

Analysis of the effectiveness of early Parental Coaching in the Autism Spectrum Disorder.
MethodRandomized, controlled and blinded clinical trial to analyze parent-child interaction videos.
ResultsThe sample consisted of 18 children being followed up at the Autism Outpatient Clinic of a Neuropediatric Center in southern Brazil diagnosed with Autism Spectrum Disorder, between 29 and 42 months of age, randomly allocated to two groups: the Study Group (SG; n=9), which received Parental Coaching performed by a professional certified by the Early Start Denver Model; and the Control Group (CG; n=9), which was in a routine follow-up, without treatment and training of parents by a trained professional. The parents of the SG were willing to attend weekly meetings and to apply the instructional techniques at home with their children. It took 12 weeks and an average of 2h per meeting.
ConclusionsThe learning rate for comprehensive development skills in the Early Start Denver Model checklist, such as receptive communication, expressive communication, social capacity, imitation, cognition, games, fine motor skills, gross motor skills, behavior, and personal independence was significantly higher in the SG, as well as the strategies and the quality of interaction between parents and children. Thus, Parental Coaching presents as a possibility of early intervention in children with Autism Spectrum Disorder.
Autism Spectrum Disorder (ASD) is a neurological development disorder characterized by significant and persistent difficulties in interaction and social communication, in addition to the stereotyped and repetitive patterns of behavior, activities, or interests.1,2
The effectiveness of early intervention in improving short-term results in ASD has led to the development of diagnostic measures for children, aiming to start treatment as early as possible.3 In the same way as the early diagnosis of children at risk for ASD, starting therapy is essential.
The prevalence of ASD has increased substantially worldwide, and according to the Centers for Disease Control and Prevention there is one child on the spectrum for every 68 children within the same age group, with a higher prevalence in males.4 Scientific literature indicates that the treatment for ASD generates higher expenses not only for the patient’s families but also for the US government, due to a loss in productivity and an increase in health costs during the patient’s life span, which can consume resources in a more significantly way.
Most of the populational data for ASD comes from developed countries, thus not describing the reality observed in the national context (Brazil) and in other countries with less favorable socioeconomic conditions.
The scientific research, theory, and clinical practice point out the importance and effectiveness of interventions involving parents, with the purpose of enhancing the development of children with developmental delay.5,6 Early intervention can occur right after birth or after diagnosis, even up to the period of early childhood.7
The Early Start Denver Model (ESDM) – Denver’s Early Model – consists of a comprehensive teaching program based on behavior analysis, applied in developmental psychology and relational approaches, focused on pre-school-aged children with ASD. It presents itself as an assertive model of early intervention, supported by a broad scope of literature.1,2,5,8–14 The model qualifies parents as the main agents and defenders of their children's development, recommending teaching them how to stimulate their child in their daily routines.11,14
In a controlled, randomized study carried out in 3 different centers, Rogers et al.5 applied the ESDM with parental education for a period of 12 weeks with an hour of daily training for the parents of 98 children. They investigated the effectiveness of parental involvement through Parental Coaching and observed an improvement in the parental interaction skills and the children’s development.
Parental Coaching is a type of intervention that has occupied a great focus of international research aimed at investigating assistive technologies.14–16 According to the American Academy of Pediatrics, parental involvement and action are essential for the best results.17
Parental Coaching based on ESDM is a process that takes place with a specific duration, directed by a qualified professional, who is objective and has training on specific teaching procedures, instructing parents and caregivers on how to deal with their children on the spectrum.14
Rogers et al. discussed Parental Coaching as a means for significant changes in children’s social communicative skills, as well as in the pattern of interaction established with their parents.14 The study presents strategies to improve the process of parental training with multimodal learning modes (videos, written materials, among others) and more frequent home visits. It also discusses the optimization of the time required for the training of caregivers as a relevant issue for guaranteeing the quality of treatment – the faster the parents commit to the training methods, the better the therapy for the child.
Early intervention in the first years of life is justified, as the great brain plasticity at this stage allows the establishment and reorganization of neural networks in response to environmental stimulation.2
Although early diagnosis is necessarily the gateway to intervention and a trigger for the caregivers to conduct the child's treatment process, in the Brazilian context there is still a significant gap between diagnosis and access to specialized health services.18
In this sense, viable means are needed for immediate access to the intervention, which guarantees the promotion of quality of life and development of infants and their families, having an increased emphasis within the international specialized literature.1,10 The general importance of early intervention for ASD is widely recognized and supported by numerous studies.1,2,5,8–13
Although the positive effects of ESDM are well documented, the feasibility and effectiveness of the model in daily community care services need to be assessed, since, from an economic point of view, they are not very adaptable to the needs of most of the population, because its implementation requires a large financial investment, intense dedication and commitment to the process, and a considerable amount of daily work hours.
The evaluation of evidence-based interventions in community settings is currently a necessary step in the field of intervention research to ensure that models developed in university settings are accessible and sustainable in services not supported by research funds.13 Due to the need to investigate economically viable treatments that guarantee access to early intervention for broad socioeconomic contexts, this research was dedicated to studying the applicability of Parental Coaching as an early intervention strategy and its effects on the quality of the interaction between parents and children.
Material and methodsThis is a randomized, controlled, and blinded clinical trial to assess the effectiveness of early Parental Coaching in ASD. The sample consisted of patients diagnosed with ASD, between 29 and 42 months of age, followed up in a specialized outpatient clinic at a Public University Hospital in southern Brazil, registered in the Brazilian Registry of Clinical Trials (REBEC) under the number RBR-44vc9n.
Twenty children and their guardians were selected based on the following inclusion criteria: a) physical conditions for effective collaboration in evaluations; b) age between 29 to 42 months; c) free and informed consent form (ICF) signed by parents or guardians; d) availability of parents or guardians to attend Parental Coaching weekly; e) absence of diagnosis of any impairment (visual, hearing, motor); f) up to a maximum of 4h of specialized care (speech therapy, occupational therapy, psychology). Two children and their parents were excluded due to unavailability to participate in all stages of the research.
Thus, 18 patients were randomly allocated to 2 groups: Study Group (SG) and Control Group (CG), with 9 children each. Even though the population size for this study research was small, the study managed to show its power by rating each allocated group by the number of eligible participants during the sample tests.
The parents in the SG received the Parental Coaching carried out by a professional certified in the ESDM, while the parents in the CG were under routine monitoring.
After the diagnosis by a specialist pediatrician and neuropediatrician, the initial evaluation was carried out using the instruments: ADOS-2 (Autism Diagnostic Observation Schedule – Second Edition); SON-R 21/2-7 (Revised Snijders-Oomen – two and a half to seven years); Early Start Denver Model Curriculum Checklist and the Denver Model commitment coding sheet for the analysis of the interaction videos between parents and children. After the 12 weeks, the ESDM Curriculum Checklist and the Denver Model commitment coding sheet were reapplied to determine the effects of the intervention.
The intervention consisted of weekly meetings lasting an average of 2h, covering topics such as: the diagnosis of ASD; children’s individual difficulties; parents’ motivation to attend each parent's individual meetings and goals with their child on how to help them. Then, measures were discussed to improve the performance of interactions between parents and children to favor the development and gain of skills in a natural environment. The selected themes used the book “An Early Start for Your Child with Autism: Using Everyday Activities to Help Kids Connect, Communicate, and Learn” as a base,11 with its chapters as topics for the family members’ training process.
After each meeting, the parents had the task of making a video in interaction with their child, practicing what had been proposed. This video was then analyzed by the professional, with an individual feedback, review of the previous topic at the next meeting and general feedback on the main points to be improved by the group. The main tips from each meeting were written on a board for the parents to take note with the purpose of remembering and putting them into practice. Parents were also encouraged to implement naturalistic therapeutic techniques from ESDM in their family routines and in play activities.
The evaluations carried out after the interventions were made by two ESDM-certified professionals, therefore guaranteeing blindness in the children’s development results and in the parents’ commitment.
The tests were completed in two different time spans (before and after), therefore making the blind tests feasible in relation to the fidelity punctuation showed in the videos. To ensure reliability and repeatability the data was stored into a drive with no personal identification; instead, it was identified with an alphabetic order, and the videos were distributed regardless of the allocation group.
The videos were analyzed by two ESDM-certified professionals in two specific moments, first during the evaluation and then revised twelve weeks after. The videos were shot at the evaluation room before applying any type of protocols. The videos lasted for 10min and showed the interaction between parents and patients in a controlled environment. To ensure faithfulness in the practice analyses the ESDM fidelity classification study system was applied, following administration and coding criteria (scores from 1 to 5) similar to the thirteen-item description manual (Rogers; Dawson, 2014).
Statistical analyses were performed using Student’s t-test (to estimate the difference between two averages, as age), Anova for repeated measures and Factorial Anova, with Duncan’s post-hoc test (to estimate the repeated averages between the two groups, before and after) and Kruskal-Wallis’s Anova with Wilcoxon’s and Mann-Whitney’s post-hoc test (to estimate the repeated medians between the two groups, before and after).
To ensure reproducibility between the evaluators during the tests the Kappa coefficient of agreement was applied in different variable categories (fidelity area assessment), and the Spearman correlation coefficient was applied in the continuous variables (fidelity scores).
The number of subjects per group was calculated based on a significance level of 0.05, statistical power of 0.90 and moderate effect magnitude (ƒ2=0.50), according to the classification established by Cohen.19 The sample thus provides a 90% test power, with a 5% significance level for all tests used (Statistica 10.0 Statsoft®). The research was approved by the Research Ethics Committee of the Institution, and at the end of the research the same series of Parental Coaching was carried out with the parents of the CG patients.
ResultsAll children were attending daycare or school, and in both groups 4 were female (22.2%) and 14 were male (77.8%), with an average age of 35.3±3.9 months (p>0.05).
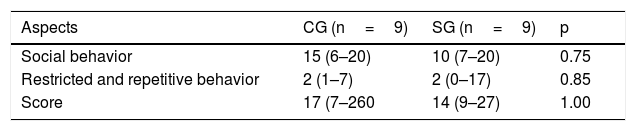
The average age of children at the time of the intervention was 3.3±0.9 years in the SG and 3.4±0.9 years in the CG (p=0.79). In both groups, 3 children were classified as being in the autistic spectrum (33.3%), and 6 as autistic (66.7%) (p=1.00). There was no significant difference between the groups regarding the Observation Scale for the Diagnosis of Autism (p>0.05) (Table 1).
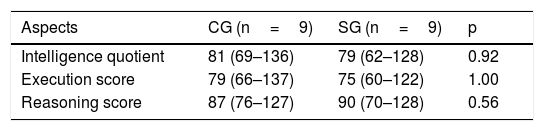
The medians of the intelligence quotient, execution score and reasoning score were also similar between groups (p>0.05) (Table 2).
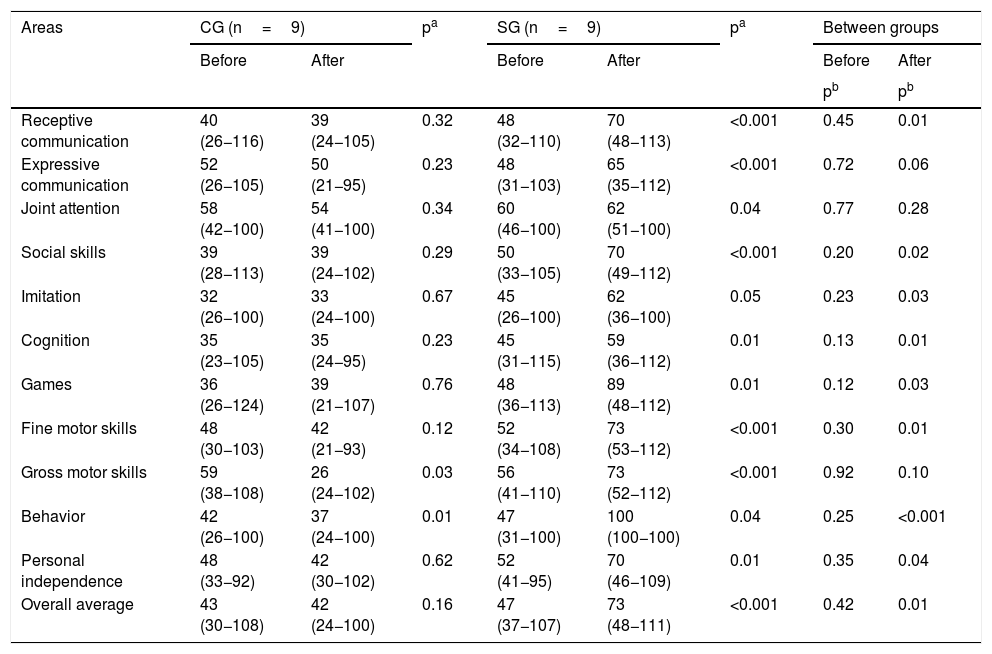
Among the CG patients, a significant decrease in gross motor skills (p=0.03) and behavior (p=0.01) was observed. In the SG there was always a significant increase in the learning rate, with the exception of Imitation, whose increase had a borderline significance level (p=0.05) (Table 3).
Learning rate, 2019.
| Areas | CG (n=9) | pa | SG (n=9) | pa | Between groups | |||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | |||
| pb | pb | |||||||
| Receptive communication | 40 (26−116) | 39 (24−105) | 0.32 | 48 (32−110) | 70 (48−113) | <0.001 | 0.45 | 0.01 |
| Expressive communication | 52 (26−105) | 50 (21−95) | 0.23 | 48 (31−103) | 65 (35−112) | <0.001 | 0.72 | 0.06 |
| Joint attention | 58 (42−100) | 54 (41−100) | 0.34 | 60 (46−100) | 62 (51−100) | 0.04 | 0.77 | 0.28 |
| Social skills | 39 (28−113) | 39 (24−102) | 0.29 | 50 (33−105) | 70 (49−112) | <0.001 | 0.20 | 0.02 |
| Imitation | 32 (26−100) | 33 (24−100) | 0.67 | 45 (26−100) | 62 (36−100) | 0.05 | 0.23 | 0.03 |
| Cognition | 35 (23−105) | 35 (24−95) | 0.23 | 45 (31−115) | 59 (36−112) | 0.01 | 0.13 | 0.01 |
| Games | 36 (26−124) | 39 (21−107) | 0.76 | 48 (36−113) | 89 (48−112) | 0.01 | 0.12 | 0.03 |
| Fine motor skills | 48 (30−103) | 42 (21−93) | 0.12 | 52 (34−108) | 73 (53−112) | <0.001 | 0.30 | 0.01 |
| Gross motor skills | 59 (38−108) | 26 (24−102) | 0.03 | 56 (41−110) | 73 (52−112) | <0.001 | 0.92 | 0.10 |
| Behavior | 42 (26−100) | 37 (24−100) | 0.01 | 47 (31−100) | 100 (100−100) | 0.04 | 0.25 | <0.001 |
| Personal independence | 48 (33−92) | 42 (30−102) | 0.62 | 52 (41−95) | 70 (46−109) | 0.01 | 0.35 | 0.04 |
| Overall average | 43 (30−108) | 42 (24−100) | 0.16 | 47 (37−107) | 73 (48−111) | <0.001 | 0.42 | 0.01 |
Note: Kruskal-Wallis Anova.
It was always observed a gain in the learning rate among the patients of the SG, while in the CG values were always negative. For all areas, except for Imitation, the SG showed a significantly higher learning rate than the CG (p<0.001) (Fig. 1).

In the analysis of the parental commitment carried out by two evaluators, an almost perfect agreement was observed for commitment and punctuation and a substantial agreement for the areas of management of unwanted behavior and quality of dyadic commitment. For sensitivity to communicative cues and transition of activities, the agreement between the evaluators was classified as moderate and for the others, as regular or weak.
DiscussionThe ASD needs extensive research within the Brazilian context, since the perception of its incidence in the population, resources for early diagnosis, and access to intervention are still scarce, since there is still a reality of late diagnosis in the national scenario, as described by Ribeiro et al.20
The qualitative report of the parents during the interviews indicated that the diagnosis was made at around 3 years of age, on average, even with recognition of signs that already worried them and caused insecurity from a very early age.
There is, therefore, an important time gap between the perception of the first signs of the disorder and the actual effective diagnosis. This situation does not seem to be restricted to the participants of this research, but rather a common reality for families living within this context, and it is also described by the specialized literature.20–22
Early diagnosis is being increasingly discussed in Brazil and is associated with a better prognosis.10,20,21 Early diagnosis and intervention are crucial measures to be taken during the first years of children’s development, an important window of neuroplasticity. Early and intensive intervention, as studies point out,16,23 is a key factor that certainly contributes to a better prognosis in most cases, being a determining measure for children to develop their full potential, promoting more favorable outcomes for them and their families.
However, in the Brazilian public health context, the reality of the majority of the population is incompatible with the treatment indications currently prevalent, and more than 70% of Brazilians depend exclusively on SUS,24 the Unified Health System.
The intervention proposal established and examined by the present study has the purpose of serving as an alternative treatment while families await intervention or simultaneously with specialized therapies.
Published studies describe this intervention model through Parental Coaching in an individualized way,5,8,10,14,16,25 which in the Brazilian reality is not economically viable for the public health system. In this sense, it was sought to implement the Parental Coaching program, but in groups, lasting 12 weeks, like how it is done individually. In the Brazilian literature, articles published with this same theme were not found, which proves with greater emphasis the need for further studies.
Through group Parental Coaching it was possible to involve parents and make them agents that multiply opportunities in a time frame compatible with the most fruitful developmental window of the child's life. With this, it is possible to ensure these families an economically viable and effective professional monitoring in improving the relationship between parents and children, as well as promoting a better quality of life in the family circle. Thus, it presents itself as a way to optimize access to early intervention.
In a recent research, Rogers et al.14 described some important points in the training of parents, which may be associated with the findings of this research, such as favoring generalization, high intensity of daily learning opportunities and significantly lower cost than those performed by specialized therapists.
It is noticed that parents have learned to understand the role of the behavior, not to reinforce inappropriate behaviors and to use appropriate strategies to provoke more adaptive substitute behaviors in their children. Regarding the quality of the dyadic commitment, parents found strategies to become play partners.
Children started to perceive their caregivers and establish interaction dynamics alternating shifts. The awareness of the presence of the other was assessed by means of behavioral indications: shared or directed gaze, intentional communicative exchanges and smiles. It was observed that reciprocity and social commitment permeated teaching activities.
The data presented in relation to the instructional techniques and improvement of the parent-child interaction were also found in previous research such as that of Waddington et al.,25 who observed that all mothers increased the number of techniques after the intervention. The findings on improving the commitment score for implementing the techniques were also found by Vismara et al.16
The analysis of the interaction between parents and children for the codification of scores and verification of commitment was performed with a sample of games, using videos of 10min of interaction between them, pre- and post-Parental Coaching, similar to the analysis applied by Waddington et al.25
Based on Parental Coaching, parents of children with ASD were able to achieve quality of interaction with a good standard, according to the ESDM implementation commitment criteria established by Rogers et al.5 Therefore, the therapeutic intervention performed has a great possibility of being generalized to other groups with similar conditions.
Given these results, it is possible to highlight the importance of parents in the process of treating their children. In this sense, parents can be the greatest allies of treatment, applying interventions for children with ASD in their natural context and promoting better development conditions for children. Such results corroborate evidence already indicated by the international literature in the last 10 years, in studies with similar hypotheses.6,8,10
Although they deserve further investigation in future research, it is possible to suggest that such a model is an accessible measure to be implemented by the Unified Health System, since it can enhance the development of children with early diagnosis and who are unable to initiate appropriate treatment.
The growing study of Parental Coaching5,8,10,14,16,25 indicates an economically viable path with significant potential to reduce the wait for treatment, in addition to having important advantages, such as the qualification of caregivers and the improvement in the development and interaction of parents and children.
Based on Parental Coaching, parents can also be agents of their children's learning in natural situations, which, without specific guidance, tend to not be rich in learning opportunities for children with ASD as they usually are for neurotypical children.6 In this sense, Parental Coaching acts as a job with great potential for generalization, facilitating the maintenance of earnings, and a means of reducing parental stress, in addition to being an alternative with reduced costs when compared to interventions conducted only by teams of specialists.
“Training parents to transform children’s lives.”26
Parental training has been recommended by the World Health Organization for families with children with developmental delays. These disorders have been a major public health challenge in the world, as most children do not have access to specialized treatment.26
Restriction and unavailability of the sample for the age group studied were a limitation of the study, which is why the type II error may have occurred in the evaluation of the imitation learning rate (p=0.05) and Expressive Communication in the evaluation before and after (p=0.06).
Therefore, this study brings its contribution with significant results from an early intervention program, carried out with groups of parents and children, in a public health system, which can have a decisive impact on the development and quality of life of these children, guaranteeing the right to have access to a public health care system. Despite the limitations regarding a small sample size, the results of this study indicate the use of Parental Coaching as an important element in the treatment of ASD.
Future investigations that consider a larger number of participants comprising the socioeconomic and cultural diversity present in the Brazilian context need to be conducted, in order to prove denser evidence regarding the applicability of this type of training in a public health care context.
Conflicts of interestThe authors declare no conflicts of interest.
The study was performed at the Programa de Pós-Graduação em Saúde da Criança e do Adolescente and Universidade Federal do Paraná, Hospital das Clínicas, Centro de Neurologia Pediátrica (CHC-UFPR), Curitiba, PR, Brazil.




