
To investigate the indoor environmental risk factors to provide measures for the prevention and control of otitis in preschool children.
MethodIn this cross-sectional study, a questionnaire survey was administered to preschool children aged 2–7 years from 60 kindergartens in six districts of Urumqi City in August 2019. Multiple regression was run to predict influence factors for otitis media in preschool children.
ResultA total of 8153 valid questionnaires were collected. After adjusting for age, the prevalence of otitis among preschool children in Urumqi was 13.1%. Multivariate logistic regression showed that previous antibiotic treatment, treatment with one to two antibiotics before 1 year of age, presence of walls with aqueous or latex paint, use of carpet floor bedding in rooms, newly decorated homes of mothers before pregnancy, purchase of new furniture for homes of children at 0–1 year of age, and presence of flowering plants in the residence of children at 0–1 years of age were all identified as risk factors for the development of otitis in children.
ConclusionParents should also pay attention to indoor living environments, and reduce indoor renovation in the homes of children during their growth and development, which can positively improve children's indoor living environment, thus effectively preventing otitis in preschool children.
Environmental pollution contributes differentially to health hazards in different populations, in which children belong to typical susceptible groups. Compared with adults, children have a large amount of activity, a fast breathing rate, and rapid development of body structure and organs. Their respiratory, immune, and other systems are not well developed, and they are more sensitive to harmful substances in the environment.1 Studies have shown that the indoor environment, renovation of dwellings, dampness inside dwellings, heating and ventilation of buildings, indoor air quality, and life habits of households are related to preschool child health.2,3 Otitis is an inflammation of the ear. It is usually divided into two types (otitis externa and otitis media) and is an infectious disease secondary to the common cold in children.4 Presently, studies on otitis in preschool children have focused on the effects of medication, and there are few investigations on the indoor environmental factors associated with the occurrence of otitis in preschool children. Concurrently, children's hearing organs and brains were irreversibly injured due to the lack of attention paid by parents to the prevention of acute otitis attacks. Therefore, it is necessary to extensively study the health effects of indoor environmental pollution on preschool children in China. This study was conducted from April to August 2019 and investigated residential environmental and otitis risk factors of preschool children in 60 kindergartens in Urumqi. This study aimed to explore the potential risk factors affecting the occurrence of otitis in preschool children and provide corresponding measures for the prevention of such diseases.
MethodsSubjectsStratified cluster random sampling was used in this study. According to the administrative area division of Urumqi city, there are six districts (Xinshi, Shayibake, Tianshan, Shuimogou, Toutunhe, and Midong), and 8–12 kindergartens were randomly selected. This study was approved by the ethics committee of Fudan University, and all parents of the children provided written informed consent.
QuestionnaireThe contents of this questionnaire refer to those used in the International Study of Asthma and Allergies in Childhood (ISAAC)5 and Dampness in buildings and health (DBH)6 survey studies. The survey consisted of six parts: (1) demographic characteristics, including sex, ethnicity, educational level, and home address; (2) feeding status, including whether they were single children, whether they were breastfed, breastfeeding duration, and age at which the child attended kindergarten; (3) health of children and family members, including otitis, pneumonia, allergic rhinitis, and other diseases and related symptoms; (4) children's residential environment, including housing type, renovation, whether the furniture was newly purchased, ventilation, and smoke evacuation; (5) lifestyle habits, including animals, plants, cleaning frequency, and smoking in the residence of the child; (6) dietary habits, including the type and frequency of meal. Before the initiation of the survey, the subject group initially contacted the Education Bureau of Urumqi City and the kindergarten gardener, and uniform professional training was provided to the teachers involved in the survey class. A questionnaire was uniformly distributed by the preschool teachers to the parents of the children in their kindergartens. The questionnaires were completed by the parents or guardians of the children when they were taken home. They were asked to fill out the questionnaire within 1 week and hand it over to the responsible teacher in the kindergarten. The teachers returned the questionnaires and sent them together to the City Education Bureau of Urumqi. All questionnaires were reviewed by more than two trained subject team members and ineligible questionnaires were excluded.
Statistical analysesThe primary objective of this study was to analyze the prevalence and indoor environment risk factors of otitis among preschool children.
The database was established using EpiData 3.1, and SPSS 25.0 software was used to complete the data analysis as it is suitable for the analysis of complex samples. Initially, univariate analysis was performed using χ2 tests between independent variables and the outcome variable, variables with P < 0.01 were selected to build the multivariate model. A multiple regression model was adopted with otitis among preschool children (yes or no) as a dependent variable. Each variable was selected using the "enter method," Differences with P < 0.05 were considered statistically significant. The α level was set at 0.05.
Ethics approval and consent to participateThe study was conducted strictly in accordance with the Declaration of Helsinki and approved by the research ethics committee of Fudan University (protocol no. IRB00002408 & FWA00002399), all parents and class teachers of the children under investigation have signed written informed consent.
ResultsGeneral condition of the investigated subjectsA total of 10000 questionnaires were distributed, and 8153 valid questionnaires were returned, resulting in an 81.53% response rate, including 4180 boys (51.3%) and 3973 girls (48.7%). The youngest age was 2.00 years, and the oldest was 7.83 years, with a mean age of 5.27 ± 1.10 years. Moreover, 7010 individuals were of Han ethnicity (86.0%), and 1143 individuals were of other ethnicities (14.0%). Furthermore, 4569 children were single children (56.0%), and 3584 were not a single child (44.0%).
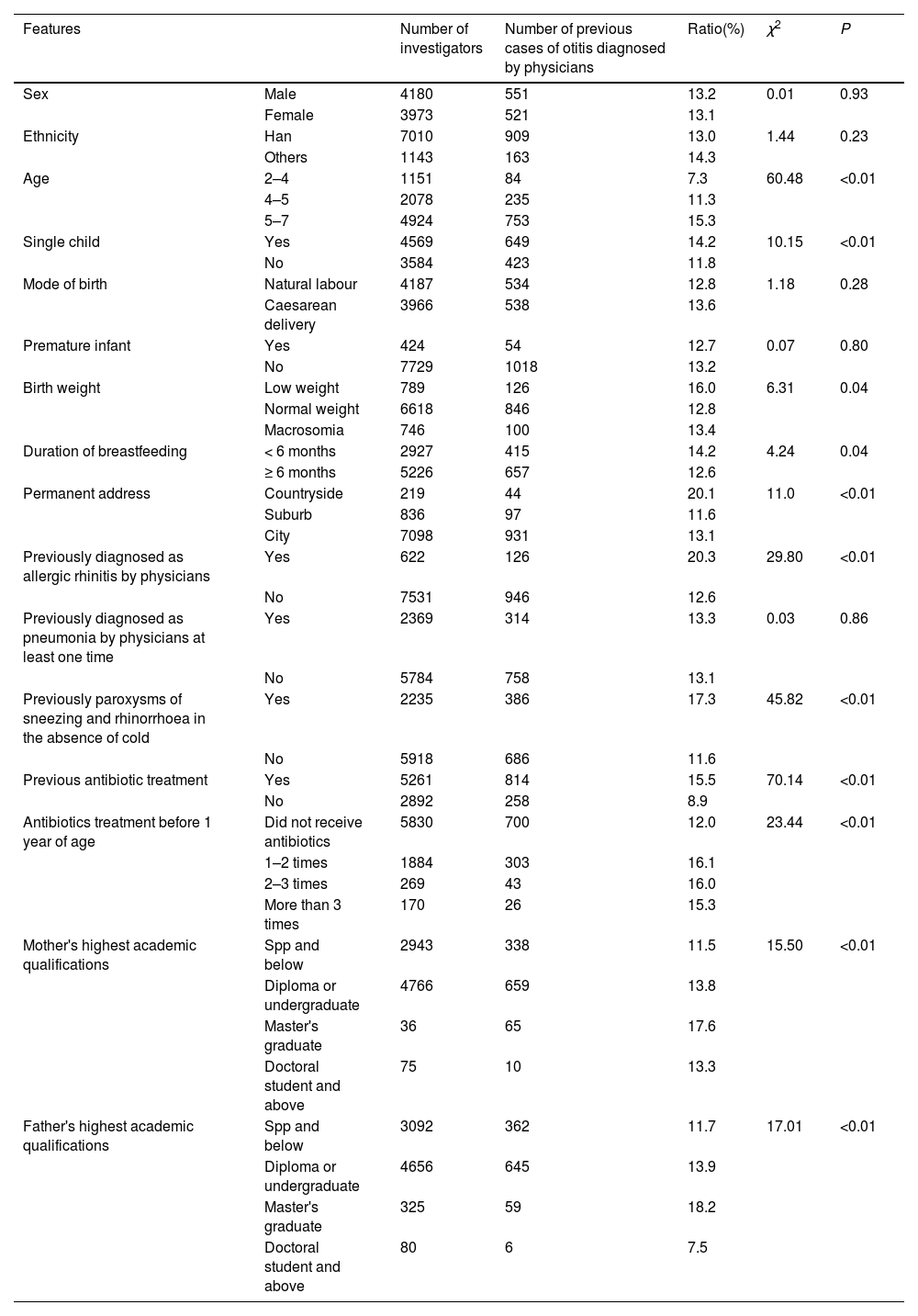
Prevalence of otitisThe characteristics of preschool children in Urumqi City who was diagnosed with otitis by physicians as reported by their parents are shown in Table 1. The findings showed that 1072 of 8153 children had at least one definite diagnosis of otitis by a physician. After adjusting for age, the prevalence of otitis in preschool children in Urumqi City was 13.1%. Moreover, a higher prevalence was noted in the age group of 5–7 years, singletons, children in rural areas, children with a previous physician diagnosis of allergic rhinitis, children who previously reported symptoms of sneezing and rhinorrhoea in the absence of a cold, children with previous antibiotic exposure, children who had received antibiotics before 1 year of age, and children whose mothers’ and fathers’ highest qualifications were master's postgraduate students compared to their counterparts (all P < 0.05).
Characteristics of preschool children in Urumqi, China who were diagnosed with otitis by physicians (n = 8153).
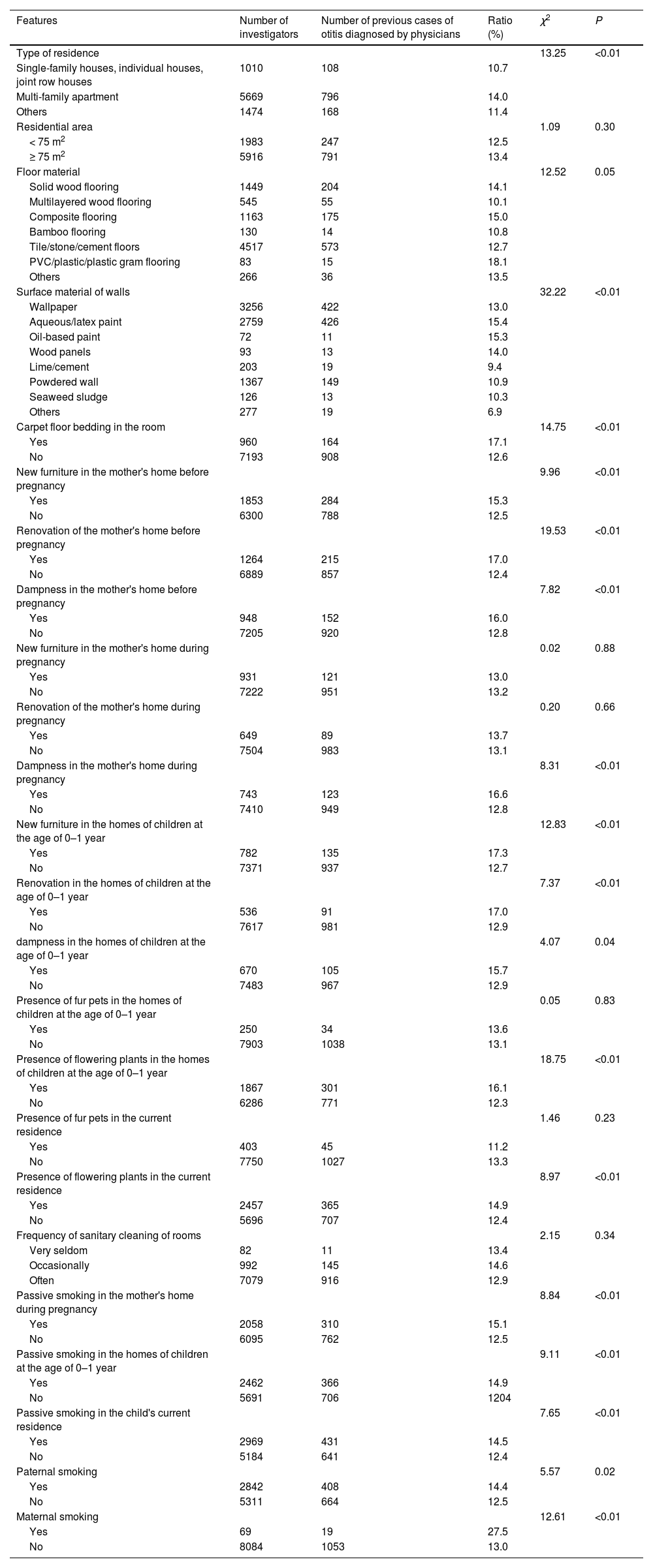
The results of the univariate analysis of the prevalence of otitis in preschool children and indoor environmental variables in Urumqi City are shown in Table 2. The results of this analysis showed that the type of residence, the surface material of the walls, carpet floor bedding in the room, new furniture in the mother's home before pregnancy, renovation of the mother's home before pregnancy, dampness in the mother's home before pregnancy, dampness in the mother's home during pregnancy, new furniture in the homes of children at the age of 0–1 year, newly decorated homes of children at the age of 0–1 year, dampness in the homes of children at the age of 0–1 year, presence of flowering plants in the homes of children at the age of 0–1 year, presence of flowering in the current residence, passive smoking in the mother's home during pregnancy, passive smoking in the homes of children at the age of 0–1 year, passive smoking in the child's current residence, paternal smoking, and maternal smoking were the main indoor environmental factors associated with otitis in children (all P < 0.05).
Univariate analysis of otitis and indoor environmental variables in preschool children in Urumqi, China (n = 8153).
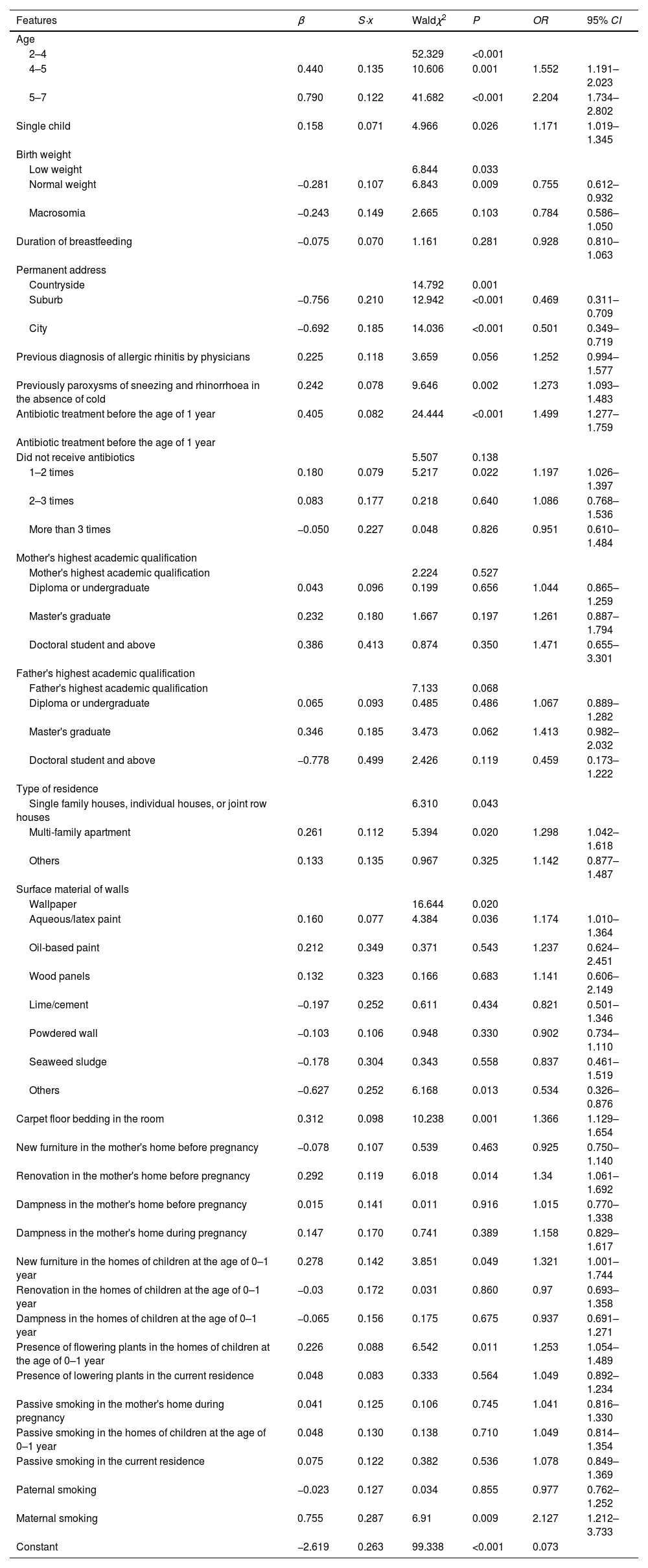
The results of the multivariate logistic regression analysis of otitis in preschool children in Urumqi City are shown in Table 3. The results of the analysis of different characteristics and univariate analysis of indoor environment variables with or without otitis as dependent variables (0 = no; 1 = yes) were introduced into the logistic regression model. Of the 28 variables in the final residence main effect model, 14 were associated with the occurrence of rhinitis-related symptoms in children.
Multivariate logistic regression analysis of otitis in preschool children in Urumqi, China (n = 8153).
Ages of 4–5 years (OR = 1.55, 95% CI = 1.19–2.02) and 5–7 years (OR = 2.20, 95% CI = 1.73–2.80), single child (OR = 1.17, 95% CI = 1.02–1.35), previous antibiotic exposure (OR = 1.50, 95% CI = 1.28–1.76) and one or two episodes of antibiotic exposure before the age of 1 year (OR = 1.20, 95% CI = 1.03–1.40), multiple apartment dwellings (OR = 1.30, 95% CI = 1.04–1.62), and presence of wall materials with aqueous paint/latex paint (OR = 1.17, 95% CI = 1.01–1.36) increased the risk of otitis in children. Carpet floor bedding in the rooms (OR = 1.37, 95% CI = 1.13–1.65), renovation in the mother's home before pregnancy (OR = 1.34, 95% CI = 1.06–1.69), new furniture in the homes of children at the age of 0–1 year (OR = 1.32, 95% CI = 1.00–1.74), presence of flowering plants in the homes of children at the age of 0–1 year (OR = 1.25, 95% CI = 1.05–1.49), and maternal smoking (OR = 2.13, 95% CI = 1.21–3.73) were risk factors of otitis in children. Normal birth weight (OR = 0.76, 95% CI = 0.61–0.93), residence in a suburban (OR = 0.47, 95% CI = 0.31–0.71) or urban areas (OR = 0.50, 95% CI = 0.35–0.72), and surface materials of walls (OR = 0.53, 95% CI = 0.33–0.88) were considered as protective factors of otitis in children.
DiscussionOtitis in children is mainly caused by bacteria, of which 69.7% are gram-positive bacteria, 16.7% are gram-negative bacteria, and 13.6% are fungi.7 Presently, China's medical treatment places otitis under the category of the five organ diseases, so some pediatricians have a vague understanding of it, which leads to a missed diagnosis by physicians, thus concluding that the prevalence of otitis in Chinese children is low and not paid attention to. However, according to the results of this survey, the prevalence of otitis in preschool children in Urumqi was 13.1%, which was higher than the prevalence (11.9%) of otitis among 4618 children in Urumqi investigated by Wang8 in 2013. This further suggests that more attention should be paid to the prevalence of otitis in preschool children. At the onset of otitis, a vast majority of physicians provide antibiotic therapy. In a study by Trinh et al.,9 the antibiotic prescription rate for otitis was 68–80 per 100 visits. Several international guidelines recommend antibiotics for children aged < 2 years with acute otitis media. However, in older children, only cases of high fever and severe ear pain require antibiotics. Overuse and inappropriate use of antibiotics are the main reasons for the emergence of antibiotic resistance.10,11 Among them, aminoglycoside antibiotics, such as streptomycin and gentamicin, have good efficacy against diseases caused by bacteria. However, its prolonged use causes its accumulation in the inner ear lymph nodes, causing the death of hair cells in the inner ear and irreversible ototoxic effects.12 The results of the present study also showed that the prevalence of otitis was 6.6% higher in children who had been treated with antibiotics than in those who had not. It was speculated that the non-standard use or abuse of antibiotics in the early years changed the susceptibility of pathogenic otitis bacteria to antibiotics, resulting in lower resistance and higher prevalence of otitis in preschool children.
The impact of the indoor environment on human health has gained much attention from the international community,13–15 especially for preschool children whose various organs and systems of the body are not yet developmentally mature. With the increase in living standards of the Chinese residents, there is also an increasing variety of furniture and new synthetic materials in dwellings, with a consequent exposure problem of chemical components. Shin et al.16 showed that formaldehyde can enter the body through the skin and eye contact, inducing the expression of inflammatory factors and mucins in human ear epithelial cells, thereby increasing the probability of developing otitis in children. Formaldehyde in residential environments mainly originates from decorating with artificial sheets, furniture, cellophane, and various types of wall materials. The results of the present study similarly showed that the purchase of new furniture and renovation in the mother's home before pregnancy and the purchase of new furniture and renovation in the homes of children at the age of 0–1 year were both associated with the development of otitis in preschool children. Concurrently, summer in Urumqi, Xinjiang, has long promoted a high-temperature environment, and the indoor temperature increases, as does the rate of formaldehyde release. A high-temperature environment is more conducive to the breeding and reproduction of fungi, which further expands the exposure risk of preschool children. Indoor decorative materials have been repeatedly associated with the occurrence of respiratory diseases in children.2,17,18 The results of this study showed that floor material, wall surface material, and carpet placement in a room were associated with otitis occurrence in children. It is presumed that newly purchased furniture and renovation materials in dwellings have some volatilization of chemical composition. Prolonged environmental exposure leads to impairment of the respiratory and immune systems of children, who are more susceptible to invasive bacterial infections that induce otitis.
Several review studies19,20 have shown that exposure to mold and dampness in the home residential environment is an important indoor environmental risk factor. Dampness in dwellings promotes the breeding of indoor microbes, of which bacteria and mold are the most common. Bacteria can affect the child's immune system, and molds can be harmful to human health by suspending them in the air. Prolonged indoor dampness also leads to heavy multiplication of dust mites, which in turn triggers disease reactions, such as allergic rhinitis, in children.21 Moreover, pests raised in damp dwellings, such as mice and cockroaches, carry pathogenic bacteria. Preschool children have a stronger desire to explore the world spirit, and a larger range of indoor activities, and have greater exposure to these causative factors than adults who remain indoors for longer periods. However, the results of the present study found that dampness in the home before versus during pregnancy of mothers was not a risk factor for the development of otitis media in preschool children.
This study has some limitations. Because this study did not consider risk factors for outdoor and child exposure in preschool and used a cross-sectional survey with poor causal ability, the results may have been biased. Otitis includes otitis externa and otitis media, which are further divided into acute and chronic otitis media. As defined above, one of these phenomena and the occurrence of otitis were considered. Therefore, the calculated prevalence of otitis in this study was higher than that in any of the abovementioned studies. Elucidation of specific risk factors for the development of otitis in preschool children should be confirmed by population-based cohort studies to allow further observation of environmental and developmental relationships with disease development in childhood.
ConclusionThe prevalence of otitis in preschool children is high, and it has a certain association with indoor environmental factors. Residence renovation, tide, and humidity during pregnancy are all risk factors for the development of otitis in preschool children. The diagnosis of otitis in children should be added to the consideration of environmental factors when they come to relevant units such as hospitals, and parents should also pay attention to the indoor living environment. Reduction of indoor renovation of the dwellings of children during their growth and development and regular vector abatement of the dwellings actively improve children's indoor living environments, thereby effectively preventing otitis in preschool children.
Data availabilityThe datasets generated and/or analyzed during the current study are not publicly available due to the data belonging to the School of Public Health of Fudan University but are available from the corresponding author upon reasonable request.
FundingThis study was supported by the National Natural Science Foundation of China (grant no. 81660140, 81860179); Teacher's professional development project of the Shanghai Municipal Education Commission and High-Level Local University Construction Projects of Shanghai University of Medicine & Health Sciences; The Key Discipline of the 14th 5-Year Plan in Xinjiang Uygur Autonomous Region-Public Health and Preventive Medicine.





