



Systematically assess studies that have analyzed the psychometric properties of multichannel intraluminal impedance-pH for the diagnosis of gastroesophageal reflux. Systematically verify studies that have analyzed the psychometric properties of multichannel intraluminal impedance-pH regarding the diagnosis of gastroesophageal reflux disease in pediatric patients.
MethodsSystematic review considering specific descriptors (children and adolescents, gastroesophageal reflux disease and multichannel intraluminal impedance-pH) and their synonyms. The systematic search was carried out in the MEDLINE/Ovid, Scopus, and Embase databases, considering the period from October 2017 to December 2018. This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), which was used for study selection. The psychometric properties described in the studies were: sensitivity, specificity, accuracy, and reproducibility.
ResultsSensitivity was discussed in most studies, with a result of more than 70% in four of them. Specificity was assessed only in conjunction with sensitivity, with values from 23% to 25% in two studies, and it reached 80% in a single study. Accuracy was assessed higher than 76% in one of the selected articles. The methodological quality of the studies demonstrated low risk of bias, and there was no significant concern related to applicability of the studies.
ConclusionsAccording to the selected studies, multichannel intraluminal impedance-pH was considered a safe and effective tool, presenting higher sensitivity values than pHmetry regarding the diagnosis of gastroesophageal reflux disease.
Avaliar sistematicamente estudos que analisaram propriedades psicométricas da impedância intraluminal multicanal associada à pHmetria (IIM-pH) no diagnóstico de refluxo gastroesofágico. Verificar sistematicamente estudos que analisaram as propriedades psicométricas de impedância intraluminal multicanal associada à pHmetria em relação ao diagnóstico da doença do refluxo gastroesofágico em pacientes pediátricos.
MétodosRevisão sistemática que considerou descritores específicos (crianças e adolescentes, doença do refluxo gastroesofágico e impedância intraluminal multicanal associada à pHmetria) e seus sinônimos. A busca sistemática foi realizada nas bases de dados Medline/ Ovid, Scopus e Embase e considerou o período de outubro de 2017 a dezembro de 2018. Esta revisão foi realizada de acordo com o checklist Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Prisma), usado para seleção de estudos. As propriedades psicométricas descritas nos estudos foram: sensibilidade, especificidade, acurácia e reprodutibilidade.
ResultadosA sensibilidade foi discutida na maioria dos estudos, com um resultado de mais de 70% em quatro deles. A especificidade foi avaliada apenas em conjunto com a sensibilidade, com valores em torno de 23 a 25% em dois estudos, e alcançou 80% em um único estudo. A acurácia foi avaliada em mais de 76% em um dos artigos selecionados. A qualidade metodológica dos estudos demonstrou baixo risco de viés e nenhuma consideração significativa relacionada à aplicabilidade dos estudos.
ConclusõesDe acordo com os estudos selecionados, a impedância intraluminal multicanal associada à pHmetria foi considerada uma ferramenta segura e eficaz, apresentou valores de sensibilidade superiores à pHmetria no diagnóstico da doença do refluxo gastroesofágico.
Gastroesophageal reflux (GER) is defined as the physiological, involuntary, and asymptomatic passage of gastric contents into the esophagus.1,2 When a condition is developed where gastroesophageal reflux causes troublesome symptoms such as heartburn, crying, irritability, sleep disturbance, cough, or complications (pneumonia, imminent risk of life, laryngitis, otitis), it is considered gastroesophageal reflux disease (GERD).3–5
Strategies to document the diagnosis of GERD are complex because several types of instruments and tests can be used. The barium swallow X-ray test, scintigraphy, and abdominal ultrasonography can be considered complementary exams.5 Upper gastrointestinal endoscopy (UGE) conducted with or without esophageal, stomach, or duodenum biopsy and manometry make it possible to analyze GERD complications.1–5 Moreover, the pHmetry defines the episodes of acid GER and their relation to the symptoms.4
However, it is necessary to use these instruments in a complementary and/or associated way, since individually they are useful to assess anatomy, motility, symptomatology, or possible complications. Currently, multichannel intraluminal impedance-pH (MIIpH) is considered the gold standard test for the direct diagnosis of GERD.4–6
MIIpH can determine if esophageal content is present and its flow (retrograde or anterograde), by analyzing variation of the electrical conductance (checked by multiple sensors) and simultaneously monitoring intraesophageal pH.4,5 It can also verify physical properties of the bolus: fluid, gaseous, or mixed; the relation of the bolus movement with the prandial period and with the symptoms, also making it possible to identify acid and non-acidic events, in association with the intraesophageal pH.4–6 The efficacy of MIIpH regarding GERD diagnosis has been investigated, discussed, and recently diffused in clinical practice.5,7
Safety and efficacy confirmation of this test allows its indication and choice by health professionals, aiming a better cost-benefit relation and adjustments of the resources available in diagnostic centers.7–10 One of the strategies used for quality verification is the evaluation of the psychometric properties (PP) and their outcome variables.
PP have demonstrated to be important for the assessment of tests used to diagnose diseases.11–13 Among the variables analyzed regarding PP, there are the following: reliability, internal consistency, validity, responsiveness, reproducibility, and viability.14 Such variables aim to avoid compromising the reliability of the tests and to make more adequate and organized measurements possible, determining well-established criteria for health professionals to be able to select the most accurate test.
The present review aimed to systematically verify studies that analyzed the PP of MIIpH for the diagnosis of GER in children and adolescents.
MethodsData source and search strategyThe literature search was carried out in the following databases: MEDLINE via Ovid, Scopus, and Embase, using specific descriptors and their synonyms according to the Medical Subject Headings (MeSH) and Emtree (Embase Subject Headings): “Infant,” “Newborn,” “Child,” “Pediatrics,” “Adolescent,” “Gastroesophageal Reflux,” “Multichannel Intraluminal Impedance-pH,” and its variations. The detailed search strategy with the terms used for this study can be found in Appendix1.
The search strategy was carried out from October 2017 to December 2018. Articles in English, Spanish, or Portuguese were considered. No search filters were used regarding date of the studies.
Study selectionThis systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).15 Selection of the studies was conducted by two independent evaluators, according to the pre-established criteria. In case of discrepancies, a third evaluator was consulted for a final decision. In the first step, after searching the databases, the duplicates were removed; subsequently, the titles and abstracts were selected; finally, the remaining articles were read in full. Manual searches were performed regarding the references of the studies included in the final review process.
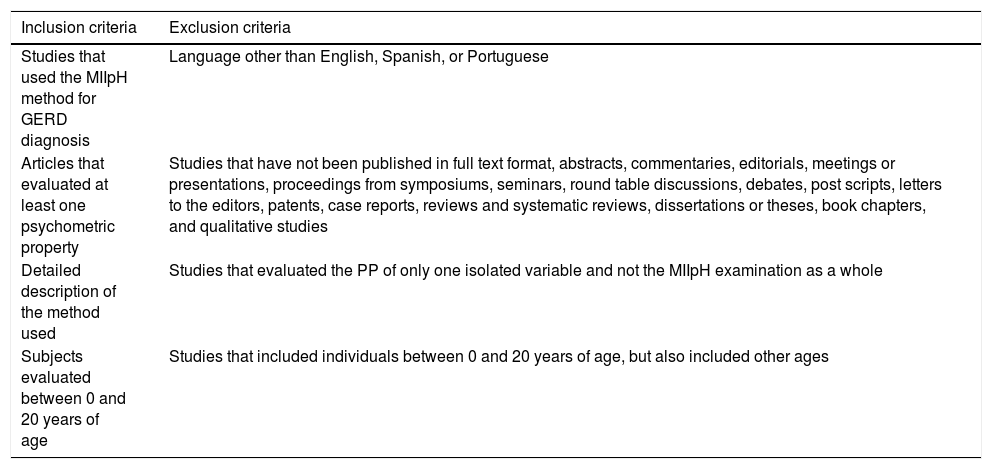
Inclusion and exclusion processThe present study included cross-sectional, randomized, or quasi-randomized studies that presented analyses of some PP regarding MIIpH as a diagnostic tool for GER in pediatric patients. Texts that were not presented in full and studies related to the diagnosis of diseases other than GERD were excluded. Articles that assessed the PP of only one isolated variable and not the MIIpH examination as a whole were also excluded. The inclusion and exclusion criteria are described in Table 1.
Description of inclusion and exclusion criteria.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Studies that used the MIIpH method for GERD diagnosis | Language other than English, Spanish, or Portuguese |
| Articles that evaluated at least one psychometric property | Studies that have not been published in full text format, abstracts, commentaries, editorials, meetings or presentations, proceedings from symposiums, seminars, round table discussions, debates, post scripts, letters to the editors, patents, case reports, reviews and systematic reviews, dissertations or theses, book chapters, and qualitative studies |
| Detailed description of the method used | Studies that evaluated the PP of only one isolated variable and not the MIIpH examination as a whole |
| Subjects evaluated between 0 and 20 years of age | Studies that included individuals between 0 and 20 years of age, but also included other ages |
GERD, gastroesophageal reflux disease; MIIpH, multichannel intraluminal impedance and pH monitoring; PP, psychometric properties.
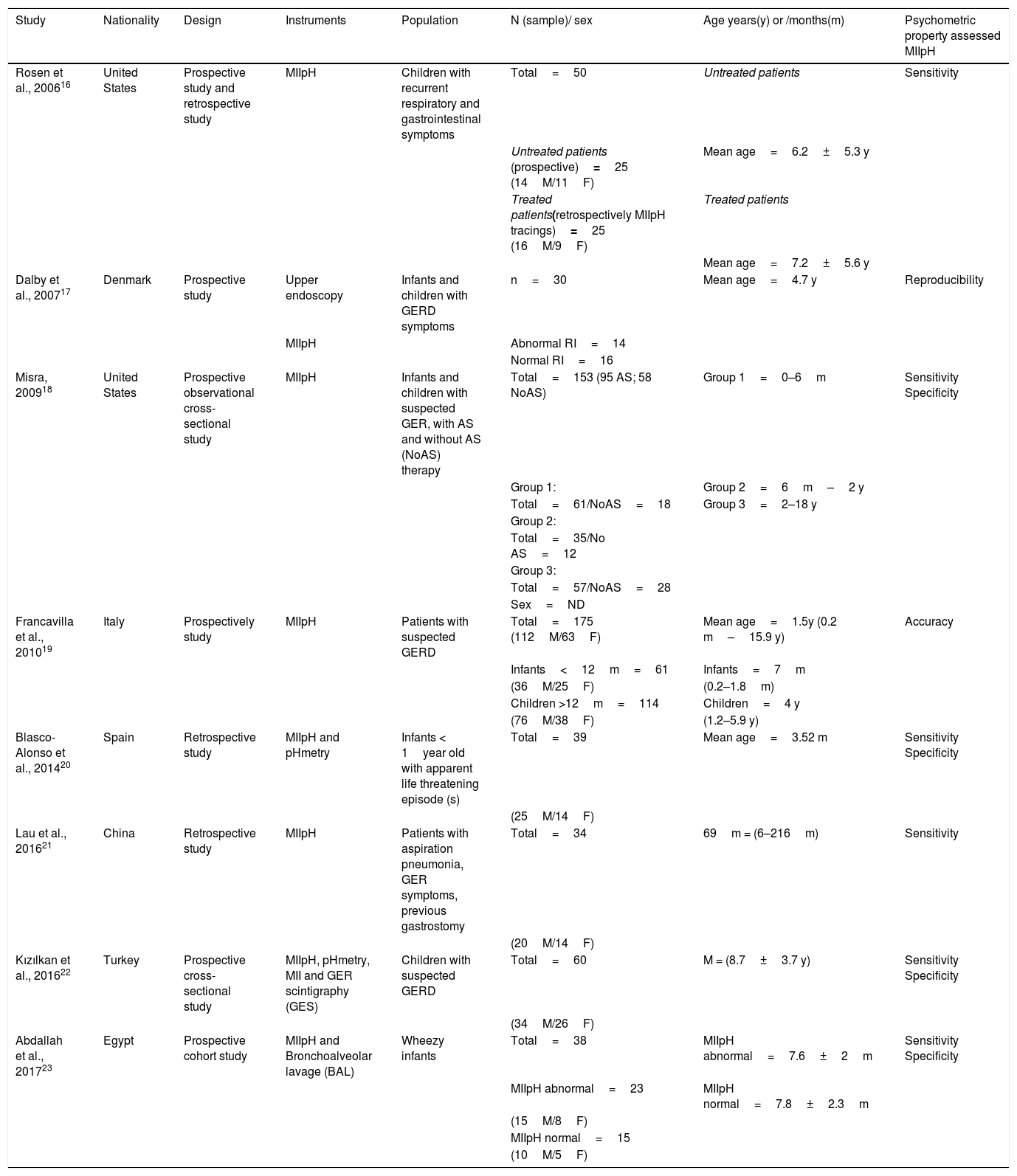
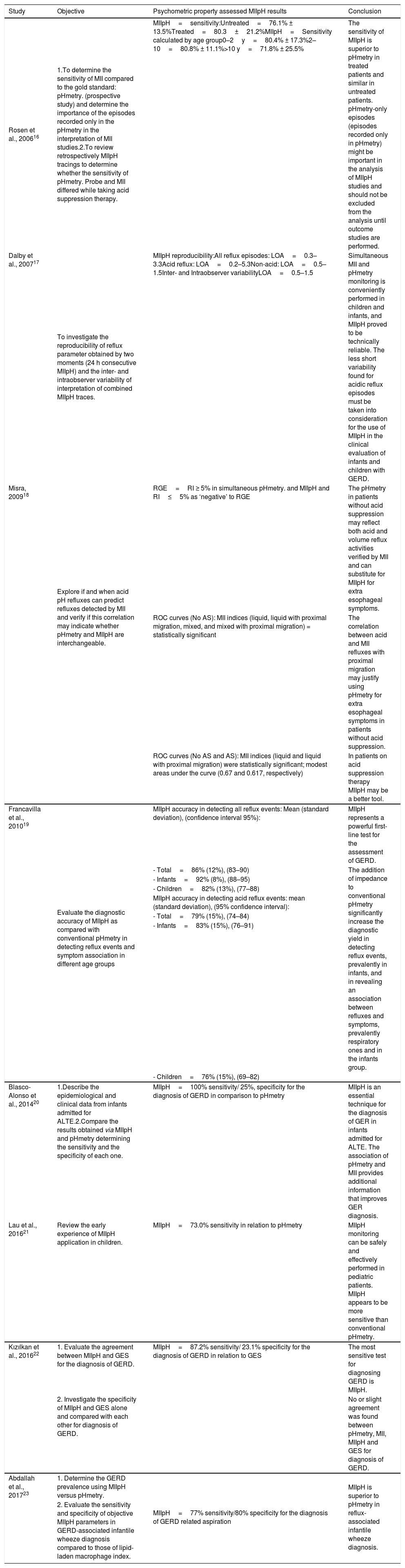
According to the PRISMA recommendations,15 two evaluators performed the extraction and analysis of the selected articles. Data on authorship, year of publication, nationality, study design, population studied, sample size, gender, age group, and PP were extracted from the selected studies16–23 (Table 2). Table 3 presents the objectives of these studies,16–23 the results of the MIIpH in relation to the psychometric property evaluated, and its conclusion.
Description of the studies.
| Study | Nationality | Design | Instruments | Population | N (sample)/ sex | Age years(y) or /months(m) | Psychometric property assessed MIIpH |
|---|---|---|---|---|---|---|---|
| Rosen et al., 200616 | United States | Prospective study and retrospective study | MIIpH | Children with recurrent respiratory and gastrointestinal symptoms | Total=50 | Untreated patients | Sensitivity |
| Untreated patients (prospective)=25 (14M/11F) | Mean age=6.2±5.3 y | ||||||
| Treated patients(retrospectively MIIpH tracings)=25 (16M/9F) | Treated patients | ||||||
| Mean age=7.2±5.6 y | |||||||
| Dalby et al., 200717 | Denmark | Prospective study | Upper endoscopy | Infants and children with GERD symptoms | n=30 | Mean age=4.7 y | Reproducibility |
| MIIpH | Abnormal RI=14 | ||||||
| Normal RI=16 | |||||||
| Misra, 200918 | United States | Prospective observational cross-sectional study | MIIpH | Infants and children with suspected GER, with AS and without AS (NoAS) therapy | Total=153 (95 AS; 58 NoAS) | Group 1=0–6m | Sensitivity Specificity |
| Group 1: | Group 2=6m–2 y | ||||||
| Total=61/NoAS=18 | Group 3=2–18 y | ||||||
| Group 2: | |||||||
| Total=35/No AS=12 | |||||||
| Group 3: | |||||||
| Total=57/NoAS=28 | |||||||
| Sex=ND | |||||||
| Francavilla et al., 201019 | Italy | Prospectively study | MIIpH | Patients with suspected GERD | Total=175 (112M/63F) | Mean age=1.5y (0.2 m–15.9 y) | Accuracy |
| Infants<12m=61 | Infants=7m | ||||||
| (36M/25F) | (0.2–1.8m) | ||||||
| Children >12m=114 | Children=4 y | ||||||
| (76M/38F) | (1.2–5.9 y) | ||||||
| Blasco-Alonso et al., 201420 | Spain | Retrospective study | MIIpH and pHmetry | Infants < 1year old with apparent life threatening episode (s) | Total=39 | Mean age=3.52 m | Sensitivity Specificity |
| (25M/14F) | |||||||
| Lau et al., 201621 | China | Retrospective study | MIIpH | Patients with aspiration pneumonia, GER symptoms, previous gastrostomy | Total=34 | 69m = (6–216m) | Sensitivity |
| (20M/14F) | |||||||
| Kızılkan et al., 201622 | Turkey | Prospective cross-sectional study | MIIpH, pHmetry, MII and GER scintigraphy (GES) | Children with suspected GERD | Total=60 | M = (8.7±3.7 y) | Sensitivity Specificity |
| (34M/26F) | |||||||
| Abdallah et al., 201723 | Egypt | Prospective cohort study | MIIpH and Bronchoalveolar lavage (BAL) | Wheezy infants | Total=38 | MIIpH abnormal=7.6±2m | Sensitivity Specificity |
| MIIpH abnormal=23 | MIIpH normal=7.8±2.3m | ||||||
| (15M/8F) | |||||||
| MIIpH normal=15 | |||||||
| (10M/5F) |
AS, acid suppression; BAL, bronchoalveolar lavage; F, female; GER, gastroesophageal reflux; GERD, gastroesophageal reflux disease; GES, GER scintigraphy; M, male; MIIpH, multiple channel intraluminal impedance and pH monitoring; ND, not described; No AS, No acid suppression; RI, reflux index.
Evaluation of the studies.
| Study | Objective | Psychometric property assessed MIIpH results | Conclusion |
|---|---|---|---|
| Rosen et al., 200616 | 1.To determine the sensitivity of MII compared to the gold standard: pHmetry. (prospective study) and determine the importance of the episodes recorded only in the pHmetry in the interpretation of MII studies.2.To review retrospectively MIIpH tracings to determine whether the sensitivity of pHmetry. Probe and MII differed while taking acid suppression therapy. | MIIpH=sensitivity:Untreated=76.1% ± 13.5%Treated=80.3±21.2%MIIpH=Sensitivity calculated by age group0–2y=80.4% ± 17.3%2–10=80.8% ± 11.1%>10 y=71.8% ± 25.5% | The sensitivity of MIIpH is superior to pHmetry in treated patients and similar in untreated patients. pHmetry-only episodes (episodes recorded only in pHmetry) might be important in the analysis of MIIpH studies and should not be excluded from the analysis until outcome studies are performed. |
| Dalby et al., 200717 | To investigate the reproducibility of reflux parameter obtained by two moments (24 h consecutive MIIpH) and the inter- and intraobserver variability of interpretation of combined MIIpH traces. | MIIpH reproducibility:All reflux episodes: LOA=0.3–3.3Acid reflux: LOA=0.2–5.3Non-acid: LOA=0.5–1.5Inter- and Intraobserver variabilityLOA=0.5–1.5 | Simultaneous MII and pHmetry monitoring is conveniently performed in children and infants, and MIIpH proved to be technically reliable. The less short variability found for acidic reflux episodes must be taken into consideration for the use of MIIpH in the clinical evaluation of infants and children with GERD. |
| Misra, 200918 | Explore if and when acid pH refluxes can predict refluxes detected by MII and verify if this correlation may indicate whether pHmetry and MIIpH are interchangeable. | RGE=RI ≥ 5% in simultaneous pHmetry. and MIIpH and RI≤5% as ‘negative’ to RGE | The pHmetry in patients without acid suppression may reflect both acid and volume reflux activities verified by MII and can substitute for MIIpH for extra esophageal symptoms. |
| ROC curves (No AS): MII indices (liquid, liquid with proximal migration, mixed, and mixed with proximal migration) = statistically significant | The correlation between acid and MII refluxes with proximal migration may justify using pHmetry for extra esophageal symptoms in patients without acid suppression. | ||
| ROC curves (No AS and AS): MII indices (liquid and liquid with proximal migration) were statistically significant; modest areas under the curve (0.67 and 0.617, respectively) | In patients on acid suppression therapy MIIpH may be a better tool. | ||
| Francavilla et al., 201019 | Evaluate the diagnostic accuracy of MIIpH as compared with conventional pHmetry in detecting reflux events and symptom association in different age groups | MIIpH accuracy in detecting all reflux events: Mean (standard deviation), (confidence interval 95%): | MIIpH represents a powerful first-line test for the assessment of GERD. |
| - Total=86% (12%), (83–90) | The addition of impedance to conventional pHmetry significantly increase the diagnostic yield in detecting reflux events, prevalently in infants, and in revealing an association between refluxes and symptoms, prevalently respiratory ones and in the infants group. | ||
| - Infants=92% (8%), (88–95) | |||
| - Children=82% (13%), (77–88) | |||
| MIIpH accuracy in detecting acid reflux events: mean (standard deviation), (95% confidence interval): | |||
| - Total=79% (15%), (74–84) | |||
| - Infants=83% (15%), (76–91) | |||
| - Children=76% (15%), (69–82) | |||
| Blasco-Alonso et al., 201420 | 1.Describe the epidemiological and clinical data from infants admitted for ALTE.2.Compare the results obtained via MIIpH and pHmetry determining the sensitivity and the specificity of each one. | MIIpH=100% sensitivity/ 25%, specificity for the diagnosis of GERD in comparison to pHmetry | MIIpH is an essential technique for the diagnosis of GER in infants admitted for ALTE. The association of pHmetry and MII provides additional information that improves GER diagnosis. |
| Lau et al., 201621 | Review the early experience of MIIpH application in children. | MIIpH=73.0% sensitivity in relation to pHmetry | MIIpH monitoring can be safely and effectively performed in pediatric patients. MIIpH appears to be more sensitive than conventional pHmetry. |
| Kızılkan et al., 201622 | 1. Evaluate the agreement between MIIpH and GES for the diagnosis of GERD. | MIIpH=87.2% sensitivity/ 23.1% specificity for the diagnosis of GERD in relation to GES | The most sensitive test for diagnosing GERD is MIIpH. |
| 2. Investigate the specificity of MIIpH and GES alone and compared with each other for diagnosis of GERD. | No or slight agreement was found between pHmetry, MII, MIIpH and GES for diagnosis of GERD. | ||
| Abdallah et al., 201723 | 1. Determine the GERD prevalence using MIIpH versus pHmetry. | MIIpH=77% sensitivity/80% specificity for the diagnosis of GERD related aspiration | MIIpH is superior to pHmetry in reflux-associated infantile wheeze diagnosis. |
| 2. Evaluate the sensitivity and specificity of objective MIIpH parameters in GERD-associated infantile wheeze diagnosis compared to those of lipid-laden macrophage index. |
ALTE, apparent life threatening episodes; AS, acid suppression; F, female; GER, gastroesophageal reflux; GERD, gastroesophageal reflux disease; GES, GER scintigraphy; h, hour; LOA, lower and upper limits of agreement; M, male; MII, multichannel esophageal intraluminal impedance testing; MIIpH, multichannel intraluminal impedance and pH monitoring; No AS, No acid suppression; RI, reflux index.
The methodological evaluation of the studies was performed by two independent evaluators, using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) criteria.24 The QUADAS-2 is structured in four key domains: patient selection, index test, reference pattern, and flow and timing. Each domain was assessed for risk of bias and the first three domains were also evaluated in terms of applicability concerns. Signaling questions are included to help judge the risk of bias such as “low risk of bias” or “high risk of bias.” The items are described as: “yes,” “no,” and “not clear.” In case of divergence, a third evaluator was consulted.
ResultsSearch and selectionRegarding the selection of articles, 539 titles were identified in the databases; after the removal of duplicates, 418 were analyzed during the selection process. Two additional articles (obtained through manual search) were added, resulting in 420 titles for evaluation. Subsequently, 100 were removed and 320 abstracts were revised according to the pre-established inclusion and exclusion criteria (Table 1). Thus, 237 articles were eligible for reading in full. As a final result, eight papers were considered for analysis (Fig. 1).
Characteristics of studies and detailing the psychometric properties
The characteristics of the selected studies are described in Table 2, in which different nationalities were observed: two Americans,16,18 three Europeans,17,19,20 one Asian,21 one Euro-Asian,22 and one African.23 The oldest study found was by Rosen et al.16 in 2006. Regarding study designs, most of them were prospective.17–19,22,23 Among the main PP, sensitivity was verified in six studies,16,18,20–23 in which four associated specificity assessment.18–20,22,23 Variances of accuracy19 and reproducibility17 were also noted.
The analyzed studies demonstrated sensitivity values considered to be high: 76.1% to 80.3% in Rosen et al.,16 100% in Blasco-Alonso et al.,20 73% in Lau et al.,21 87.2% in Kilzilkan,22 and 77% in Abdallah,23 whereas specificity values were of 23% in Kilzilkan et al.,22 25% in Blasco-Alonso et al.,20 and only Abdallah et al.23 presented values of 80%.
Evaluation of methodological qualityIn the present review, methodological quality was assessed through risk of bias and concern regarding applicability (Fig. 2).
.")
Considering risk of bias, the results demonstrated regarding the domain “Flow and Timing”: 63% as low risk, 25% high, and 13% unclear. In relation to the "Reference Standard" and “Index Test” domains, 100% of the values were considered low risk. Moreover, in the “Patient Selection” domain the proportion was 50% for low risk and 50% unclear (Fig. 2B). Regarding concern about applicability, the “Reference Standard” domain presented 100% unclear, the “Index Test” domain resulted in 100% high concern, and the “Patient Selection” domain presented 100% low concern (Fig. 3A,B).
Discussion
The investigation regarding diagnosis of GERD continues to be the subject of numerous recent studies, as well as the use of different tools for this purpose.1–5,7
The PP are as follows: verification of internal consistency, validity, reproducibility, responsiveness, feasibility, sensitivity, and specificity.12,14,25–27 However, the concern with applicability in a safe, reliable, and standardized way is seldom discussed in the literature.
Findings of the present systematic search state that the PP are still not presented in a clear way and are not included in most of the studies related to the diagnosis through specific instruments. The statements about GER and GERD demonstrate different situations and questions. Among them is the use of diagnostic instruments such as pHmetry, which despite having been considered a gold standard for a long time, can only evaluate episodes of acid reflux and does not assess immediate postprandial GER or characterize the physicochemical properties of GER, not allowing an accurate swallowing investigation.6,7,9,28
As a more complete alternative to evaluate the different aspects of GERD, the MIIpH is an examination based on the association of pHmetry and the evaluation of electric potential of esophageal contents by multiple channels, which allows characterizing acid and non-acidic episodes, in addition to assessing retrograde or anterograde “bolus” flow, physical-chemical properties, and association to symptoms.4,5,28,29
As previously mentioned, the evaluation of the PP of a diagnostic test is useful in order to assure the quality of its application.12,14 The search for PP was performed with the objective of obtaining safety in the use of the MIIpH with more judicious, organized, and better-elucidated parameters.
In the analyzed articles the PP of sensitivity was recorded, which is the probability of a test identifying among sick individuals who actually has the disease16,18,20–23,30; specificity, which represents the ability of a test to identify among the normal individuals those who do not really have the disease18,20,22,23,30; accuracy, which refers to the degree to which the test is able to determine the true value of what is being measured19,30; and, finally, reproducibility, which has the purpose of verifying the consistency of results when the exam is repeated.17,30
The PP most used in the studies were sensitivity and specificity, as shown in Blasco-Alonso et al.20; Kızılkan et al.,22 and Abdallah et al.23 These properties were used to compare MIIpH with other diagnostic instruments regarding GERD, such as bronchoalveolar lavage (BAL),23 GER scintigraphy (GES),22 and pHmetry,20 in which sensitivity values of around 77% to 100% and specificity varying from 23.1% to 80% for MIIpH were found.20,22 The authors concluded that MIIpH alone is a very sensitive and very specific method for the diagnosis of GERD and its complications.
In cases of atypical GERD symptoms, in which respiratory manifestation was the only or most important event, MIIpH also showed high sensitivity for the diagnosis of GERD, as can be observed in the results obtained by Abdallah et al. (77%),23 Lau et al. (73.0%),21 and Blasco-Alonso et al. (100%).20
Sensitivity alone was evaluated in the studies of Lau et al.21 and Rosen et al.16 In both studies, most of the sample analysis was retrospective and MIIpH was compared with pHmetry. Sensitivity values of MIIpH ranged from 73% to 80.3%, which demonstrated better sensitivity of the MIIpH regarding diagnosis of GERD in children.
These high sensitivity and safety values of MIIpH regarding diagnosis of GERD in children were also found by other authors. Safe et al.31 reviewed all MIIpH tests over a six-year period at Sydney Children's Hospital and found that the use of MIIpH resulted in 50.4% higher diagnoses of GERD in comparison to the isolated pHmetry, regardless of the use of antireflux medications. Moreover, the sensitivity value for diagnosis of children who were taking medication was 92.94%.
Wenzel, in 2003,32 presented a retrospective study that simultaneously analyzed the MIIpH, isolated pHmetry, and polysomnography tests in 22 infants and children who had apnea, aspiration, and respiratory disorders. The author concluded that the pHmetry associated with impedancemetry proved to be a valuable tool to diagnose GERD regardless of its pH value and association of GER with symptoms, as well as the possibility of evaluating the composition of the refluxate, and its movement, duration, and esophageal clearance. In 2014 Mousa et al.29 published an analysis of MIIpH tracings in 117 children with GER with normal levels of acid and no association of GER episodes with symptoms. The authors concluded that these values can be used as comparison references to identify infants and/or children who may be at risk of developing clinical manifestations associated with GERD due to abnormal GERD patterns.
More specifically, in the work of Rosen et al. in 2006,16 two procedures were carried out. Initially, a prospective study where MIIpH was performed in infants and children who discontinued antacid medication 48h previously to the test, to assess sensitivity of pHmetry and MIIpH. This practice is common in the application routine of the MIIpH29 and they observed that the sensitivity was similar, approximately 80%, in the two tests: (pHmetry=80.6%±18.2% and MIIpH=76.1%±13.5%). In the sequence, they performed a retrospective evaluation of MIIpH exams with the same age group and the group who used medication: proton pump inhibitor, H2 blocker, or both. The sensitivity of MIIpH remained constant while pHmetry fell to approximately 40% (pHmetry=47.2%±36.0% and MIIpH=80.3%±21.1%). This decrease in the sensitivity of pHmetry may be related to the diet, which in this age group, is predominantly of milk and consequently low acidic.
Another psychometric property found in publications was the accuracy of MIIpH in relation to isolated pHmetry in one group of infants (<12months) and another group of children (>12months).19 The findings showed that the mean accuracy for both groups was higher for MIIpH, considering that it was 86% (83–90% CI) for the total number of refluxes and 79% (74–84%) for the total number of acid refluxes, which, according to the authors, demonstrated that MIIpH is a powerful tool for GERD assessment.19
Regarding the reproducibility variable, the prospective study of Dalby et al. in 200717 was the only one that conducted the monitoring in two periods of 24 consecutive hours. The evaluation consisted of verifying all episodes of GER, acid and non-acid GER, and intra- and interobserver variability in order to analyze the results. The lower and upper limit values of approval (LOA) for these parameters made it possible to conclude that the simultaneous evaluation of MIIpH and pHmetry is a very reliable technique in children and infants. Moreover, the smaller variability among the results is due to the use of MIIpH.
In the present review some parameters related to psychometric properties were verified; however, only sensitivity and specificity were reported. Moreover, accuracy and reproducibility were each mentioned in one article. No studies were found regarding results of the response to treatment using MIIpH.
Although the studies included in this review present individuals with ages ranging from birth to 18 years, the analyses in some studies were carried out in different age groups. In pediatrics, no studies have been validated in healthy children in all different age groups.
In the final analysis, it was pointed out that the sensitivity variable was the most commonly used in all analyzed articles, being able to express and guarantee the importance of MIIpH in the diagnosis of GERD in infants and children. Sensitivity is more related to characteristics of the assessment instrument structure and represents an important issue to be investigated in longitudinal studies,12 since it reflects the ability to truly identify the disease among sick individuals.
Regarding the assessment of the methodological quality of the studies, low risk of bias was observed in all domains, above 50%, reaching 100% low risk for the “Index Test” and “Reference Standard” domains. There was concern about applicability of 100% regarding the “Index test” domain.
ConclusionThe evaluation of PP in studies that used instruments for diagnosing GERD showed that the interest in this context is still undervalued. Since few studies have verified these PP, some questions about clinical applicability still remain. In this review, it was verified that MIIpH is a safe and effective tool, and presents higher sensitivity values than the pHmetry regarding the diagnosis of GERD.
Conflicts of interestThe authors declare no conflicts of interest.
MEDLINE (Ovid)
1 Infant, Newborn/
2 Infant/
3 Child/
4 child*.mp.
5 Child, Preschool/
6 Pediatrics/
7 Adolescent/
8 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7
9 esophageal reflux.mp.
10 Gastroesophageal Reflux/
11 gastro-esophageal reflux.mp.
12. gastro esophageal reflux.mp.
13 GER.mp.
14 GERD.mp.
15 gastro-oesophageal reflux.mp.
16 gastro oesophageal reflux.mp.
17 gastric acid reflux.mp.
18 9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17
19 Multichannel Intraluminal Impedance-pH.mp.
20 MII-pH.mp.
21 impedance-pH Monitoring.mp.
22 esophageal Impedance Monitoring.mp.
23 19 OR 20 OR 21 OR 22
24 8 AND 18 AND 23
Embase
(newborn OR infant OR pediatrics OR ‘preschool child’ OR adolescent OR child AND ‘gastroesophageal reflux’ OR (esophageal AND reflux) OR (‘gastro esophageal’ AND reflux) OR (gastro AND esophageal AND reflux) OR ger OR gerd OR (‘gastro oesophageal’ AND reflux) OR (gastro AND oesophageal AND reflux) OR (gastric AND acid AND reflux)) AND multichannel AND intraluminal AND impedance OR ‘MII ph’ OR (‘impedance ph’ AND monitoring) OR (esophageal AND impedance AND monitoring)) AND ([controlled clinical trial]/lim OR [randomized controlled trial]/lim)
Scopus
(newborn OR infant OR child* OR preschool OR pediatrics OR adolescent) AND (esophageal reflux OR gastroesophageal reflux OR gastro esophageal reflux OR gastro-esophageal reflux OR GER OR GERD OR gastro-oesophageal reflux OR gastroesophageal reflux OR gastric acid reflux) AND (multichannel intraluminal impedance-pH OR MII-pH OR impedance-pH monitoring OR esophageal impedance monitoring) AND (LIMIT-TO LANGUAGE, “English”) OR LIMIT-TO (LANGUAGE, “Spanish”) OR LIMIT-TO (LANGUAGE, “Portuguese”)
Please cite this article as: Gonçalves ES, Assumpção MS, Servidoni MF, Lomazi EA, Ribeiro JD. Multichannel intraluminal impedance-pH and psychometric properties in gastroesophageal reflux: systematic review. J Pediatr (Rio J). 2020;96:673–85.





