
To describe the association of maternal and neonatal characteristics with the adherence status to the in-hospital stages of the Kangaroo-Mother Care Method – KMC (full, partial, and no-adherence).
MethodsRetrospective cohort study including infants < 2500 g admitted to a reference maternity hospital for the KMC in Rio de Janeiro from January to December 2018. Maternal and neonatal characteristics were distributed according to the adherence status to the KMC in-hospital stages. In the first stage, KMC is performed in Neonatal Intensive Care Unit and Conventional Neonatal Intermediate Care Unit. The second stage is completed in Kangaroo Neonatal Intermediate Care Unit. Multinomial multiple regression was performed with KMC adherence as a three-category dependent variable and maternal and neonatal characteristics as independent variables.
ResultsOf 166 dyads, 102 (61.5%) participated in two stages. Those who did not participate in any stage (n = 52; 31.3%) had a lower level of education, a higher frequency of adverse conditions, and were more often single mothers; mothers who participated only in the first stage (n = 12; 7,2%) had more premature and sick infants. Conditions associated with adherence to the two stages compared to no adherence were: high school education (OR = 2.34; 95% CI = 1.08-5.07), presence of a partner (OR = 3.82; 95% CI = 1.7-8.61), no adverse conditions (OR = 3.54; 95% CI = 1.59-7.89) and no neonatal resuscitation (OR = 2.73; 95% CI = 1.22-6.1).
ConclusionsThe study identified maternal and neonatal conditions associated with adherence status to the KMC. The results suggest opportunities to improve adherence.
Worldwide, 15% to 20% of all births are low birth weight (LBW), representing more than twenty million births annually. LBW, defined as weight at birth less than 2500g, is a global public health problem. It is a major predictor of mortality and morbidity and is associated with both short- and long-term consequences related to neurodevelopment and increased risk for cardiovascular and metabolic diseases.1 Interventions to reduce morbidity and mortality in this population are fundamental.
The Kangaroo-Mother Care Method (KMC), conceived in Colombia in 1979 to deal with overcrowding and lack of resources, consisted of skin-to-skin contact with the mother in the supine position, allowing the infant to stay out of the incubator and earlier discharge.2 In 2003, the World Health Organization (WHO) recognized this method as a safe, effective, and low-cost alternative to conventional care for low-birth-weight infants, being suggested as standard care, even in developed countries. The WHO defined the KMC as early, continuous, and prolonged skin-to-skin contact between the baby and his mother, exclusive breastfeeding whenever possible, and early discharge with close follow-up.3 Robust scientific evidence has proven its benefits when compared to conventional care, such as lower mortality decreased risk of neonatal sepsis, hypothermia, hypoglycemia, and rehospitalization; increased exclusive breastfeeding rates and mother-infant bond; decreased physiological responses to pain; better growth, motor and cognitive development.4-8
In Brazil, the proposal is more comprehensive. It involves active participation of the father, welcoming to the family, humanization, individualization of care, and control of the environment, conducted in three stages (two in-hospitals and one at home). In 2000, it was officially included in the Government Policy on Public Health through the “Norm for implementing the Kangaroo Method.” The Ministry of Health selected National Reference Centers and coordinated several strategies to disseminate the method and training of a multidisciplinary team.9-12
Despite the proven benefits of the KMC and the worldwide dissemination of knowledge about the method, there are still many barriers to its universal implementation.13-17 Although being a national health policy in Brazil, participation in KMC is low.18,19 Few Brazilian studies address the association between maternal and neonatal characteristics and adherence to the KMC. Detecting these factors can help develop public policies to improve adherence to the method and neonatal outcomes.
This study aims to describe the characteristics of mother-infants dyads stratified in three groups according to full, partial, and no adherence to the in-hospital stages of KMC; and to evaluate the association between maternal and neonatal conditions and the adherence status to KMC.
MethodsA retrospective cohort study included mother/LBW infant dyads admitted to a neonatal unit of a public maternity hospital in Rio de Janeiro, a reference center for the KMC, from January to December 2018.
In this maternity hospital and other Brazilian public institutions, the KMC is implemented in three stages, as defined and regulated in documents from the Ministry of Health.11,12,20 This study evaluated only the first and second in-hospital KMC stages. The first stage begins during prenatal care for pregnant women who need specialized care. It extends to the delivery room and newborns' hospitalization in the Neonatal Intensive Care Unit (NICU) and the Conventional Neonatal Intermediate Care Unit (NItCU-Co), where the mother initiates skin-to-skin contact intermittently but does not remain hospitalized with her baby. The second stage is performed in the Kangaroo Neonatal Intermediate Care Unit (NItCU-K), where the mother remains hospitalized with her baby full-time. In the second stage, all care processes started in the first stage are kept, with particular attention to breastfeeding. The infant stays with his mother in the kangaroo position as long as possible.
All dyads of mother and infants with a birth weight below 2500g who were admitted to the NICU, NItCU-Co, or NitCU-K during the study period were selected. Infants with major congenital malformations or genetic syndromes and those discharged or who died less than seven days of hospitalization were excluded. Data from the participants were extracted from medical records, entered in the REDCAP data bank (Vanderbilt University, Nashville, TN, USA), and exported to Excel spreadsheets (Microsoft Corporation, USA).
The participant dyads were grouped according to the KMC adherence: group 1 (Full adherence) – adherence to the two in-hospital KMC stages (mother-infants dyads who participated in the first stage at NICU and/or NItCU-Co, and in the second stage at NitCU-K); group 2 (No adherence) – no adherence to any in-hospital stage (mothers did not perform skin-to-skin contact with their babies during hospitalization); group 3 (Partial adherence) – adherence only to the first stage (mothers performed skin-to-skin contact with their babies at NICU and/or NItCU-Co intermittently, but they did not remain full-time in NitCU-K).
Sociodemographic and clinical maternal variables (age, race, education, marital status, occupation, adverse conditions, prenatal visits, parity, gestational complications, antenatal corticosteroids, delivery mode, complications at birth) and neonatal variables (gender, twin birth, gestational age, birth weight, resuscitation at delivery room, Apgar at 5 minutes and late neonatal complication), were distributed according to the three groups of adherence.
Descriptive statistics were presented for maternal and neonatal characteristics according to the adherence status to in-hospital stages of KMC stratified into three categories (full, partial, and no adherence). Categorical variables were presented as proportions, and numerical variables were presented as medians and interquartile ranges (IQR). Statistical tests were performed to compare the three categories of adherence (Kruskal Wallis for comparison of medians and Chi-square for comparison of proportions). For the variables that showed significance in these first tests, the authors also performed multiple comparison tests (Nemenyi test when the Kruskal Wallis was applied) and a pair of proportions tests (chi-square) to define between which groups there was a difference. To identify factors associated with adherence to the KMC method, a multinomial multiple regression was developed comparing mothers who did not adhere to the KMC method as a reference (group2) to those with partial (group 3) and full (group 1) adherence (dependent variable with three categories) in relation to the maternal and neonatal characteristics (independent variables) that showed statistical significance in bivariate associations (p < 0.05). A significance level of 5% was adopted for all analyses, using the statistical program R (R Core Team, Vienna, Austria). Multiple logistic regressions were performed, comparing each pair of the dependent variable (group 1 x group 2, group 1 x group 3 and group 2 x group 3).
The study was approved by the Research Ethics Committee of the Municipal Health Secretary of Rio de Janeiro under the number 3.593.196.
ResultsOf 6046 live births in the study unit in 2018, 587 (9.7%) had birth weight < 2500 g. Of these, 223 were admitted to the neonatal unit, but 57 were excluded due to the following reasons: 26 were discharged from the neonatal unit to the rooming-in unit within less than seven days, four had genetic syndromes, 10 had major congenital malformations, and 17 died within less than seven days of life. A total of 166 mother-infant dyads were included in the study and stratified into three groups according to the adherence status to the two in-hospital stages of KMC: G1(full adherence) – adherence to two stages (n = 102); G2 – no adherence (n = 52), and G3 (partial adherence) - adherence only to the first stage (n = 12).
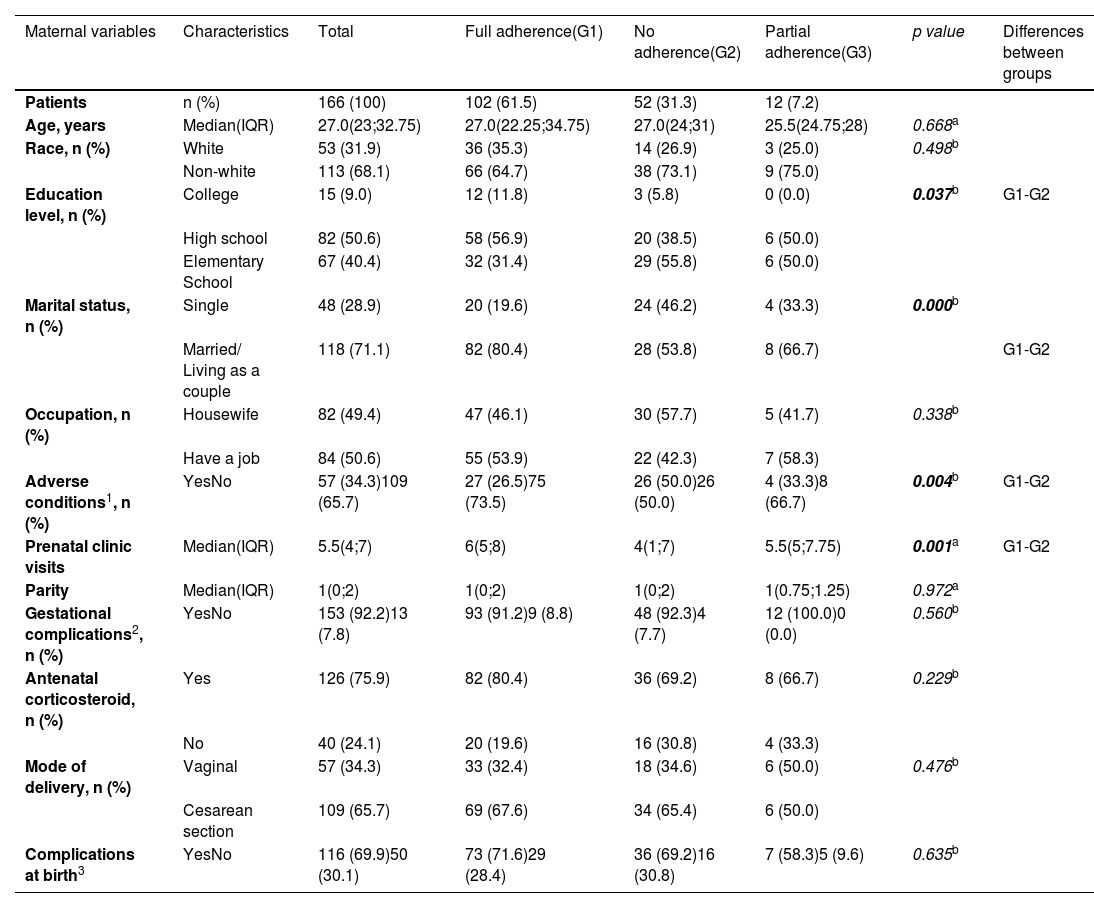
Maternal age was similar in the three groups, with a median of 27 years (IQR 23;32.8). Most mothers declared as non-white race (68.1%), had high school education (50.6%), and had a partner (71.1%). Differences were observed between the full-and no-adherence groups (G1 x G2) for some variables. The no-adherence group (G2) had a greater proportion of single mothers (46.2% x 19.6%) and adverse conditions (50.0% x 26.5%), a smaller proportion of high-level education (5.8 × 11.8), and a lower median number of prenatal visits (4.0 × 6.0). The use of antenatal corticosteroids (75.9%), gestational complications (92.2%), and complications at birth (69.9%) were frequent, without significant differences between the groups. Cesarean section was the most frequent mode of delivery (65.7%) and was similar in the three groups (Table 1).
Maternal sociodemographic, clinical, pregnancy and delivery characteristics, according to adherence status to Kangaroo-mother care method.
| Maternal variables | Characteristics | Total | Full adherence(G1) | No adherence(G2) | Partial adherence(G3) | p value | Differences between groups |
|---|---|---|---|---|---|---|---|
| Patients | n (%) | 166 (100) | 102 (61.5) | 52 (31.3) | 12 (7.2) | ||
| Age, years | Median(IQR) | 27.0(23;32.75) | 27.0(22.25;34.75) | 27.0(24;31) | 25.5(24.75;28) | 0.668a | |
| Race, n (%) | White | 53 (31.9) | 36 (35.3) | 14 (26.9) | 3 (25.0) | 0.498b | |
| Non-white | 113 (68.1) | 66 (64.7) | 38 (73.1) | 9 (75.0) | |||
| Education level, n (%) | College | 15 (9.0) | 12 (11.8) | 3 (5.8) | 0 (0.0) | 0.037b | G1-G2 |
| High school | 82 (50.6) | 58 (56.9) | 20 (38.5) | 6 (50.0) | |||
| Elementary School | 67 (40.4) | 32 (31.4) | 29 (55.8) | 6 (50.0) | |||
| Marital status, n (%) | Single | 48 (28.9) | 20 (19.6) | 24 (46.2) | 4 (33.3) | 0.000b | |
| Married/ Living as a couple | 118 (71.1) | 82 (80.4) | 28 (53.8) | 8 (66.7) | G1-G2 | ||
| Occupation, n (%) | Housewife | 82 (49.4) | 47 (46.1) | 30 (57.7) | 5 (41.7) | 0.338b | |
| Have a job | 84 (50.6) | 55 (53.9) | 22 (42.3) | 7 (58.3) | |||
| Adverse conditions1, n (%) | YesNo | 57 (34.3)109 (65.7) | 27 (26.5)75 (73.5) | 26 (50.0)26 (50.0) | 4 (33.3)8 (66.7) | 0.004b | G1-G2 |
| Prenatal clinic visits | Median(IQR) | 5.5(4;7) | 6(5;8) | 4(1;7) | 5.5(5;7.75) | 0.001a | G1-G2 |
| Parity | Median(IQR) | 1(0;2) | 1(0;2) | 1(0;2) | 1(0.75;1.25) | 0.972a | |
| Gestational complications2, n (%) | YesNo | 153 (92.2)13 (7.8) | 93 (91.2)9 (8.8) | 48 (92.3)4 (7.7) | 12 (100.0)0 (0.0) | 0.560b | |
| Antenatal corticosteroid, n (%) | Yes | 126 (75.9) | 82 (80.4) | 36 (69.2) | 8 (66.7) | 0.229b | |
| No | 40 (24.1) | 20 (19.6) | 16 (30.8) | 4 (33.3) | |||
| Mode of delivery, n (%) | Vaginal | 57 (34.3) | 33 (32.4) | 18 (34.6) | 6 (50.0) | 0.476b | |
| Cesarean section | 109 (65.7) | 69 (67.6) | 34 (65.4) | 6 (50.0) | |||
| Complications at birth3 | YesNo | 116 (69.9)50 (30.1) | 73 (71.6)29 (28.4) | 36 (69.2)16 (30.8) | 7 (58.3)5 (9.6) | 0.635b |
IQR, Interquartile range.
Adverse condition: underlying disease (chronic hypertension, hypothyroidism, psychiatric disorders, diabetes, asthma, obesity) or violence in childhood or domestic violence or illicit drug use or smoking or alcoholism or homeless.
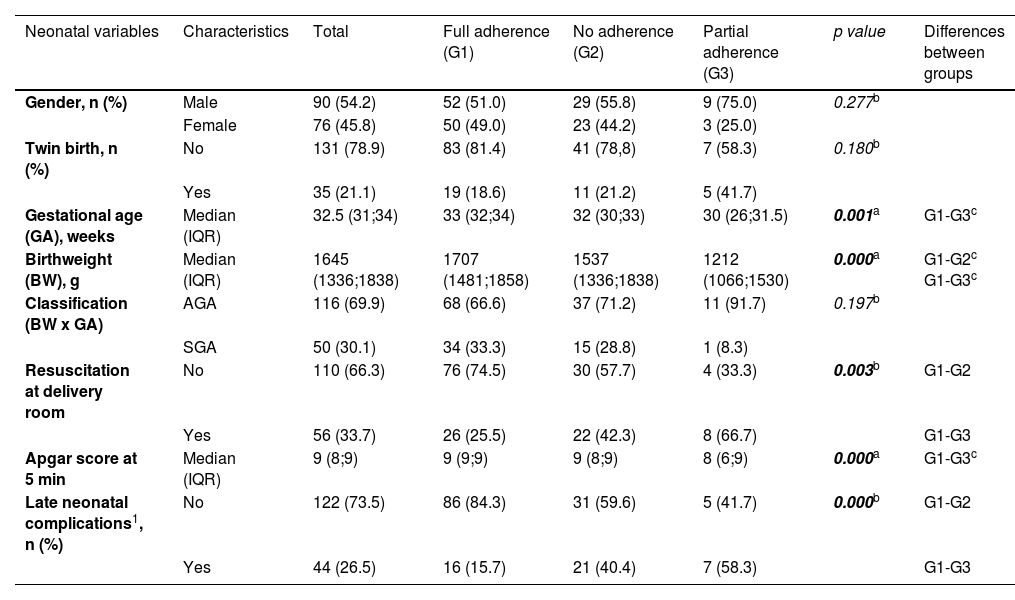
Regarding infants, there was no difference between groups regarding gender or twin birth. Significant differences were observed for gestational age (G1 x G3), birthweight (G1 x G2 and G1 x G3), resuscitation at the delivery room (G1 x G2 and G1 x G3), Apgar at 5 minutes (G1 x G3), late neonatal complications (G1 x G2 and G1 x G3). The partial-adherence group (G3) had the lowest median gestational age (30.0, IQR 26;31.5), birth weight (1212g, IQR 1066;1530g), and Apgar at 5’ (8 [IQR 6-9]), and the greatest proportions of resuscitation at the delivery room (66.7%) and neonatal complications (58.3%) (Table 2).
Neonatal demographic and clinical characteristics, according to adherence status to Kangaroo-mother care method.
| Neonatal variables | Characteristics | Total | Full adherence (G1) | No adherence (G2) | Partial adherence (G3) | p value | Differences between groups |
|---|---|---|---|---|---|---|---|
| Gender, n (%) | Male | 90 (54.2) | 52 (51.0) | 29 (55.8) | 9 (75.0) | 0.277b | |
| Female | 76 (45.8) | 50 (49.0) | 23 (44.2) | 3 (25.0) | |||
| Twin birth, n (%) | No | 131 (78.9) | 83 (81.4) | 41 (78,8) | 7 (58.3) | 0.180b | |
| Yes | 35 (21.1) | 19 (18.6) | 11 (21.2) | 5 (41.7) | |||
| Gestational age (GA), weeks | Median (IQR) | 32.5 (31;34) | 33 (32;34) | 32 (30;33) | 30 (26;31.5) | 0.001a | G1-G3c |
| Birthweight (BW), g | Median (IQR) | 1645 (1336;1838) | 1707 (1481;1858) | 1537 (1336;1838) | 1212 (1066;1530) | 0.000a | G1-G2c G1-G3c |
| Classification (BW x GA) | AGA | 116 (69.9) | 68 (66.6) | 37 (71.2) | 11 (91.7) | 0.197b | |
| SGA | 50 (30.1) | 34 (33.3) | 15 (28.8) | 1 (8.3) | |||
| Resuscitation at delivery room | No | 110 (66.3) | 76 (74.5) | 30 (57.7) | 4 (33.3) | 0.003b | G1-G2 |
| Yes | 56 (33.7) | 26 (25.5) | 22 (42.3) | 8 (66.7) | G1-G3 | ||
| Apgar score at 5 min | Median (IQR) | 9 (8;9) | 9 (9;9) | 9 (8;9) | 8 (6;9) | 0.000a | G1-G3c |
| Late neonatal complications1, n (%) | No | 122 (73.5) | 86 (84.3) | 31 (59.6) | 5 (41.7) | 0.000b | G1-G2 |
| Yes | 44 (26.5) | 16 (15.7) | 21 (40.4) | 7 (58.3) | G1-G3 |
AGA, appropriate for gestational age; SGA, small for gestational age; IQR, Interquartile range.
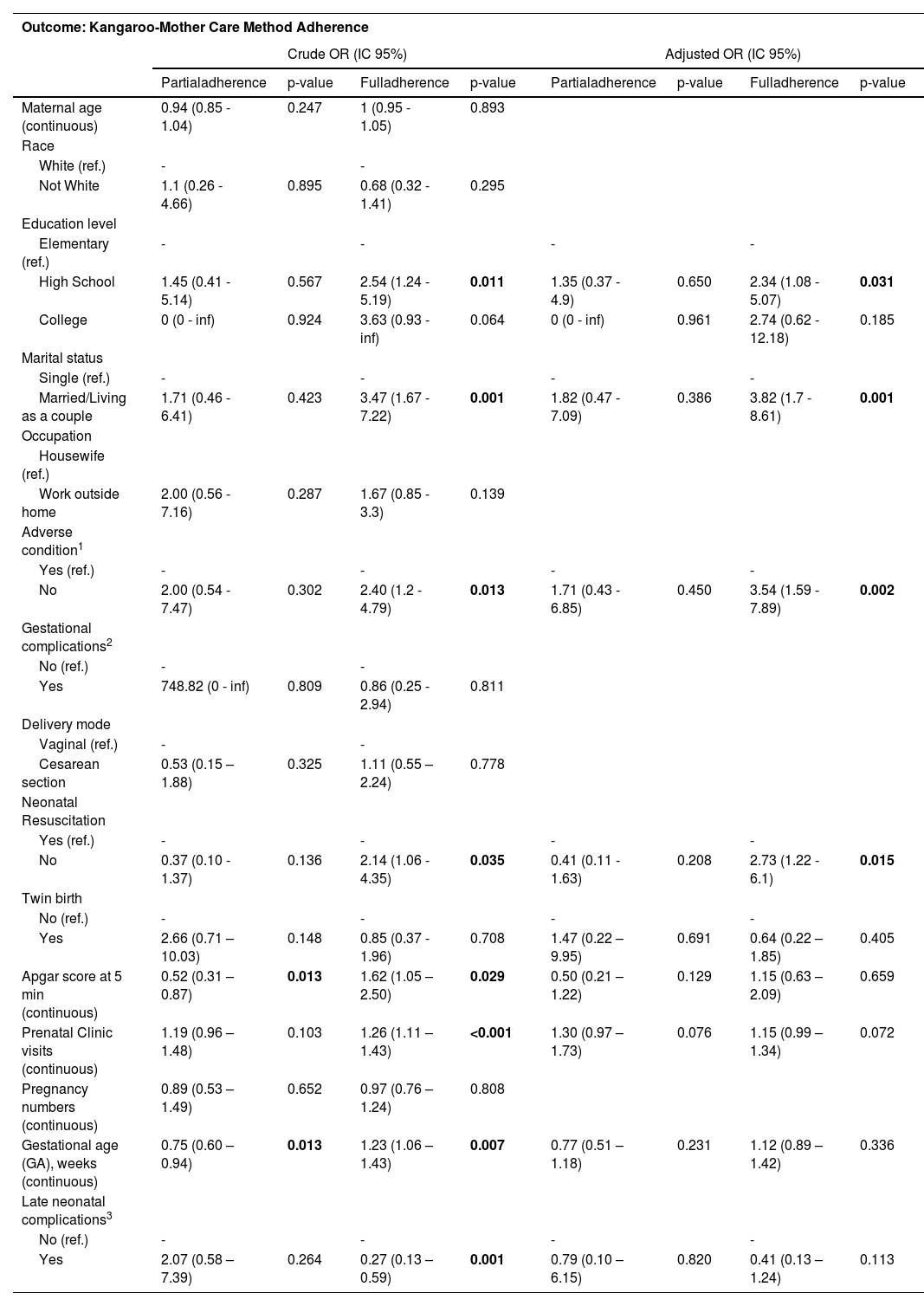
Greater adherence to the two stages of the KMC was associated with the following conditions: mothers with high school education, compared to elementary school (OR 2.34; IC95:1.08 - 5.07); mothers with a partner (married or living as a couple) compared to single mothers (OR 3.82; IC 95: 1.7 - 8.61); mothers without adverse conditions (OR 3.54; IC95: 1.59 - 7.89); and infants with no need of resuscitation in the delivery room (OR 2.73; IC95: 1.22 - 6.1) (Table 3).
Factors associated with adherence status to the Kangaroo-Mother Care method compared to no adherence (ref.)
| Outcome: Kangaroo-Mother Care Method Adherence | ||||||||
|---|---|---|---|---|---|---|---|---|
| Crude OR (IC 95%) | Adjusted OR (IC 95%) | |||||||
| Partialadherence | p-value | Fulladherence | p-value | Partialadherence | p-value | Fulladherence | p-value | |
| Maternal age (continuous) | 0.94 (0.85 - 1.04) | 0.247 | 1 (0.95 - 1.05) | 0.893 | ||||
| Race | ||||||||
| White (ref.) | - | - | ||||||
| Not White | 1.1 (0.26 - 4.66) | 0.895 | 0.68 (0.32 - 1.41) | 0.295 | ||||
| Education level | ||||||||
| Elementary (ref.) | - | - | - | - | ||||
| High School | 1.45 (0.41 - 5.14) | 0.567 | 2.54 (1.24 - 5.19) | 0.011 | 1.35 (0.37 - 4.9) | 0.650 | 2.34 (1.08 - 5.07) | 0.031 |
| College | 0 (0 - inf) | 0.924 | 3.63 (0.93 - inf) | 0.064 | 0 (0 - inf) | 0.961 | 2.74 (0.62 - 12.18) | 0.185 |
| Marital status | ||||||||
| Single (ref.) | - | - | - | - | ||||
| Married/Living as a couple | 1.71 (0.46 - 6.41) | 0.423 | 3.47 (1.67 - 7.22) | 0.001 | 1.82 (0.47 - 7.09) | 0.386 | 3.82 (1.7 - 8.61) | 0.001 |
| Occupation | ||||||||
| Housewife (ref.) | ||||||||
| Work outside home | 2.00 (0.56 - 7.16) | 0.287 | 1.67 (0.85 - 3.3) | 0.139 | ||||
| Adverse condition1 | ||||||||
| Yes (ref.) | - | - | - | - | ||||
| No | 2.00 (0.54 - 7.47) | 0.302 | 2.40 (1.2 - 4.79) | 0.013 | 1.71 (0.43 - 6.85) | 0.450 | 3.54 (1.59 - 7.89) | 0.002 |
| Gestational complications2 | ||||||||
| No (ref.) | - | - | ||||||
| Yes | 748.82 (0 - inf) | 0.809 | 0.86 (0.25 - 2.94) | 0.811 | ||||
| Delivery mode | ||||||||
| Vaginal (ref.) | - | - | ||||||
| Cesarean section | 0.53 (0.15 – 1.88) | 0.325 | 1.11 (0.55 – 2.24) | 0.778 | ||||
| Neonatal Resuscitation | ||||||||
| Yes (ref.) | - | - | - | - | ||||
| No | 0.37 (0.10 - 1.37) | 0.136 | 2.14 (1.06 - 4.35) | 0.035 | 0.41 (0.11 - 1.63) | 0.208 | 2.73 (1.22 - 6.1) | 0.015 |
| Twin birth | ||||||||
| No (ref.) | - | - | - | - | ||||
| Yes | 2.66 (0.71 – 10.03) | 0.148 | 0.85 (0.37 - 1.96) | 0.708 | 1.47 (0.22 – 9.95) | 0.691 | 0.64 (0.22 – 1.85) | 0.405 |
| Apgar score at 5 min (continuous) | 0.52 (0.31 – 0.87) | 0.013 | 1.62 (1.05 – 2.50) | 0.029 | 0.50 (0.21 – 1.22) | 0.129 | 1.15 (0.63 – 2.09) | 0.659 |
| Prenatal Clinic visits (continuous) | 1.19 (0.96 – 1.48) | 0.103 | 1.26 (1.11 – 1.43) | <0.001 | 1.30 (0.97 – 1.73) | 0.076 | 1.15 (0.99 – 1.34) | 0.072 |
| Pregnancy numbers (continuous) | 0.89 (0.53 – 1.49) | 0.652 | 0.97 (0.76 – 1.24) | 0.808 | ||||
| Gestational age (GA), weeks (continuous) | 0.75 (0.60 – 0.94) | 0.013 | 1.23 (1.06 – 1.43) | 0.007 | 0.77 (0.51 – 1.18) | 0.231 | 1.12 (0.89 – 1.42) | 0.336 |
| Late neonatal complications3 | ||||||||
| No (ref.) | - | - | - | - | ||||
| Yes | 2.07 (0.58 – 7.39) | 0.264 | 0.27 (0.13 – 0.59) | 0.001 | 0.79 (0.10 – 6.15) | 0.820 | 0.41 (0.13 – 1.24) | 0.113 |
The final statistical model for multiple regressions was presented in supplementary tables (Tables S1 to S6).
DiscussionThis study, conducted in a reference unit for the KMC, identified maternal and neonatal conditions associated with adherence to KMC, such as education, marital status, adverse maternal conditions before pregnancy, and neonatal resuscitation in the delivery room. The participation rate in the in-hospital stages of KMC was higher than that described in the literature19,20; about 70% of mothers participated in at least one stage and more than 60% in two stages.
Due to the robust evidence regarding the benefits of the KMC in reducing neonatal morbidity and mortality,4-8 the complete implementation of all stages of the method is an indicator of quality in neonatal care. Although the KMC has been a well-defined public health policy with technical standards and guidelines for more than twenty years in Brazil,10-12 many Brazilian neonatal units have not implemented it.19,20
Given the proven impact of this method on neonatal outcomes and its low implementation rate reported in the literature, it is extremely relevant to identify factors that interfere with adherence to the method to adopt strategies that change this scenario. Some international studies have described barriers to implementing the KMC related to the health system, health professionals, and family members.14-18 Still, there is a lack of studies addressing maternal and neonatal aspects related to adherence to the method.
The maternity hospital of the present study has adequate facilities and trained human resources to perform the three stages of KMC, encouraging the mother to stay in the neonatal unit from the time of neonatal admission and promoting the family's participation in neonatal care. Therefore, it does not have the structural and human resources barriers reported in the literature which interfere with the implementation of the method. In this context, this study made it possible to identify other factors related to the mother and the infant, which may be associated with participation in the stages of KMC and, thus, contribute data to adopt public health measures.
Previous qualitative studies identified several maternal barriers to implementing the method. Prolonged hospitalization, fear of caring for a premature infant, responsibilities with other children, inadequate hospital accommodations, lack of family and health team support, lack of knowledge about the benefits of kangaroo care, maternal discomfort with the kangaroo position and breastfeeding were the main reasons mentioned.16,17
In the present study, it was possible to verify that infants who participated in only one stage of KMC were the most premature and had more neonatal complications, suggesting that these neonatal conditions limited the adherence to the two stages of the method. As for those dyads that did not participate in any stage, gestational age, birth weight, and the frequency of neonatal complications were intermediate between those who participated in one or two stages, suggesting that other factors unrelated to the infants might have contributed to no adherence. In fact, in the no-adherence group, some maternal adverse conditions such as illicit drug use, smoking, and alcoholism were more frequent than in the other two groups and showed an association with the adherence status to KMC.
Maternal conditions associated with lower adherence to the two stages of the method were low education level, absence of a partner, and presence of adverse conditions before pregnancy. Maternal schooling may be necessary for understanding the recommendations of professionals and for accessing the information on the benefits of KMC. A family and social support network that offers structural and emotional conditions for the mother to be available and calm to stay in the hospital with the infant and dedicate herself to him is essential. Winnicott highlights the importance of supporting figures for the mother, such as the partner and other family members, to feel better prepared to play her role.21 The absence of a partner may also be associated with a less desired pregnancy. According to Brockington,22 an undesired pregnancy and lack of interaction with the fetus may relate to infant rejection. Maternal adverse conditions such as underlying disease, domestic violence, living on the street, illicit drug use, smoking, and psychiatric disorders may reflect poor physical and mental states to care for the infant, lack of interest in their health, and the infant's health. In this context, mother-infant bonding and adherence to KMC are impaired. These conditions can be identified from prenatal care and indicate the need for special attention for this subgroup of pregnant women.23 A Brazilian cohort study that evaluated maternal factors associated with impairments in the mother-infant relationship showed associations with maternal education, unplanned pregnancy, alcohol consumption during pregnancy, and maternal mental health.24
This study has some limitations. Due to its retrospective design, some maternal variables, such as psychological and other social aspects, probably associated with adherence to KMC, could not be studied. Future prospective studies should consider all these maternal aspects for a more comprehensive analysis of the conditions associated with kangaroo method adherence. The sample size, determined by the study period, allowed only an exploratory analysis of some associations studied, with low precision of some findings. Finally, this study was limited to the in-hospital stages of KMC and did not evaluate the third stage after hospital discharge.
Despite these limitations and given the paucity of data on maternal and neonatal barriers to adherence to KMC, the findings of this study may contribute to a better understanding of these factors and provide subsidies for the elaboration of public policies that support greater participation, improving neonatal care. The use of instruments such as genograms and ecomap can guide measures to strengthen the family, social, and community support network that can contribute to increasing maternal participation in KMC. Policies that provide psychological and social support to families and financial support for maternity hospitals to ensure a hospital structure that allows the mother to stay in the neonatal unit, can be important to increase KMC adherence.




