

The present study aims to present and discuss the role of neuropsychological assessment (NA) in the investigation of neurodevelopmental disorders (NDDs), with an emphasis on early diagnosis, on the steps that make up the evaluation process, and on the resources that complement clinical evaluation. Furthermore, the discussion is expanded to specific conditions, such as Attention Deficit/Hyperactivity Disorder (ADHD), Autism Spectrum Disorder (ASD), and Specific Learning Disorders (SLD), considering that they represent frequent assessment demands.
Data sourcesA critical review of the national and international literature on neuropsychological assessment in NDDs was carried out, highlighting standardized instruments for the Brazilian context, complementary clinical tasks, and main cognitive and behavioral domains. References to essential books and manuals were included, with analysis enriched by the authors' clinical and teaching experience.
Data synthesisNA constitutes a central tool for the early identification of alterations in neurodevelopment, with contributions to diagnosis and to the definition of intervention strategies. The process involves systematic steps, such as detailed anamnesis, application of standardized tests, and behavior analysis, covering different domains. The feedback, the final stage of the process, is essential for the understanding of the results and for adhering to the suggested procedures, and it should guide parents on practical implications, therapeutic and educational recommendations, and necessary referrals.
ConclusionsNA represents an essential resource in pediatric practice, both for diagnostic support and for directing interventions and monitoring the progress of children with NDDs. Its early use can modify the prognosis and promote better functional, academic, and socioemotional outcomes.
Neurodevelopment refers to the continuous process of anatomical and functional maturation of the nervous system (NS), which begins in utero and continues more intensely throughout the first years of life. This process involves fundamental stages, such as neuronal proliferation and migration, the formation of synaptic connections, myelination, and synaptic pruning, which enable the progressive acquisition of motor, cognitive, emotional, and social skills [1]. Neuropsychological development, on the other hand, results from the dynamic interaction between an individual's genetic heritage, other biological factors, and environmental stimuli, such as family, social, affective, and cultural factors. Thus, early experiences, both positive and adverse, can have a significant impact on brain organization and cognitive and behavioral functioning throughout life.
As a clinical and scientific resource, neuropsychological assessment (NA) is highly relevant for understanding the functioning of individuals suspected of having neurodevelopmental disorders (NDDs), providing essential information for identifying areas of strength and vulnerability, as well as possible comorbidities. Its main objective is to recognize patterns of functioning (cognitive-adaptive profile) that aid in diagnosis and estimate functional impact, enabling intervention planning and longitudinal monitoring, going beyond the mere description of symptoms and allowing a broader understanding of the patient's profile [2].
The assessment of NDDs should, whenever possible, be conducted by a multidisciplinary team, considering the complexity and variability of clinical manifestations. The integration of different areas, encompassing cognitive, emotional, behavioral, motor, and social aspects, favors not only a more accurate diagnosis but also the development of individualized and effective care/therapeutic strategies aligned with the specific needs of each case.
It is estimated that approximately 250 million children worldwide have some type of neurodevelopmental delay or disability [3]. International data indicate an increasing trend in the prevalence of neurodevelopmental and behavioral disorders within the broader context of disabilities. Among the most prevalent disorders, the following stand out:
- •
Autism Spectrum Disorder (ASD), with a recent estimate from the Centers for Disease Control and Prevention (CDC) indicating that one in 31 children up to age 8 has been diagnosed with the disorder; [4]
- •
Attention Deficit Hyperactivity Disorder (ADHD), whose global prevalence is estimated at between 5 % and 8 %, according to the Brazilian Attention Deficit Association (ABDA); [5]
- •
Specific Learning Disorders (SLD), which affect between 5 % and 15 % of the global population, according to the American Psychiatric Association [6].
According to the World Health Organization [7]. such estimates may be underestimated, considering the difficulties in early diagnosis, the high mortality rates in vulnerable populations, and the stigma associated with these conditions. These are, therefore, highly prevalent conditions whose impact on academic and psychosocial development poses significant challenges throughout the various stages of life. Early diagnosis, combined with appropriate interventions, is essential, as it has a decisive impact on the prognosis and quality of life of children and their families.
Neurodevelopmental disordersNDDs constitute a group of clinical conditions that begin during the developmental period, usually in early childhood, and are characterized by deficits in cognitive, behavioral, social, and emotional functioning [6]. These disorders result from alterations in brain development and manifest early, with significant repercussions on the individual's academic, social, and occupational life.
Unlike other mental and behavioral disorders, such as schizophrenia or bipolar disorder, in neurodevelopmental disorders, cognitive and behavioral changes are central manifestations, not secondary or associated conditions [8].
It is important to note that an individual may present comorbidity between NDDs, suggesting the influence of shared genetic and environmental factors. Regarding the etiology, it is known to be complex and multifaceted and, in many cases, unknown.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR), in its most recent version in Brazil, includes the following NDDs:
- •
Intellectual Development Disorders
- •
Communication Disorders
- •
Autism Spectrum Disorder
- •
Attention Deficit/Hyperactivity Disorder
- •
Specific Learning Disorder
- •
Motor Disorders
NA is a structured clinical procedure that aims to understand the individual's cognitive, emotional, and behavioral functioning, using standardized tests, neuropsychological tasks, complementary instruments, as well as clinical observations and interviews. There is no fixed battery that is applicable to all cases, since the choice of instruments should be guided by the specific demands of the assessment, the diagnostic hypotheses, and the objectives of the process. Nevertheless, the investigation of certain domains is recommended, such as intellectual functioning, attention and executive functions, memory, language, visuospatial and constructive skills, reading, writing, and math skills, as well as emotional and behavioral aspects (complementary to the cognitive profile) and adaptive functioning (AF). In pediatric practice, NA is used for different purposes:
- •
Mapping the cognitive-adaptive profile, aiding in diagnosis
It consists of describing the neuropsychological profile, identifying the presence or absence of cognitive dysfunctions, and the level of impact on the individual's life [9]. This information aids in diagnosis, as it provides complementary evidence to clinical and contextual data, in addition to guiding appropriate interventions. It would be like constructing a detailed portrait of how the child/adolescent learns, thinks, and adapts to daily life at that moment, allowing the identification of both strengths and vulnerabilities, which guides diagnosis and interventions.
To achieve this goal, various methods and techniques are employed, including interviews, behavioral observations, clinical scales, and the administration of standardized instruments and other neuropsychological tasks to investigate different domains, in addition to qualitative performance analysis [10]. In the case of individuals with NDDs, the diversity of clinical manifestations can make both the selection of the test battery and the interpretation of results an additional challenge [2]. The professional's expertise is essential to define the limits and applicability of each assessment method.
- •
Identify the presence of comorbidities and clarify the differential diagnosis (e.g., distinguish primary manifestations of ADHD from anxiety/sleep effects, etc.)
Neuropsychological assessment, by integrating data from interviews, observation, and the use of standardized instruments, allows us to distinguish primary manifestations of the disorder from those related to comorbidities, contributing to a more accurate diagnosis. Symptoms such as attention difficulties, school problems, or behavioral changes can often be present in different conditions, such as ADHD, SLD, ASD, or anxiety disorders.
- •
Estimating functional impact and support needs
NA is not limited to identifying cognitive deficits; it allows estimating the functional impact of changes observed in the daily life of children with NDD and identifying the most appropriate support needs. Through the integrated analysis of cognitive, emotional, and behavioral skills, combined with qualitative observation and family reports/other sources of information, it is possible to outline needs that will be the focus of intervention and/or educational and social adjustments, promoting the child's functionality and participation in different contexts.
Adaptive functioning (AF) refers to the individual's ability to apply their cognitive skills to daily life, encompassing practical, social, and conceptual aspects. Assessing these domains reveals how the individual copes with the demands of daily life. Domains assessed (according to DSM-5-TR and AAIDD [11]):
- (a)
Conceptual: communication, language, academic skills, reasoning, and memory.
- (b)
Social: interpersonal relationships, empathy, social skills, group participation.
- (c)
Practical: autonomy, self-care, use of community resources, routine organization, safety.
- •
Support the planning of interventions and the longitudinal monitoring, as well as guide the family and school
The results of the assessment have direct implications for clinical and educational management. The information obtained guides individualized intervention programs, pedagogical strategies, and the training of parents and teachers to address the specific demands of each child. The assessment also serves as a baseline for monitoring the evolution of the condition over time and evaluating the effectiveness of the implemented interventions.
Stages of the assessment processTo assist in understanding this systematic and rigorous process, eight steps are highlighted, suggested by other authors [1] and here adapted to the Brazilian context, which must be integrated to record the information provided and appropriately interpret and communicate the results: [1]
- (1)
Attentive listening to the reason for seeking consultation: This initial phase focuses on understanding the reported concerns and needs, considering the factors involved, the affected individuals, and the manifestations of the condition in the patient and their environment. It is an opportunity for parents/caregivers and children to feel heard and understood, creating a comfortable environment for the following steps. According to the Code of Professional Ethics for Psychologists ( Art. 8) [12] and Federal Council of Psychology (Resolution No. 13/2022) [13], which consolidates standards and principles for the provision of psychological services to children and adolescents, conducting a neuropsychological assessment in children requires formal authorization from at least one legal guardian.
- (2)
Knowledge of the child's clinical and academic history, behavior and family background: Includes personal data (name, date of birth, chronological age, school year, school, with whom the child lives), clinical history (neuropsychomotor development, chronic conditions, medical treatments and pharmacological and non-pharmacological interventions), academic history (age of entry into school, performance, learning problems, failures, adaptation, changes of school), behavior (relevant traits, sociability, anxiety, mood, motivation, sleep disorders) and family history (home environment, age and level of education of parents and siblings, family history of NDDs). It is crucial to delve deeper into the child's AF at this stage [1].
- (3)
Analysis of complementary examinations and of additional health and educational records: This stage involves reviewing previous neuropsychological evaluations, reports from teachers and/or other professionals working with the child, and relevant medical examinations [1]. It also considers the presence of curricular adaptations, specialized educational service plans, tutoring interventions, or other relevant educational support strategies.
- (4)
Permanent clinical observation: This includes the child's initial contact (visual, posture, communication), participation and engagement during the interview and testing/task completion, motivation, energy level, state of consciousness, attention, comprehension, and mood. It considers possible interferences such as changes in vigilance, attention, and energy due to lack of sleep and/or medication use, allowing for the optimal timing of the evaluation.
- (5)
Application of neuropsychological tests and neuropsychiatric scales: These are highly relevant assessment tools. Tests/tasks and scales appropriate for the specific clinical case should be selected, with known psychometric properties. Standardizing these tests ensures the validity and reliability of the data.
- (6)
Emotional aspects assessment: Although not essentially part of neuropsychological studies, it is recommended to include it, as emotional changes are a frequent comorbidity in NDDs and can interfere with cognitive processes [1]. Understanding socioemotional factors helps identify the origin of a certain behavior and inform the planning of more effective interventions. Neuropsychological repercussions in children can impact the school, family, and social environments, leading to interaction difficulties and influencing self-image. For assessment, the use of instruments such as depression and anxiety questionnaires, self-concept scales, and measures of socioemotional skills, among others, is recommended.
- (7)
Analysis of the child's results: The child's performance, expressed in standardized scores for their chronological age or school year, is analyzed considering the reason for the consultation, clinical observations, diagnostic hypothesis, possible comorbidities, and the context in which the child develops. Qualitative analysis in NA is also important, as it complements the results of objective tests and helps to better understand the performance of the person being evaluated. Finally, a report is prepared that integrates all this information, providing a comprehensive view of the child's condition and the suggested actions based on the findings.
- (8)
Delivery of results to interested parties (feedback): This includes legal guardians and the child themselves (considering their age, maturity, and level of understanding). Feedback can also be provided to members of the school system and to the health and education professionals involved, with written consent from the legal guardians. Even with authorization, the psychologist must ensure that the information shared is relevant, ethical, and to the extent necessary, preserving confidentiality and avoids undue exposure of the child.
Emphasis is placed on the analysis of the neuropsychological profile, its “translation” into school, home, and social life, and recommendations for necessary interventions and support. The feedback interview is a fundamental step in the neuropsychological assessment, as it allows clear communication of findings, guides interventions, and supports families, ensuring engagement in the suggested behaviors and ethical monitoring of the child.
It is important to note that the neuropsychological profile is dynamic and can vary over time due to the maturation process and therapeutic and pedagogical efforts. Furthermore, most traditional tests are standardized on typically developing populations and may not consider crucial factors in patients with NDDs, such as fatigue, boredom, low self-esteem, difficulties with motor control, understanding instructions, and stress. Therefore, clinical judgment and the development of new tools are essential for a more accurate assessment.
Cognitive and behavioral assessment tools in NDDsAmong the main domains investigated are: intelligence, attention and executive functions, memory, oral language, reading and writing, visuospatial and visuoconstructive functions, as well as socioemotional skills, other behavioral aspects, and AF. As previously mentioned, there is no single battery capable of assessing all NDDs; the choice of instruments depends on the specific objective of the investigation, the individual's overall level of functioning, and medication use, among other factors. The examiner's expertise is crucial, as they have the autonomy to select the most appropriate instruments to answer the clinical questions presented.
The combined analysis of these elements allows the construction of a profile of strengths and weaknesses, essential for understanding each individual's uniqueness [14].
Table 1 [15–55] presents the main instruments currently used in neuropsychological practice in Brazil, indicating the investigated domains. It is noteworthy that, although each neuropsychological instrument preferentially assesses a specific construct, they involve different skills. Therefore, the examiner's experience is a key differentiator in integrating the obtained data, based on clinical reasoning, to guide the best course of action at the end of the investigative process [56]. It should also be noted that neuropsychological assessment is a complex process that goes beyond the mere application of tests and tasks/other scales, and always involves a series of steps, in addition to the integration of knowledge necessary for the clinical context (neuroanatomy, psychopathology, child development, influences of the socioeconomic context, psychometrics, among others).
Neuropsychological Tests and Tasks and Instruments for Behavioral Assessment in NDDs.
* Some instruments are specific to certain neurodevelopmental disorders, while others have cross-sectional application and can be used in different conditions to assess cognitive, behavioral, or socioemotional domains.
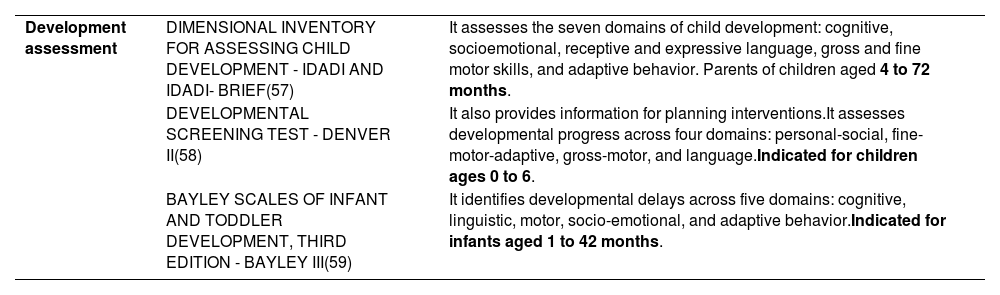
For infants and young children, specific developmental assessment scales are generally used, as detailed in Table 2, [57–59] allowing the early identification of skills and possible delays in different domains of neuropsychomotor, cognitive, and socioemotional growth.
Scales for assessing child development.
In clinical practice, neuropsychological assessment has wide application in different NDDs. Generally speaking, in cases of ADHD, it can be said that it helps characterize the predominant type of symptoms and their functional impact. SLD allows us to identify which reading, writing, or math skills are most compromised, guiding targeted pedagogical interventions. In ASD, it helps to map preserved cognitive skills and associated deficits, aiding in the definition of teaching and support strategies. Thus, the discussion focused on specific conditions, presented later, considering that they represent frequent assessment demands.
Neuropsychological assessment in ADHD: points of attention for clinical practiceThe diagnosis of ADHD is essentially clinical, based on DSM-5-TR and/or ICD-11 criteria and information obtained from multiple sources. Although the NA is not mandatory, international guidelines, such as those of the American Academy of Pediatrics (AAP), recommend its use in specific situations, such as in cases of diagnostic uncertainty, the presence of comorbidities, or the need for detailed characterization of the cognitive and functional profile [60].
Thus, the NA plays a relevant role in ADHD, contributing to the understanding of the different manifestations of the disorder, characterizing severity and prognosis, and identifying comorbidities, as mentioned above. Structured or semi-structured interviews, symptom screening scales, and other instruments that aid in the identification of psychiatric symptoms can be used for this purpose, in addition to instruments for cognitive and behavioral assessment (such as those described in Table 1), clinical observations, and informant reports. The exam is also useful in defining cognitive therapeutic targets, which can be addressed through both pharmacological and non-pharmacological interventions [61].
It is important to emphasize that there is no universal assessment protocol for ADHD: it should be planned based on the patient's history, considering age, potential comorbidities, medication use and their effects, as well as an estimate of overall cognitive level (61). Therefore, the neuropsychologist must be familiar with theoretical models of cognitive functioning, remembering that assessment goes far beyond the administration of tests and tasks. The analysis of results should always consider environmental, contextual, and cultural factors.
Although there is heterogeneity, some patterns are frequently observed in children with ADHD:
- •
Attention: impaired sustained and selective attention, with increased vulnerability to distraction.
- •
Executive functions: difficulties with response inhibition, planning, decision-making, cognitive flexibility, and performance monitoring.
- •
Working memory: deficits in retaining and manipulating information, affecting reasoning and learning.
- •
Processing speed: slowing down in tasks that require speed and precision (often as a means of achieving greater accuracy in performance).
- •
Inhibitory control: difficulties in inhibiting automatic/impulsive responses.
- •
Emotional regulation: difficulties in modulating emotions, often related to low frustration tolerance.
- •
Cognitive and Behavioral Self-Regulation: Persistence, mental effort, monitoring performance and time.
It is important to emphasize, however, that caution is needed when interpreting the results, as a significant portion of patients with ADHD may perform within normal limits on traditional neuropsychological tests [61]. The opposite is also true; excessive agitation may be associated with, for example, psychomotor overexcitability in high ability /giftedness (HA/G), anxiety, and other disorders, and is not “synonymous” with ADHD with a predominantly hyperactive/impulsive presentation.
Neuropsychological assessment in ASD: points of attention for clinical practiceDue to the complexity and heterogeneity of the neuropsychological profile of ASD, the term "spectrum" reflects the wide variability of cognitive, behavioral, and adaptive manifestations among individuals. Each person may show distinct combinations of abilities and challenges, which require a comprehensive and individualized assessment, covering domains such as attention, memory, executive functions, language, visuospatial and socioemotional skills, sensory processing, and emotional regulation. In this context, the use of standardized and targeted scales (suggested in Table 1) can optimize assessment time and provide objective data on characteristics essential for diagnosis, enabling the identification of behavioral and cognitive patterns typical of ASD, but always in conjunction with clinical practice (instruments are part of the process, but clinical judgment always prevails). Integrating data from family members, teachers, and others (multiple sources/different contexts) and clinical observations allows not only the identification of deficits but also the recognition of specific strengths and talents, providing support for the planning of personalized interventions aimed at maximizing functional potential and promoting quality of life.
At the end of the assessment, suggested actions should include referrals to appropriate services and interventions (and therapeutic options), as well as guidance to the family on the diagnosis, legal rights, and educational and social resources, aiming to support the individual's development, inclusion, and quality of life.
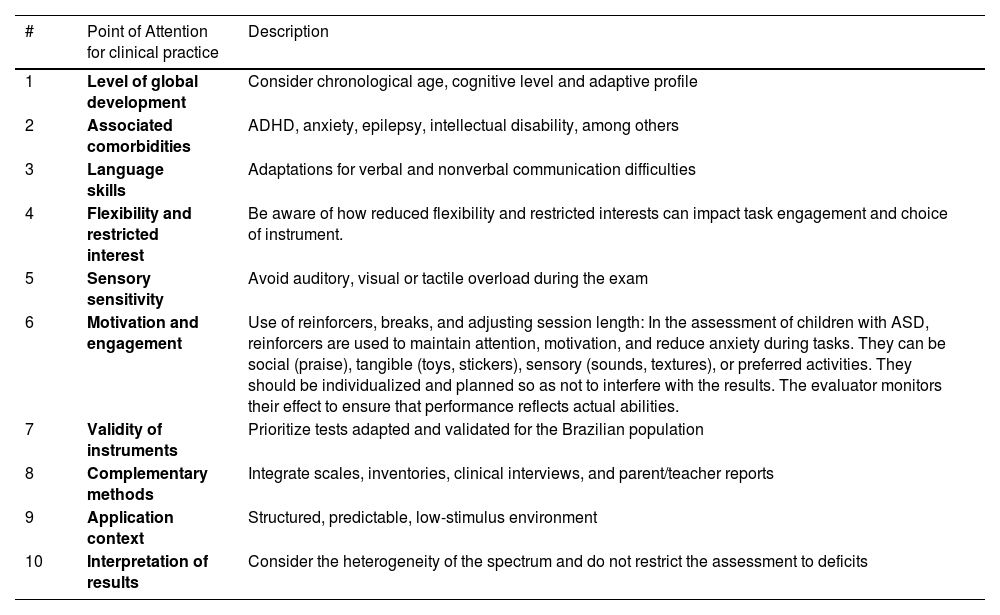
In the ASD NA, the authors emphasize 10 points that deserve special attention to ensure the assessment is clinical, ethical, and effective (illustrated in Table 3).
10 points of attention for neuropsychological assessment in ASD.
SLDs, which include dyslexia, dyscalculia, and dysgraphia, are characterized by significant and persistent impairments in specific academic skills that cannot be explained by sensory or intellectual deficits, or lack of schooling. The literature shows that these disorders are often associated with deficits in core neuropsychological functions, such as phonological awareness, working memory, sustained and selective attention, processing speed, receptive and expressive language, in addition to executive functions such as inhibition and cognitive flexibility. Another clinical indicator is avoidance of activities that require academic skills.
Children with dyslexia may demonstrate significant impairments in verbal working memory and phonological processing, while those with dyscalculia have more marked impairments in visuospatial working memory and the mental representation of quantity [62]. Transdiagnostic studies point to three essential cognitive pillars—phonological processing, processing speed, and executive functions—that significantly explain academic difficulties in reading and mathematics, regardless of the presence of ADHD [63].
Neuropsychological assessment plays an essential role in identifying and characterizing these impairments, using instruments that accurately assess the relevant cognitive domains. In addition to quantitative analysis of scores, the assessment also relies on qualitative data, such as compensatory strategies, error type, and performance pattern, which are essential for the differential diagnosis between disorders and secondary school difficulties. Studies show that children with SLD perform worse on memory tasks, executive functions, and perceptual-motor skills when compared to peers with typical development, reinforcing the importance of a comprehensive assessment that is sensitive to the child's neurocognitive profile [64].
The interpretation should also consider contextual factors, schooling/access to stimulation, and socioemotional aspects. Collaboration with speech-language pathologists, educational psychologists, and teachers is essential for an effective, evidence-based treatment plan.
ConclusionNA plays a central role in the investigation of NDDs, allowing not only a better diagnostic definition but also providing concrete support for individualized interventions and the building of support networks between family, school, and health services. Given the inherent complexity of these conditions, the need for a rigorous, multifaceted, and culturally sensitive approach is highlighted, integrating standardized psychometric instruments, qualitative observations, and the work of multidisciplinary teams as key elements for an accurate diagnosis and an effective intervention plan. Furthermore, constant updating of international classifications and validation of instruments for the Brazilian population are essential steps toward improving the quality of care for individuals with NDDs.
Early diagnosis is essential to minimize the impact on a child's overall development. Although each disorder has specific clinical manifestations, many share comorbidities and symptomatic overlap, requiring an integrated approach to assessment and treatment. Furthermore, the recognition of neurological diversity has fostered significant advances in how these disorders are understood, treated, and included in society.
However, it is crucial to recognize existing limitations. Available instruments are not always sufficiently sensitive to the cultural and socioeconomic specificities of the Brazilian population, requiring professionals to carefully analyze and contextualize results when interpreting them. This is compounded by the challenge of access, as many families still face significant barriers to accessing specialized services. Despite these challenges, future prospects are promising. Technological advances, such as the application of computerized tests and the use of artificial intelligence, tend to increase the accuracy and accessibility of assessments. Integration with neuroimaging and genetic data may also offer a more comprehensive understanding of NDDs.
Financial supportNone declared.
Research data availabilityThe full dataset supporting the findings of this study is available upon request to the corresponding author.
The authors declare no conflicts of interest.
Institution: Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Escola de Ciências da Saúde e da Vida e Escola de Medicina; Instituto do Cérebro da PUCRS, Porto Alegre, Brazil.




