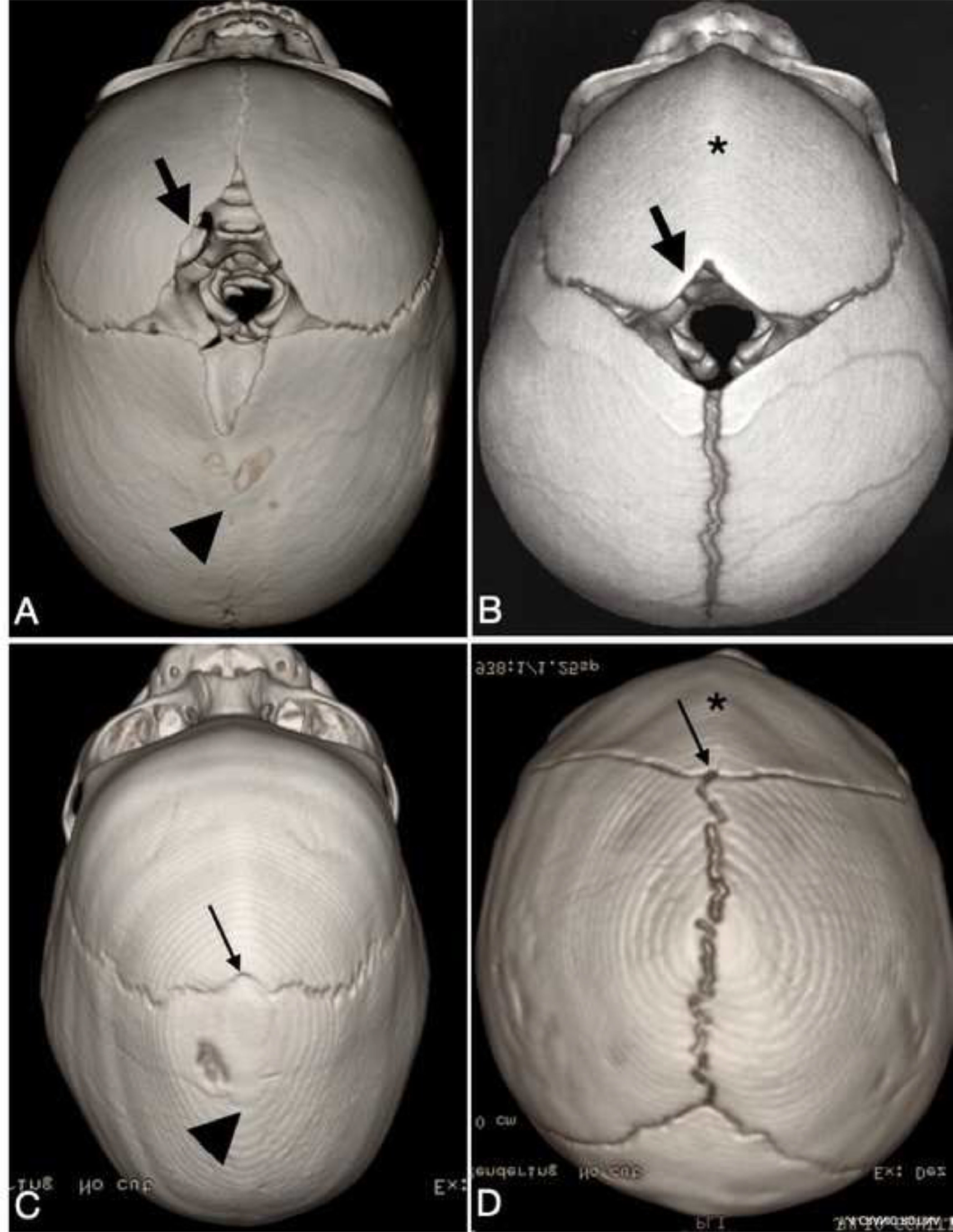
 could present as open (thick black arrow) or closed (thin black arrow). (A) A widely open AF is depicted in patients with (A) scaphocephaly and (B) trigonocephaly or (C) a completely fused AF in scaphocephaly and (D) trigonocephaly. The metopic suture is fused in trigonocephaly (*). The sagittal suture is fused in the scaphocephaly (arrowhead).")
Computed tomography image with three-dimensional reconstruction of the skull image in children with non-syndromic craniosynostosis, demonstrating that anterior fontanel (AF) could present as open (thick black arrow) or closed (thin black arrow). (A) A widely open AF is depicted in patients with (A) scaphocephaly and (B) trigonocephaly or (C) a completely fused AF in scaphocephaly and (D) trigonocephaly. The metopic suture is fused in trigonocephaly (*). The sagittal suture is fused in the scaphocephaly (arrowhead).
The SPSS version 20 (IBM Corp., Armonk, NY), Minitab 16 (Minitab Inc., State College, PA, USA), and Excel Office 2010 software programs (Microsoft, Redmond, WA, USA) were used for the statistical analyses. A confidence interval of 95% was applied. The two-proportion equality test (chi-square) was used to compare the rates among the covariates of age and sex. P values < 0.005 were considered statistically significant.
To calculate the sensibility, specificity, positive predictive value, and negative predictive value of AF closure in relation to the non-syndromic CS diagnosis, the authors considered the CT scan and clinical findings of CS as gold standards for the diagnosis of CS. Accordingly, the authors categorized the population of this study into those who were positive and those who were negative for CS and AF closure.
ResultsStudy populationDuring the study period, 140 children were assessed and distributed into the two groups. The overall sex distribution was as follows: 88 boys (62.9%) and 52 girls (37.1%) overall (p < 0.001), with 44 (62.1%) and 43 boys (61.4%) boys in groups 1 and 2, respectively (p > 0.005). The mean ages in groups 1 and 2 were 11.06 and 6.53 months, respectively (p = 0.047). In addition, the incidence of trigonocephaly was highest, followed by scaphocephaly, in group 2, as shown in Table 1.
Characteristics of the 70 children with non-syndromic craniosynostosis and their relative anterior fontanel (AF) closure proportions.
A completely open AF was observed in 86 patients (61.4%; p < 0.001; Table 1). The distributions of open and closed fontanels were identical in the two groups, wherein 43 patients (61.4%) had open fontanels (p = 1.00).
For closed AF, different age distribution was observed between the two groups; however, the CS group tended to have earlier AF closure (Table 2). The mean age at AF closure was 9.8 months (range, 3–13 months) in group 1 and 6.8 months (range, 1–13 months) in group 2. AF closure was found in 7 (26%) of the 27 children aged <3 months, in 27 patients (47.2%) between 3 and 8 months of age, and in 24 patients (40%) aged >8 months.
Despite the aforementioned high proportion of boys in both groups, no statistically significant differences were observed regarding AF closure and sex between groups 1 (p = 0.189) and 2 (p = 0.688).
The children with trigonocephaly were more susceptible to AF closure, accounting for 67.8% of this study population. Conversely, the children with scaphocephaly were less susceptible to AF closure, with 76% of them having an open AF at diagnosis.
AF fusion and accuracy of CS diagnosisFontanel closure in the patients aged <13 months presented a sensitivity of 38%, specificity of 61%, positive predictive value of 50%, and negative predictive value of 50% for predicting a CS diagnosis. In the patients aged <6 months, early fontanel closure presented a sensitivity of 36.1%, specificity of 72%, the positive predictive value of 59%, and a negative predictive value of 51% for the same purpose.
DiscussionDemographic influences of AF closureHistorically, although six months have been considered the cutoff age for early AF closure, no consensus has been reached as to the specific age for normal AF closure, and great variability has been reported. AF closure might occur after days,15,16 during the second month,20 after 3.7 months,21 after 6 months,2 and even after 13.8 months.11 In addition, this variability was attributed to ethnicity, sex, and ancestry.1,2,5,12,14,15 In the present study, normal Brazilian children presented an overall closure rate of 40%, with a mean age of 9.8 months. Likewise, the AF fusion rate in the Maõri/Pacifican population of New Zealand was 47% at 12 months compared with 24% in the English population. Boran et al.22 found a similar AF closure rate at a mean of 9.7 months in Turkish children. This pattern of closure could reinforce the role of ethnicity, especially in the Brazilian population, which consists of a mixture of Africans, Europeans, and indigenous Brazilians, displaying a trend toward early AF closure compared with European, Iranian, and Chinese children.2,13,23-25
Several studies have reported the influence of sex on AF closure in boys who presented with AF closure at an average of 1 month earlier than girls.26 By contrast, the present study adopted head trauma and CS as the inclusion criteria, with higher incidence rates in males than in females according to the literature, which explains the disparity between the sexes.18,27 Despite this fact, in a population that consisted mostly of boys, like other studies, our study did not show a statistically significant impact of sex on AF closure.2
AF closure and CS diagnosisEarly AF closure was observed in the CS group compared with the healthy population, explaining the abnormal ossification on the four sutures in association with AF, which was mainly found in the children with trigonocephaly and the most common type of CS in this study. In addition, this higher incidence rate is different from most studies, which showed scaphocephaly as the most common CS. The result of this study is in accordance with previous observations of changes in the epidemiology of CS with increasing incidence of trigonocephaly in the last two decades. Several risk factors have been reported, such as less folic acid intake, under the assumption that folic acid could prevent midline defects such as early metopic fusion. Another factor is valproic acid use during pregnancy and other environmental risk factors such as external pressure on the fetal skull, birth presentation, birth weight, gestational age, and mode of delivery.27-29
This discrepancy in AF closure pattern between patients with trigonocephaly and those with scaphocephaly reveals the different directions of suture fusion in the two conditions. Indeed, in most children with scaphocephaly, fusion begins on the posterior segment of the suture toward the AF. During diagnosis, due to the abnormal skull shape, the AF remains completely open. Otherwise, the metopic suture starts to close in the proximity of the AF, which greatly impacts early closure. This directionality of fusion was corroborated by Lottering et al.,26 who investigated the temporal closure of AF in 256 healthy children aged <30 months by using multislice cranial CT scans and observed the posteroanterior pattern of sagittal suture ossification and metopic closure near the AF and the coronal sutures synchronously.
Although AF assessment is initially performed using the examiner's index fingers,30 currently, CT scanning is considered the gold standard for measuring the AF size and confirming the closure.2 In addition, our study used high-resolution CT images to examine AF closure and diagnose CS after closure appearance in 65.5% of the patients but low sensitivity and specificity were obtained. In addition, this was the first study to show that AF fusion was not highly associated with CS diagnosis, with 38% sensitivity and 61% specificity. Nonetheless, if the authors considered patients aged <6 months, the sensitivity would increase to 61%, reinforcing the awareness of this phenomenon as a sign of skull ossification abnormality. Hence, pediatricians should consider the risk of CT radiation after judging an AF closure, pointing out mild head trauma.18 Conversely, pediatric neurosurgeons should evaluate patients before performing a CT scan to diagnose a potential CS.
To the best of our knowledge, a major risk is the misdiagnosis of the absence of CS based on the perception of a widely open AF. This false-negative interpretation might have occurred in 30% of our sample, and half of the patients who presented with an open AF had CS (Figure 2). Thus far, no information regarding this fact is available in the literature, and the authors surmise that the risk is crucial in cases with scaphocephaly. Therefore, pediatricians should be aware of this fact and focus on the existence of skull deformities that are characteristic of CS to reduce the possibility of a misdiagnosis.
Limitations and future directionsThis study has some limitations, such as the absence of data regarding the measurement sizes of the AFs and retrospective data. Moreover, evaluation by the senior author might have caused a bias. However, the main strength of this study was the valid comparison between healthy children and those with non-syndromic CS based on representative population data, thereby highlighting the considerable number of children with CS presenting with open AF. Furthermore, further studies comparing fontanel sizes could reveal the cutoff for AF closure in Brazilian children and clarify this relationship.
ConclusionIn spite of the overall low accuracy of closed AF in the diagnosis of CS, AF closure remains a concern, showing different patterns worldwide. To our knowledge, early suture fusion in CS is clearly associated with closed AF in some conditions, especially in trigonocephaly. Moreover, to avoid misdiagnosis, pediatricians should be aware of the risk of wide-open AF concomitantly in children with a true CS. Therefore, the best practical suggestion is primarily to gather information regarding skull deformity patterns and rule out classical non-syndromic CS before referring to a pediatric neurosurgeon for concern of closed AF, thereby avoiding unnecessary CT scan procedures.
Study conducted at the Vila da Serra Hospital, Nova Lima, MG, Brazil.





