

To assess the occurrence of an aggregate risk to cardiometabolic and musculoskeletal health of Brazilian adolescents in the period 2008/09 and 2013/14 and to identify whether there are differences in risk between the genders and in these periods.
MethodsThis was a trend epidemiological study with a quantitative approach, consisting of a voluntary sample of adolescents from 16 Brazilian states. Data were extracted from the database of Brazil Sports Project (Projeto Esporte Brasil). Health-related physical fitness was evaluated based on body mass index, cardiorespiratory fitness, flexibility, and abdominal strength/resistance. Descriptive analysis, chi-squared test, and Poisson log regression were used for the statistical treatment.
ResultsIn the years 2008/09, 14.6% of Brazilian youngsters showed an aggregate risk to cardiometabolic health and 17.1% an aggregate risk for musculoskeletal indicators, whereas in 2013/14, the values of the risk indicators were, respectively 40.0% and 22.4%. It was observed that, in the years 2013/14, the risk to the cardiometabolic health of boys was 2.51 times greater than in 2008/09, while for girls, a three-fold increase in risk was observed. Concerning musculoskeletal health, girls showed a 2.21 risk of being in the risk zone in 2013/14 when compared with 2008/09.
ConclusionThe occurrence of an aggregate risk to the cardiometabolic and musculoskeletal health of Brazilian adolescents increased in the 2008/09 and 2013/14 periods. Regarding gender, an increase in the cardiometabolic and musculoskeletal risk between these periods was observed in girls. As for boys, an increase was observed only in cardiometabolic risk.
Verificar a ocorrência de risco agregado à saúde cardiometabólica e musculoesquelética de adolescentes brasileiros no período de 2008/09 e 2013/14 e identificar se existem diferenças no risco entre os sexos e nesses períodos.
MétodosTrata-se de um estudo epidemiológico de tendência com abordagem quantitativa, composto por uma amostra voluntária de adolescentes, de 16 estados brasileiros. Os dados foram extraídos da base de dados do Projeto Esporte Brasil. A aptidão física relacionada a saúde foi avaliada a partir de: índice de massa corporal, aptidão cardiorrespiratória, flexibilidade, e força/resistência abdominal. Para o tratamento estatístico foi utilizado análise descritiva, qui-quadrado e regressão Poisson log.
ResultadosNos anos de 2008/09, 14,6% de jovens brasileiros apresentaram risco à saúde cardiometabólica agregada e 17,1% risco agregado dos indicadores musculoesqueléticos. Enquanto em 2013/14, os valores dos indicadores de risco foram, respectivamente 40,0% e 22,4%. Observou-se que nos anos de 2013/14 o risco à saúde cardiometabólica dos meninos era 2,51 vezes maior que em 2008/09. Já para as meninas o aumento desse risco foi de 3 vezes. No que se refere à saúde musculoesquelética, as meninas apresentaram risco de 2,21 de estar na zona de risco em 2013/14 em relação à 2008/09.
ConclusãoA ocorrência de risco agregado à saúde cardiometabólica e musculoesquelética de adolescentes brasileiros aumentou no período de 2008/09 e 2013/14. Com relação ao sexo houve um aumento no risco cardiometabólico e musculoesquelético nas meninas entre esses períodos. Já para os meninos houve aumento apenas do risco cardiometabólico.
Recent studies have demonstrated an association between health risk factors such as overweight/obesity and low levels of cardiorespiratory fitness (CRF), with the early risk of developing metabolic diseases.1 Low levels of musculoskeletal fitness, i.e., of flexibility and muscular strength/resistance criteria, have also been considered predictors of problems such as postural deviations and other musculoskeletal disorders.2 According to Thomas et al.,3 cardiorespiratory, musculoskeletal, neuropsychological, endocrine, and metabolic health depend directly on the level of physical fitness and, thus, fitness has become an important marker of health in children and adolescents.4
However, this population has shown low levels of health-related physical fitness (HRPF).5 In the United States and in Brazil, these inadequate levels have alarmingly increased in recent years, with occurrences ranging from 42% to 63%.6–8 The greatest impact of these data is disclosed when studies indicate that low levels of CRF combined with overweight and obesity indicators (such as body mass index [BMI]) have become predictors of early risk for cardiometabolic diseases, such as insulin resistance, type II diabetes, and myocardial infarction.1,2 Additionally, according to Ortega et al.,2 a low level of CRF, when considered alone, is already an indicator of health risk, since it is associated with high mortality rates.8 The same can be said about BMI, which is even more of a concern, considering that approximately 30% of Brazilian children and young individuals are overweight or obese.9
Regarding muscle strength and flexibility, Meisler et al.10 stated that these are physical capacities that prevent trauma and bone fracture risks. Furthermore, when these two indicators are aggregated at low levels, they may accelerate more severe musculoskeletal disorders, such as sarcopenia, lean mass loss, and bone mass loss.11 All these associated factors tend to limit body functions throughout life, also influencing the practice of physical activity.12
In fact, maintaining good levels of HRPF is important to provide adequate motor skills to carry out daily activities,13 which is associated with direct health markers.2 What is new in this regard is that when HRPF components are assessed together, they are likely to indicate a much higher risk condition than when assessed alone, as they determine different health risks. However, little is known about the prevalence of aggregate inadequate physical fitness levels in the young Brazilian population.
In this sense, it is important to study HRPF, considering all its components. In addition, HRPF assessment in schools is a very adequate method for this purpose, since it is easy to apply, effective, low-cost, and can be performed in a large number of subjects.14–16 Subsequently, interventions that consider HRPF broadly can be created. Moreover, physical education classes can be developed with the purpose of promoting health.17 Thus, the present study aimed to verify the occurrence of an aggregate risk to the cardiometabolic and musculoskeletal health of Brazilian adolescents in the period 2008/09 and 2013/14 and to identify whether there are differences in risk between the genders and in those periods.
MethodsThis was an trend epidemiological study with a quantitative approach, consisting of a voluntary sample of schoolchildren aged 12–17 years, from public and private schools of 16 Brazilian states, namely: Amazonas, Bahia, Ceará, Distrito Federal, Espirito Santo, Goiás, Minas Gerais, Mato Grosso, Piauí, Paraná, Rio de Janeiro, Rio Grande do Norte, Rio Grande do Sul, Santa Catarina, São Paulo, and Tocantins. The adolescents were evaluated regarding HRPF, by their Physical Education teachers in each voluntary education institution in 2008/2009 (n=4538) and 2013/2014 (n=3106). Teachers, students, parents, and the educational institutions agreed to carry out the study by signing the authorization and informed consent forms, confidentiality of the students’ identities, and the sending of data and authorization documents to a national database, where they could obtain results and reports with feedback on the health of the schoolchildren from an interactive website. The inclusion criteria in the analyses of the present study were: (1) all students who volunteered to participate; (2) those who had all the authorization documentation previously described; and (3) who had undergone all HRPF tests.
As reference for conducting the tests, the teachers used the manual of tests and measures of physical fitness in the health components: measures of body mass and height: calculation of BMI; nine-minute run/walk test: cardiorespiratory fitness; flexibility: sit and reach test without a bench; and abdominal resistance-strength: sit-ups in one minute. This method was created by Brazil Sports Project (Projeto Esporte Brasil [PROESP-Br]).15 The instructions for applying these tests are available at: www.proesp.ufrgs.br. It should be noted that these tools were developed considering the reality of Brazilian schools, offering low-cost, applicable resources, while following valid, reproducible, and reliable scientific quality standards to estimate some health parameters in children and adolescents.18
Therefore, body mass was measured using a digital anthropometric scale, graduated from 0 to 150kg, with a resolution of 0.05kg and recorded in kilograms, using one digit after the decimal point. The adolescents were evaluated preferentially while wearing physical education clothes and barefoot, standing with their elbows extended close to the body. Height was measured using a metric tape fixed to the wall and extended from the bottom upwards, with the students in the upright position, with feet and trunk touching the wall. This measure was recorded in centimeters with one digit after the decimal point. The described procedures followed the PROESP-Br standard. Subsequently, the BMI was calculated by dividing body mass (in kilograms) by height (in square meters). The cutoff point of PROESP-Br was used, considering gender and age.15
For the nine-minute run/walk test, the adolescents were divided into groups that were adequate for the running track dimensions. They were instructed to run as long as possible, avoiding velocity peaks interspersed by long walks for nine minutes. During the test, the passage of time was informed to the students at two, four, and six minutes. (“Warning: 1minute to finish”). Additionally, participants were verbally encouraged. At the end of the test, after a signal was given, the students interrupted the running, remaining in place where they were standing until the distance traveled was recorded or signaled.
The sit and reach test was performed with a measuring tape fixed to the ground. At the 38-cm mark on the tape, a piece of 30-cm adhesive tape was fixated perpendicularly. Adolescents were barefoot, with extended knees and overlapping hands; the assessed individual slowly bowed and stretched out the hands as far as possible in two attempts, of which the higher one was recorded.
The one-minute sit-up test was performed with the assessed individual in the supine position with knees flexed at 45 degrees, arms crossed over the thorax, and ankles fixated to the floor by the evaluator. At the evaluator's sign, the student flexed the trunk until he/she touched the thighs with the elbow, returning to the starting position, as many times as possible in one minute.
In accordance with the PROESP-Br manual, which considers gender and age, data from the HRPF variables were categorized in the risk zone or in the healthy zone, following an adequate statistical assumption (www.proesp.ufrgs.br).15
Furthermore, the present study was approved by the Ethics Committee of Universidade Federal do Rio Grande do Sul, under number 2008010.
In the statistical analysis, the characteristics of the sample were first described in the two assessed periods (2008/09 and 2013/14), reporting the absolute and percentage values of the occurrence of gender, age, region of Brazil, and the risk zone of the HRPF variables. Considering the objectives of the present investigation, the risk variables of the HRPF were grouped into cardiometabolic risk (BMI+CRF) and musculoskeletal risk (flexibility+abdominal strength/resistance). Thus, only the frequency of individuals with aggregate risk and those in the healthy zone was considered. It should be noted that students who only had one risk of the HRPF variables were not included in the subsequent analyses, which refer to the statistical tests. To describe the aggregation of cardiometabolic and musculoskeletal risk, absolute and percentage values were used in the years 2008/09 and 2013/14, as illustrated in a bar chart.
After this description, the chi-squared test was performed to measure the prevalence ratio (PR) of the aggregate risk on the frequency of healthy individuals in the different genders, in each evaluated year period (2008/09 and 2013/14). The association between age and aggregate risk was also verified using Spearman's correlation test. Finally, considering the results of these primary analyses, a Poisson log regression was performed, stratified by gender, where the aggregate risk PR was verified for healthy individuals between 2008/09 and 2013/14. These analyses were performed using the SPSS (IBM SPSS Statistics for Windows, Version 22.0, NY, USA), considering a level of significance for an alpha <0.05.
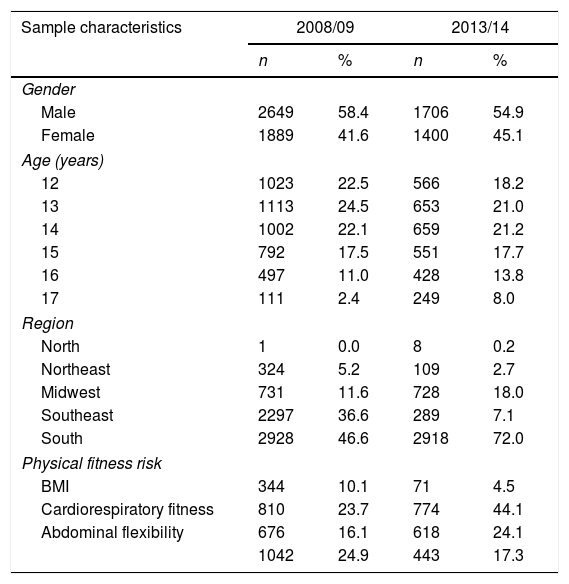
ResultsTable 1 shows the characteristics of the sample in 2008/09 and 2013/14. A total of 4538 adolescents were evaluated in the years 2008/09 and 3106 in the years of 2013/14, in the age group of 12–17 years.
Sample characteristics in the 2008/09 and 2013/14 periods.
| Sample characteristics | 2008/09 | 2013/14 | ||
|---|---|---|---|---|
| n | % | n | % | |
| Gender | ||||
| Male | 2649 | 58.4 | 1706 | 54.9 |
| Female | 1889 | 41.6 | 1400 | 45.1 |
| Age (years) | ||||
| 12 | 1023 | 22.5 | 566 | 18.2 |
| 13 | 1113 | 24.5 | 653 | 21.0 |
| 14 | 1002 | 22.1 | 659 | 21.2 |
| 15 | 792 | 17.5 | 551 | 17.7 |
| 16 | 497 | 11.0 | 428 | 13.8 |
| 17 | 111 | 2.4 | 249 | 8.0 |
| Region | ||||
| North | 1 | 0.0 | 8 | 0.2 |
| Northeast | 324 | 5.2 | 109 | 2.7 |
| Midwest | 731 | 11.6 | 728 | 18.0 |
| Southeast | 2297 | 36.6 | 289 | 7.1 |
| South | 2928 | 46.6 | 2918 | 72.0 |
| Physical fitness risk | ||||
| BMI | 344 | 10.1 | 71 | 4.5 |
| Cardiorespiratory fitness | 810 | 23.7 | 774 | 44.1 |
| Abdominal flexibility | 676 | 16.1 | 618 | 24.1 |
| 1042 | 24.9 | 443 | 17.3 | |
n, absolute value; %, percentage; BMI, body mass index.
The occurrences of aggregate risks added to cardiometabolic and musculoskeletal health are shown in Fig. 1. It can be observed that there was an increase in cardiometabolic and musculoskeletal risk between the years. In 2008/09, cardiometabolic risk (total n: 2260; n at aggregate risk: 332) was proportionally lower than in 2013/14 (total n: 901; n at risk: 370). Regarding musculoskeletal risk, there was an increase in the proportion between the years 2008/09 (total n: 2472; n at risk: 437) and 2013/14 (total n: 1499; n at risk: 360).

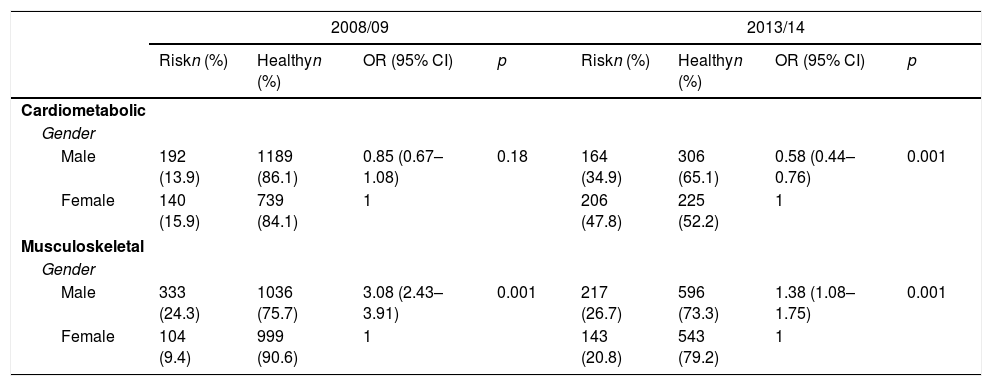
Table 2 shows the association of gender and age with the aggregation of cardiometabolic and musculoskeletal risk in the different evaluation periods. Regarding gender, it was observed that there is a difference between being in the risk in the assessed periods. It was also observed that the strength of the correlations between age and aggregate risk, both cardiometabolic and musculoskeletal, are very weak, although some associations have a significance level within the expected.
Aggregation of cardiometabolic and musculoskeletal risk in relation to gender and age of adolescents in the years 2008/09 and 2013/14.
| 2008/09 | 2013/14 | |||||||
|---|---|---|---|---|---|---|---|---|
| Riskn (%) | Healthyn (%) | OR (95% CI) | p | Riskn (%) | Healthyn (%) | OR (95% CI) | p | |
| Cardiometabolic | ||||||||
| Gender | ||||||||
| Male | 192 (13.9) | 1189 (86.1) | 0.85 (0.67–1.08) | 0.18 | 164 (34.9) | 306 (65.1) | 0.58 (0.44–0.76) | 0.001 |
| Female | 140 (15.9) | 739 (84.1) | 1 | 206 (47.8) | 225 (52.2) | 1 | ||
| Musculoskeletal | ||||||||
| Gender | ||||||||
| Male | 333 (24.3) | 1036 (75.7) | 3.08 (2.43–3.91) | 0.001 | 217 (26.7) | 596 (73.3) | 1.38 (1.08–1.75) | 0.001 |
| Female | 104 (9.4) | 999 (90.6) | 1 | 143 (20.8) | 543 (79.2) | 1 | ||
| n | r | p | n | r | p | |
|---|---|---|---|---|---|---|
| Cardiometabolic | ||||||
| Age | 2260 | 0.05 | 0.006 | 901 | −0.05 | 0.06 |
| Musculoskeletal | ||||||
| Age | 2472 | 0.03 | 0.06 | 1499 | 0.04 | 0.86 |
n, absolute value; %, relative value; r, Spearman's correlation coefficient; 95% CI, 95% confidence interval (chi-squared test); OR, odds ratio.
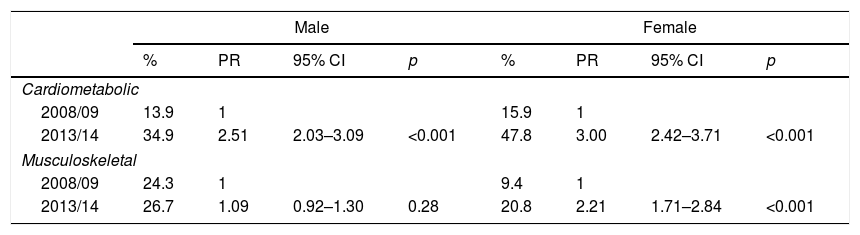
The comparisons between the aggregate risks to cardiometabolic and musculoskeletal health of the adolescents assessed in the years 2008/09 and 2013/14, stratified by gender, are shown in Table 3. In males, cardiometabolic risk increased by 2.5-fold in 2013/14 when compared with 2008/09. In females, an increase in risk of approximately three-fold was observed. Musculoskeletal risk increased by approximately 2.2-fold (CI: 1.71–2.84) in 2013/14, when compared with the 2008/09 period in females; no significant increase was observed in males.
Prevalence ratio of aggregate risks to cardiometabolic and musculoskeletal health between the years 2008/09 and 2013/14, stratified by gender.
| Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|
| % | PR | 95% CI | p | % | PR | 95% CI | p | |
| Cardiometabolic | ||||||||
| 2008/09 | 13.9 | 1 | 15.9 | 1 | ||||
| 2013/14 | 34.9 | 2.51 | 2.03–3.09 | <0.001 | 47.8 | 3.00 | 2.42–3.71 | <0.001 |
| Musculoskeletal | ||||||||
| 2008/09 | 24.3 | 1 | 9.4 | 1 | ||||
| 2013/14 | 26.7 | 1.09 | 0.92–1.30 | 0.28 | 20.8 | 2.21 | 1.71–2.84 | <0.001 |
%, relative value; PR, prevalence ratio; 95% CI, 95% confidence interval (chi-squared test).
The main results of the present study indicated that in the years 2008/09, 14.6% of Brazilian youngsters had an aggregate cardiometabolic health risk and 17.1% had an aggregate risk of musculoskeletal indicators, while in 2013/14, the risk indicator values were, respectively, 40.0% and 22.4%. It was observed that in 2013/14, the cardiometabolic health risk of the boys was 2.51-fold greater than in 2008/09. For girls, the increase in risk was three-fold. Concerning musculoskeletal health, girls showed a PR of 2.21 of being in the risk zone in 2013/14 when compared with 2008/09.
The cardiometabolic and musculoskeletal health risk increased considerably between the evaluation periods. To the best of the authors’ knowledge, this is the first study to investigate the occurrence of cardiometabolic and musculoskeletal risk aggregates for BMI+CRF and flexibility+abdominal strength/resistance. It is known that when the variables are considered alone, the prevalence of obesity and cardiorespiratory impairment shows a trend of concern. In that sense, a study published in the United States indicated that the percentage of obese adolescents in the period 1988–1994 was 10.5%, increasing to 20.6% in 2013–2014.19 Regarding CRF, the findings point in the same direction, indicating a decrease between 1992 and 1999 and between 1992 and 2012 in African children and adolescents. The same occurs when considering the variables of muscular strength/resistance and flexibility: children and youngsters were more flexible, agile, and fast in 1992 than in 2012.20
The increase in the aggregate risk of HRPF indicators may have occurred due to several behavioral factors, such as decrease in physical activity levels, increase in sedentary behavior and consumption of unhealthy foods, and decrease in active displacement, in addition to the high occurrence of overweight and obesity in Brazilian youngsters.9,21 It is noteworthy that cardiometabolic risk increased at an alarming rate between the periods, which may be due to the fact that Brazilian adolescents have been showing lower levels of CRF. One of the consequences of low CRF and its decline over time is the association with an increase in cardiometabolic diseases such as type II diabetes, hypertension, and dyslipidemia.22 Considering these aspects, which makes the findings of the present study even more of a matter of concern is that the presence of two simultaneous risk indicators increases the likelihood that the individual will have some type of health problem in the future.
Regarding cardiometabolic health between the genders, there was an increase in risk for both boys and girls when comparing the two periods. It is noteworthy that the risk was higher for girls. These findings can be explained by the fact that girls have a less active lifestyle, as well as cultural factors that lead them to practice less sport and physical activities.23–25 Additionally, girls tend to have greater gains in fat mass, which may also be related to the hormonal changes of puberty.26 In boys, however, these hormonal factors are associated with increased lean mass from the end of childhood to early adolescence.27
Regarding musculoskeletal health, girls showed a PR of 2.21 of being in the risk zone in 2013/14 when compared with 2008/09, i.e., 9.4% were in the risk zone in the first considered period, increasing to 20.8%. In boys, however, no difference was found between the periods, but this may have occurred because 24.3% of the boys were already in the risk zone in 2008/09, increasing to 26.7% in 2013/14. Therefore, in the two analyzed periods, the percentage of boys in the risk zone for musculoskeletal health was high, and higher than the values found in girls.
Considering the musculoskeletal health indicators alone, a study on Spanish adolescents showed a decrease in muscular strength of boys and girls between the periods 2001–2002 and 2006–2007.28 As for Mozambican adolescents, the results indicated a decrease in muscle strength in girls between 1992 and 2012, and an increase was observed in boys.20 In fact, according to the literature, boys show lower risks in the variable muscle strength because hormonal factors naturally increase this variable.29 Similarly, regarding flexibility, a decline in performance was observed over time.20,30
Considering the aforementioned aspects, it is important to know the reality regarding the HRPF of Brazilian adolescents, so that, based on this, intervention programs that promote health can be created, taking into account that one of the places to develop these actions is the school environment, through the physical education teacher, by encouraging the practice of physical activity, active behavior, and decrease of sedentary lifestyle.
Therefore, it should be noted that this study makes a great contribution to the HRPF area, since all its indicators were investigated. It is also emphasized that the aggregated manner as the data were considered allowed an analysis perspective that was different from the studies in this area. Additionally, adolescents from all regions of Brazil were assessed, although the sample was small in the North. Nevertheless, these data allow an overview of HRPF in Brazil.
Nevertheless, some limitations must be considered. The sample was selected by convenience and had a different number of subjects in the two analysis periods. Additionally, the same subjects were not assessed in both periods of analysis. Due to the availability of data in the PROESP-Br database, a heterogeneity in the number of adolescents in each region was observed. It should be noted that sexual maturation was not assessed.
Therefore, the presence of an aggregate risk to the cardiometabolic and musculoskeletal health of Brazilian adolescents increased from 2008/09 to 2013/14. Regarding gender was an increase in the PR of cardiometabolic and musculoskeletal risk in girls was observed between these periods. For boys, there was an increase only in cardiometabolic risk. Considering these data, it can be concluded that the HRPF of adolescents has worsened over the years. These data point to a scenario of concern, since low levels of CRF, abdominal strength/resistance, and flexibility, as well as high levels of BMI are associated with several health problems.
FundingNational Council for Scientific and Technological Development (CNPq) and Coordination for the Improvement of Higher Level-or Education- Personnel (CAPES).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Gaya AR, Dias AF, Lemes VB, Gonçalves JC, Marques PA, Guedes G, et al. Aggregation of risk indicators to cardiometabolic and musculoskeletal health in Brazilian adolescents in the periods 2008/09 and 2013/14. J Pediatr (Rio J). 2018;94:177–183.
Study carried out at Universidade Federal do Rio Grande do Sul (UFRGS), Escola Superior de Educação Física, Fisioterapia e Dança (ESEFID), Research Group: Brazil Sports Project (PROESP-Br), Porto Alegre, RS, Brazil.




