
To investigate the association between emotional and behavioral difficulties in schoolchildren and maternal educational practices.
MethodsParticipants and Setting: 631 mother-child pairs were evaluated in a poor urban district in Recife, northeastern Brazil. Cross-sectional study carried out between 2013 and 2014. It integrates a prospective cohort study designed to investigate the consequences of intimate partner violence that occurred during pregnancy, postpartum, and seven years after birth for the physical and mental health of women and their children. Maternal educational practices were assessed using the Parent-Child Conflict Tactics Scale (CTSPC - mother-child version) and the child's behavioral and emotional disorders through the Strengths and Difficulties Questionnaire (SDQ) mother-version. The association was estimated through crude and adjusted prevalence ratios, using Poisson regression considering the 95% confidence interval.
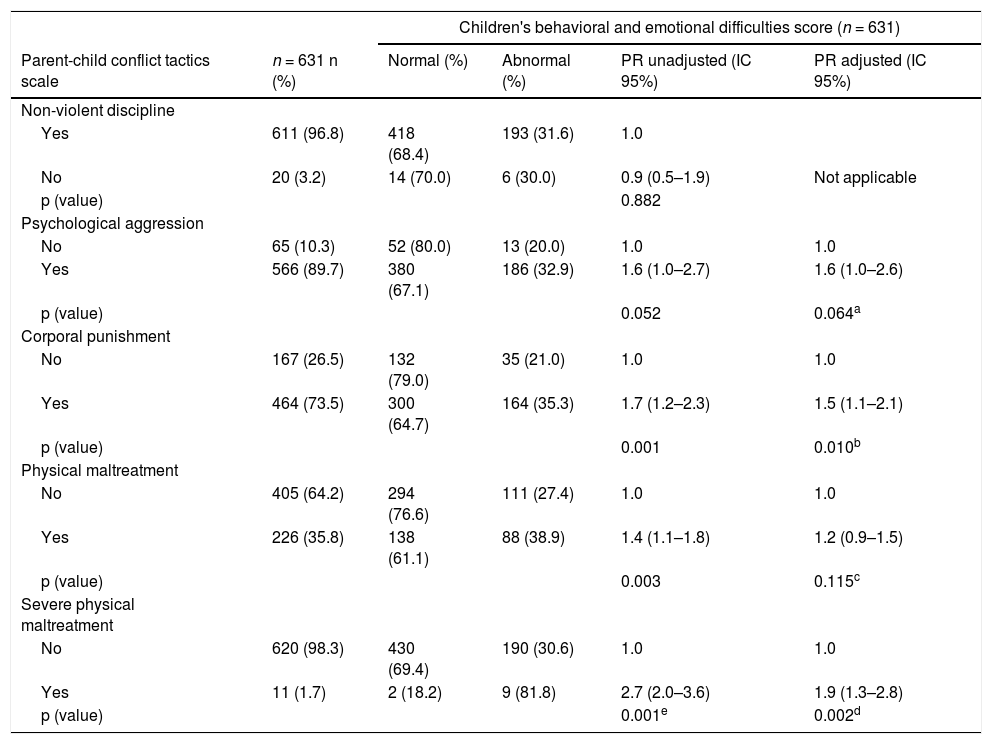
ResultsThe prevalence of violent maternal educational practices was 91.8% (572/631) being 89.7% (566/631) of psychological aggression and 75.6% of physical aggression, subdivided into corporal punishment (73.5%), physical maltreatment (35.8%) and severe physical maltreatment (1.7%). Corporal punishment (Adjusted PR 1.5; CI 95%: 1.1–2.1; p = 0.010) and severe physical maltreatment (Adjusted PR 1.9; CI 95%: 1.3–2.8; p = 0.002) were associated with emotional and behavioral difficulties in schoolchildren.
ConclusionThe high prevalence of violent maternal educational practices, especially corporal punishment and severe physical maltreatment is associated with emotional and behavioral disorders in children. Therefore, it is necessary to interventions that promote parental support and effective use of non-violent discipline in conducting the educational process to establish healthier family relationships and to prevent/mitigate the impact of emotional and behavioral problems in children.
The family is the first social environment in which the child will be exposed to educational practices whose quality will influence the behavioral, emotional, and social development of their children.1
Parental educational practices can act as protective factors (positive educational practices) or risk factors (negative educational practices) for children's mental health, mainly behavioral and emotional problems.2
Positive parenting practices are related to the development of secure attachment, good academic performance, and prosocial behavior, as well as negative parenting practices, which are related to the increase of psychopathology risk among children and adolescents.1
Among the negative educational practices, the use of violence to discipline children stands out. The practice of this “justified violence” is frequent in other countries3 and in Brazil.4 Therefore, the family context that would have the function of protecting their members, especially children, fails to achieve this function, so that, domestic violence against children prevails as a serious social and human rights problem.4
In different countries, there is a high percentage of children who receive corporal punishment from their parents, with the mother being the main perpetrator.3
In a study carried out in southern Brazil,5 despite mothers reporting high percentages of non-violent discipline, it was found that almost half of maternal conflict resolution tactics with their children involve verbal or physical aggression. Verbal aggression are representations of psychological aggression, which can cause fear and psychological suffering. Physical aggression represents corporal punishment that refers to the use of physical force to cause some level experience of pain and discomfort, with the intention of modifying the child's behavior.6
The fact that a violent maternal educational practice is pointed out as the most frequent in several studies,3,5 it may be a consequence of the mother spending more time with her children, being responsible for education and discipline, it is centralizing household chores, or even transferring to children her difficulties and internal conflicts.4
There are several other aspects that contribute to violent maternal educational practice and that can influence children's mental health by altering both the environment and the maternal posture of child care, such as the mother mental health,7 use of legal and illegal drugs,8 poverty,9 maternal history of recent intimate partner violence or in her family of origin or still abuse suffered as a child10 and lack of social support.11
Children exposed to violent maternal educational practices, including psychological aggression and corporal punishment, can be associated with aggression, antisocial behavior, externalizing and internalizing problems, mental health problems, negative relationships with parents, lower cognitive ability, and low self-esteem.12,13
The aim of the study is to investigate the association between maternal educational practices reported by the mothers and mental health disorders of school-age children.
MethodsStudy design and populationCross-sectional study inserted in a cohort conducted in the health district II in the city of Recife, Pernambuco, Brazil between July 2013 and December 2014, with women and children participating in the third stage of a prospective cohort study designed to investigate the consequences of violence committed by the intimate partner against women during pregnancy, in the postpartum period and in the last seven years for women's mental health and the psychosocial development of children born between July 2005 and October 2006.
In the cohort study, three stages of data collection were conducted. The first two occurred in 2005 and 2006. In the first, all 1.120 pregnant women registered in the Family Health Strategy participated with ages between 18 and 49 years and with 31 weeks or more of gestation. In the second, interviews were carried out with 1.057 women until 01 years after delivery, from May to December 2006. Additional information about the study methods is reported in other publications with data from the first and second stages14 and from the third one. Published studies with data from the third stage do not include information on the content of the present study.15-17
From the first to the second stage there was a loss of only 5.7%. From the second to the third stage there was a loss of 39% of the 1057 women who were part of the 2nd stage of the cohort. A comparison of some characteristics of the women who left the study with those who stayed was carried out to assess the magnitude of the selection bias. However, there was no statistical difference between age, race/color, marital status, education, and reports of intimate partner violence between women who took part in this stage of the study and those who did not.15
For this study, 644 women were interviewed, representing 61% of those who participated in the second stage. Between the second and third stages, five women died, 391 were not found due to a change of address and 17 refused to remain in the study. Among the children, four died. Two children who were donated to other families, two who lived with other family members, and five pairs of twins were excluded from the study with their respective mothers. Thus, the study population consisted of 631 pairs of mothers and their children.
In the final sample for analysis, 73.2% of women were over 30 years old, 66.4% earned below the minimum wage, 50.6% had not completed fundamental education, and 82.2% declared non-white ethnicity. Non-white participants were predominately mixed race (brown/pardo/black). The children were between 6 and 9 years old, and 50.9% were female. The majority (64.1%) were attending the second year of elementary school.
All interviews were conducted by women researchers with experience in research on intimate partner violence and violence against children, without the presence of the partner or any child aged two years and older. The women interviewed received a guide with information about the support services available in the city of Recife for women and children in situations of violence.
MeasuresMental health difficulties of childThe Strengths and Difficulties Questionnaire (SDQ) is a brief questionnaire developed by Goodman (1997)18 and validated for the Brazilian context.19 It has been widely used to track behavioral and emotional difficulties. It is available free of charge in 85 languages, including Portuguese (http://www.sdqinfo.org/py/sdqinfo/b3.py?language=Portugueseqz(Brazil). It can be administered to parents and teachers of children and adolescents between 4 and 17 years old and self-administered to adolescents between 11 and 17 years old. It consists of 25 attributes, some positive and others negative, divided into five scales, each containing five items, which generate a total difficult score and scores for prosocial behavior, hyperactivity, emotional problems, behavioral problems, and relationship problems with peers. These child attributes are evaluated with reference to the last six months or the current school year.18
The authors used the total difficulties score of the SDQ. A child with a score of 17 or over was considered to have a high risk of mental health problems. The cut-off points used were: 0–13 to categorize normal children, 14–16 for borderline children, and 17–40 for abnormal children.18 'Borderline' was categorized as 'normal' and then compared to 'abnormal' (positive for child mental health disorders).
Maternal educational practicesThe Parent-Child Conflict Tactics Scale (CTSPC), adopted and validated in Brazil20 is one of the most international instruments used for investigating domestic violence against children.21 It consists of 22 items that investigate domestic violence based on parental educational practice. Three dimensions are evaluated: non-violent discipline (4 items), psychological aggression (5 items), and physical aggression (13 items) being this last one subdivided into three, each one contemplating different acts of severity: corporal punishment (6 items), physical maltreatment (3 items) and severe physical maltreatment (4 items).
For the CTSPC, the items from different scales and different levels of severity are interspersed in a randomly determined order to make the subdivisions less evident to the interviewee.22 Can be answered by the mother regarding her attitudes towards her child asks about the events of the last 12 months, evaluating the frequency of each of the 22 items in three dimensions: it did not happen, it happened once and it happened more than once.22
A positive case of violent maternal educational practice against the child was considered when the affirmative answer of the practice, in the last 12 months of at least one item of the subscales.
CovariatesThe following covariates selected were related to the mother: age in years (≥ 30; < 30), race (white; nonwhite), education in years of schooling (> 9; ≤ 9), marital status (with a partner; without a partner), employment status (employed; unemployed), income in the minimum wage (≥ 1; < 1), head of household (yes; no), and common mental disorders (no; yes). Employment status was categorized according to the classification adopted by the Brazilian census (Instituto Brasileiro de Geografia e Estatística – IBGE, 2011): formal worker, informal worker, housewife, unemployed, student, or retired. In this report, the authors have grouped women as unemployed and employed.
The women's mental health in the past four weeks was assessed by the Self Reporting Questionnaire (SRQ-20), an instrument developed by the World Health Organization to detect psychiatric problems in primary health care for developing countries. It consists of twenty yes-no questions, four on physical symptoms and sixteen on psycho-emotional disorders.23 It was validated in Pernambuco.24 In data analysis, one point was assigned for each affirmative answer and zero for each negative answer. The cut-off score of the SRQ-20 for this study was defined as 7/8 and women were divided into two groups: non-suspected of common mental disorders (score ≤ 7) and suspected of common mental disorders (score ≥ 8).
Regarding children, the variables were: age (6–7 years; 8–9 years), sex (female; male), presence of siblings (no; yes), birth order (1st-2nd position; ≥ 3rd position), grade (≥ 2nd year; ≤ 1st year;), type of school (private; public).
The variables about the woman's partner were: father of the child (yes; no), race (white; non-white), employment status (employed; unemployed), and use of alcohol (no; yes).
The profile of the couple's relationship was measured by use of the variables: duration of the couple's relationship in years (> 6; ≤ 6), communication between the couple (good; poor), couple's fights in times per month (<1; ≥ 1) and intimate partner violence (no; yes).
Statistical analysisThe statistical analysis was performed using the Stata program version 13.0 for Windows.
The sample was described by the variables studied. The prevalence and associations of maternal educational practice (non-violent discipline, physical aggression, and its subdivisions, and psychological aggression) and the child's behavioral/emotional disorders were estimated through prevalence ratios, using Poisson regression considering the 95% confidence interval.
In the multivariate logistic regression analysis, it was included covariables that had p-value < 0.10 in the bivariate analysis with exposure and outcome.
This research was approved by the Research Ethics Committee of the Health Sciences Center of the Federal University of Pernambuco (ref 194.672 de 06/02/2013).
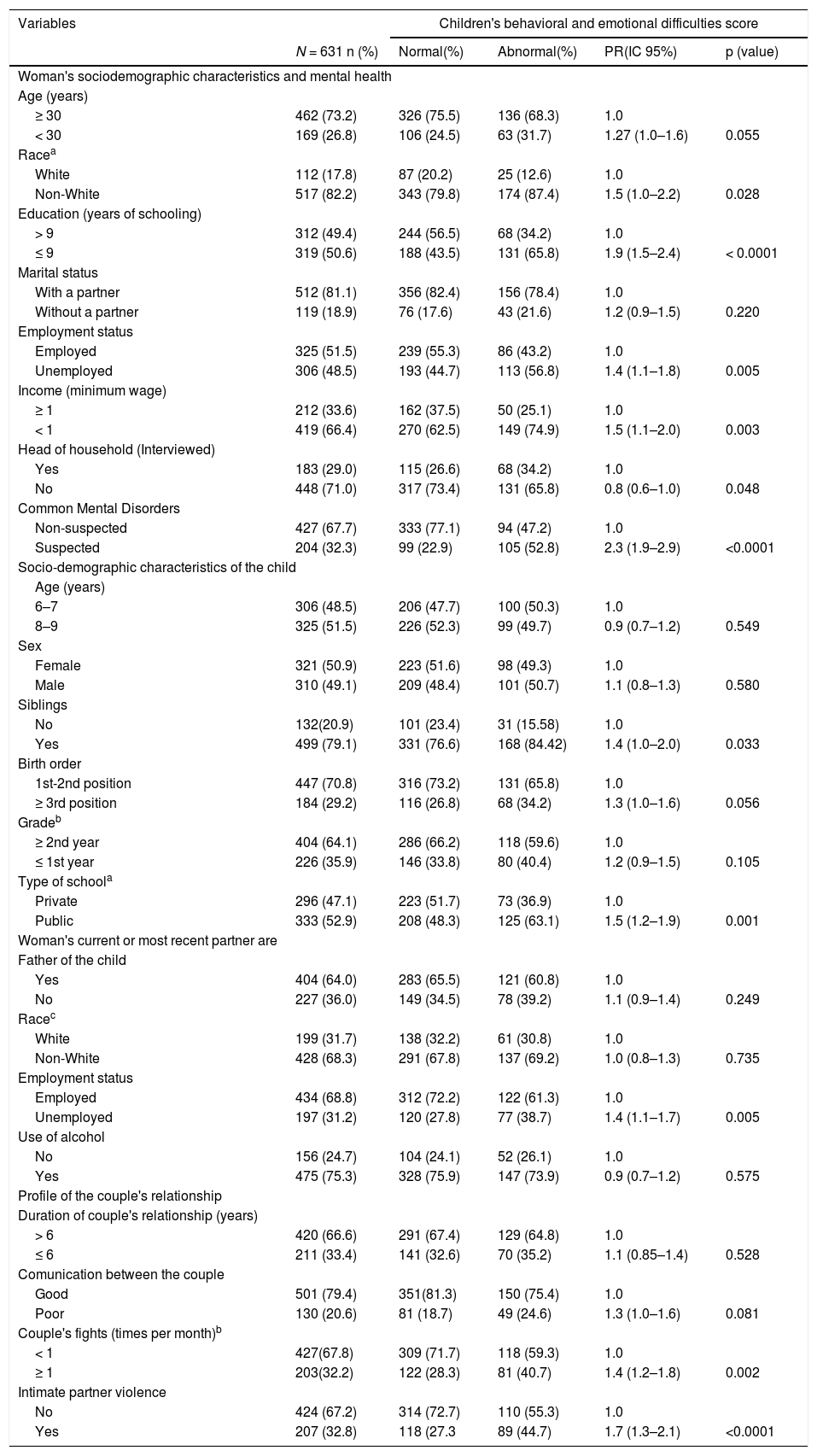
ResultsTable 1 shows the association between the child's behavioral and emotional disorders with the demographic and socioeconomic characteristics of the woman and her partner, the demographic characteristics of the child, the couple's relationship, and the woman´s mental health. The children who presented more behavioral and emotional problems, compared to those who had a normal score were those who had mothers under 30 years, were not white, with 9 years or less of study, were unemployed, with income < 1 minimum wage per month, and were suspected of common mental disorders.
Bivariate analysis between demographic and socioeconomic characteristics of the woman and her partner, demographic characteristics of the child, the couple's relationship, woman's mental health, and child behavioral and emotional disorders.
| Variables | Children's behavioral and emotional difficulties score | ||||
|---|---|---|---|---|---|
| N = 631 n (%) | Normal(%) | Abnormal(%) | PR(IC 95%) | p (value) | |
| Woman's sociodemographic characteristics and mental health | |||||
| Age (years) | |||||
| ≥ 30 | 462 (73.2) | 326 (75.5) | 136 (68.3) | 1.0 | |
| < 30 | 169 (26.8) | 106 (24.5) | 63 (31.7) | 1.27 (1.0–1.6) | 0.055 |
| Racea | |||||
| White | 112 (17.8) | 87 (20.2) | 25 (12.6) | 1.0 | |
| Non-White | 517 (82.2) | 343 (79.8) | 174 (87.4) | 1.5 (1.0–2.2) | 0.028 |
| Education (years of schooling) | |||||
| > 9 | 312 (49.4) | 244 (56.5) | 68 (34.2) | 1.0 | |
| ≤ 9 | 319 (50.6) | 188 (43.5) | 131 (65.8) | 1.9 (1.5–2.4) | < 0.0001 |
| Marital status | |||||
| With a partner | 512 (81.1) | 356 (82.4) | 156 (78.4) | 1.0 | |
| Without a partner | 119 (18.9) | 76 (17.6) | 43 (21.6) | 1.2 (0.9–1.5) | 0.220 |
| Employment status | |||||
| Employed | 325 (51.5) | 239 (55.3) | 86 (43.2) | 1.0 | |
| Unemployed | 306 (48.5) | 193 (44.7) | 113 (56.8) | 1.4 (1.1–1.8) | 0.005 |
| Income (minimum wage) | |||||
| ≥ 1 | 212 (33.6) | 162 (37.5) | 50 (25.1) | 1.0 | |
| < 1 | 419 (66.4) | 270 (62.5) | 149 (74.9) | 1.5 (1.1–2.0) | 0.003 |
| Head of household (Interviewed) | |||||
| Yes | 183 (29.0) | 115 (26.6) | 68 (34.2) | 1.0 | |
| No | 448 (71.0) | 317 (73.4) | 131 (65.8) | 0.8 (0.6–1.0) | 0.048 |
| Common Mental Disorders | |||||
| Non-suspected | 427 (67.7) | 333 (77.1) | 94 (47.2) | 1.0 | |
| Suspected | 204 (32.3) | 99 (22.9) | 105 (52.8) | 2.3 (1.9–2.9) | <0.0001 |
| Socio-demographic characteristics of the child | |||||
| Age (years) | |||||
| 6–7 | 306 (48.5) | 206 (47.7) | 100 (50.3) | 1.0 | |
| 8–9 | 325 (51.5) | 226 (52.3) | 99 (49.7) | 0.9 (0.7–1.2) | 0.549 |
| Sex | |||||
| Female | 321 (50.9) | 223 (51.6) | 98 (49.3) | 1.0 | |
| Male | 310 (49.1) | 209 (48.4) | 101 (50.7) | 1.1 (0.8–1.3) | 0.580 |
| Siblings | |||||
| No | 132(20.9) | 101 (23.4) | 31 (15.58) | 1.0 | |
| Yes | 499 (79.1) | 331 (76.6) | 168 (84.42) | 1.4 (1.0–2.0) | 0.033 |
| Birth order | |||||
| 1st-2nd position | 447 (70.8) | 316 (73.2) | 131 (65.8) | 1.0 | |
| ≥ 3rd position | 184 (29.2) | 116 (26.8) | 68 (34.2) | 1.3 (1.0–1.6) | 0.056 |
| Gradeb | |||||
| ≥ 2nd year | 404 (64.1) | 286 (66.2) | 118 (59.6) | 1.0 | |
| ≤ 1st year | 226 (35.9) | 146 (33.8) | 80 (40.4) | 1.2 (0.9–1.5) | 0.105 |
| Type of schoola | |||||
| Private | 296 (47.1) | 223 (51.7) | 73 (36.9) | 1.0 | |
| Public | 333 (52.9) | 208 (48.3) | 125 (63.1) | 1.5 (1.2–1.9) | 0.001 |
| Woman's current or most recent partner are | |||||
| Father of the child | |||||
| Yes | 404 (64.0) | 283 (65.5) | 121 (60.8) | 1.0 | |
| No | 227 (36.0) | 149 (34.5) | 78 (39.2) | 1.1 (0.9–1.4) | 0.249 |
| Racec | |||||
| White | 199 (31.7) | 138 (32.2) | 61 (30.8) | 1.0 | |
| Non-White | 428 (68.3) | 291 (67.8) | 137 (69.2) | 1.0 (0.8–1.3) | 0.735 |
| Employment status | |||||
| Employed | 434 (68.8) | 312 (72.2) | 122 (61.3) | 1.0 | |
| Unemployed | 197 (31.2) | 120 (27.8) | 77 (38.7) | 1.4 (1.1–1.7) | 0.005 |
| Use of alcohol | |||||
| No | 156 (24.7) | 104 (24.1) | 52 (26.1) | 1.0 | |
| Yes | 475 (75.3) | 328 (75.9) | 147 (73.9) | 0.9 (0.7–1.2) | 0.575 |
| Profile of the couple's relationship | |||||
| Duration of couple's relationship (years) | |||||
| > 6 | 420 (66.6) | 291 (67.4) | 129 (64.8) | 1.0 | |
| ≤ 6 | 211 (33.4) | 141 (32.6) | 70 (35.2) | 1.1 (0.85–1.4) | 0.528 |
| Comunication between the couple | |||||
| Good | 501 (79.4) | 351(81.3) | 150 (75.4) | 1.0 | |
| Poor | 130 (20.6) | 81 (18.7) | 49 (24.6) | 1.3 (1.0–1.6) | 0.081 |
| Couple's fights (times per month)b | |||||
| < 1 | 427(67.8) | 309 (71.7) | 118 (59.3) | 1.0 | |
| ≥ 1 | 203(32.2) | 122 (28.3) | 81 (40.7) | 1.4 (1.2–1.8) | 0.002 |
| Intimate partner violence | |||||
| No | 424 (67.2) | 314 (72.7) | 110 (55.3) | 1.0 | |
| Yes | 207 (32.8) | 118 (27.3 | 89 (44.7) | 1.7 (1.3–2.1) | <0.0001 |
About the children, most were aged between 8 and 9 years (51.5%), female (50.9%), had siblings (79.1%), with the 1st or 2nd position in birth order (70.8%), ≥ 2nd-year grade (64.1%), in a public school (52.9%).
Regarding the characteristics of the partner of the women, most of the partners were the parents of the children (64%), non-white (68.3%), unemployed (32.2%), and used alcohol (75.3%).
In the relationship profile, most of the couples had a relationship time > 6 years (66.6%), did not have good communication (20,6%) frequency of fights ≥ 1 time per month (32.2%), and reported intimate partner violence (32,8%).
The prevalence of child behavioral and emotional difficulties was 31.54% (199/631).
Bivariate analysis shows that the sociodemographic variables were strongly associated with children's abnormal total difficulties, except for age and marital status among women and use of alcohol among men. Children with high total difficulties scores were more likely to have siblings and to have attended a public than a private school. Couple's fights ≥ one time per month and intimate partner violence were also associated with children's abnormal total difficulties.
The violent maternal educational practice had high frequency. When describing the three dimensions of the instrument separately, 89.7% of the women reported acts of psychological aggression and 75.6% of physical aggression, which was subdivided into corporal punishment (73.5%), physical maltreatment (35.8%), and severe physical maltreatment (1.7%).
Non-violent discipline had a prevalence of 96.8% coexisting with violent discipline strategies.
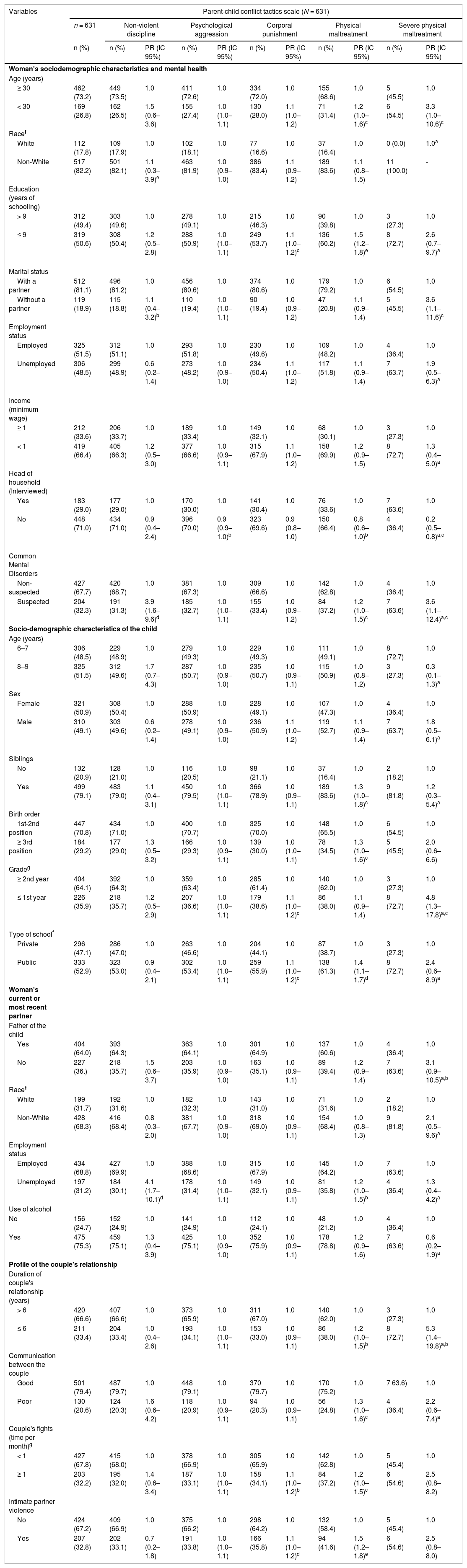
In the bivariate analysis (Table 2), corporal punishment was associated with lower maternal education, grade ≤ 1st year, public school, and intimate partner violence reported.
Bivariate analysis between demographic and socioeconomic characteristics of the woman and her partner, demographic characteristics of the child, couple's relationship, woman´s mental health and maternal educational practice.
| Variables | Parent-child conflict tactics scale (N = 631) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 631 | Non-violent discipline | Psychological aggression | Corporal punishment | Physical maltreatment | Severe physical maltreatment | ||||||
| n (%) | n (%) | PR (IC 95%) | n (%) | PR (IC 95%) | n (%) | PR (IC 95%) | n (%) | PR (IC 95%) | n (%) | PR (IC 95%) | |
| Woman's sociodemographic characteristics and mental health | |||||||||||
| Age (years) | |||||||||||
| ≥ 30 | 462 (73.2) | 449 (73.5) | 1.0 | 411 (72.6) | 1.0 | 334 (72.0) | 1.0 | 155 (68.6) | 1.0 | 5 (45.5) | 1.0 |
| < 30 | 169 (26.8) | 162 (26.5) | 1.5 (0.6–3.6) | 155 (27.4) | 1.0 (1.0–1.1) | 130 (28.0) | 1.1 (1.0–1.2) | 71 (31.4) | 1.2 (1.0–1.6)c | 6 (54.5) | 3.3 (1.0–10.6)c |
| Racef | |||||||||||
| White | 112 (17.8) | 109 (17.9) | 1.0 | 102 (18.1) | 1.0 | 77 (16.6) | 1.0 | 37 (16.4) | 1.0 | 0 (0.0) | 1.0a |
| Non-White | 517 (82.2) | 501 (82.1) | 1.1 (0.3–3.9)e | 463 (81.9) | 1.0 (0.9–1.0) | 386 (83.4) | 1.1 (0.9–1.2) | 189 (83.6) | 1.1 (0.8–1.5) | 11 (100.0) | - |
| Education (years of schooling) | |||||||||||
| > 9 | 312 (49.4) | 303 (49.6) | 1.0 | 278 (49.1) | 1.0 | 215 (46.3) | 1.0 | 90 (39.8) | 1.0 | 3 (27.3) | 1.0 |
| ≤ 9 | 319 (50.6) | 308 (50.4) | 1.2 (0.5–2.8) | 288 (50.9) | 1.0 (1.0–1.1) | 249 (53.7) | 1.1 (1.0–1.2)c | 136 (60.2) | 1.5 (1.2–1.8)e | 8 (72.7) | 2.6 (0.7–9.7)a |
| Marital status | |||||||||||
| With a partner | 512 (81.1) | 496 (81.2) | 1.0 | 456 (80.6) | 1.0 | 374 (80.6) | 1.0 | 179 (79.2) | 1.0 | 6 (54.5) | 1.0 |
| Without a partner | 119 (18.9) | 115 (18.8) | 1.1 (0.4–3.2)b | 110 (19.4) | 1.0 (1.0–1.1) | 90 (19.4) | 1.0 (0.9–1.2) | 47 (20.8) | 1.1 (0.9–1.4) | 5 (45.5) | 3.6 (1.1–11.6)c |
| Employment status | |||||||||||
| Employed | 325 (51.5) | 312 (51.1) | 1.0 | 293 (51.8) | 1.0 | 230 (49.6) | 1.0 | 109 (48.2) | 1.0 | 4 (36.4) | 1.0 |
| Unemployed | 306 (48.5) | 299 (48.9) | 0.6 (0.2–1.4) | 273 (48.2) | 1.0 (0.9–1.0) | 234 (50.4) | 1.1 (1.0–1.2) | 117 (51.8) | 1.1 (0.9–1.4) | 7 (63.7) | 1.9 (0.5–6.3)a |
| Income (minimum wage) | |||||||||||
| ≥ 1 | 212 (33.6) | 206 (33.7) | 1.0 | 189 (33.4) | 1.0 | 149 (32.1) | 1.0 | 68 (30.1) | 1.0 | 3 (27.3) | 1.0 |
| < 1 | 419 (66.4) | 405 (66.3) | 1.2 (0.5–3.0) | 377 (66.6) | 1.0 (0.9–1.1) | 315 (67.9) | 1.1 (1.0–1.2) | 158 (69.9) | 1.2 (0.9–1.5) | 8 (72.7) | 1.3 (0.4–5.0)a |
| Head of household (Interviewed) | |||||||||||
| Yes | 183 (29.0) | 177 (29.0) | 1.0 | 170 (30.0) | 1.0 | 141 (30.4) | 1.0 | 76 (33.6) | 1.0 | 7 (63.6) | 1.0 |
| No | 448 (71.0) | 434 (71.0) | 0.9 (0.4–2.4) | 396 (70.0) | 0.9 (0.9–1.0)b | 323 (69.6) | 0.9 (0.8–1.0) | 150 (66.4) | 0.8 (0.6–1.0)b | 4 (36.4) | 0.2 (0.5–0.8)a,c |
| Common Mental Disorders | |||||||||||
| Non-suspected | 427 (67.7) | 420 (68.7) | 1.0 | 381 (67.3) | 1.0 | 309 (66.6) | 1.0 | 142 (62.8) | 1.0 | 4 (36.4) | 1.0 |
| Suspected | 204 (32.3) | 191 (31.3) | 3.9 (1.6–9.6)d | 185 (32.7) | 1.0 (1.0–1.1) | 155 (33.4) | 1.0 (0.9–1.2) | 84 (37.2) | 1.2 (1.0–1.5)c | 7 (63.6) | 3.6 (1.1–12.4)a,c |
| Socio-demographic characteristics of the child | |||||||||||
| Age (years) | |||||||||||
| 6–7 | 306 (48.5) | 229 (48.9) | 1.0 | 279 (49.3) | 1.0 | 229 (49.3) | 1.0 | 111 (49.1) | 1.0 | 8 (72.7) | 1.0 |
| 8–9 | 325 (51.5) | 312 (49.6) | 1.7 (0.7–4.3) | 287 (50.7) | 1.0 (0.9–1.0) | 235 (50.7) | 1.0 (0.9–1.1) | 115 (50.9) | 1.0 (0.8–1.2) | 3 (27.3) | 0.3 (0.1–1.3)a |
| Sex | |||||||||||
| Female | 321 (50.9) | 308 (50.4) | 1.0 | 288 (50.9) | 1.0 | 228 (49.1) | 1.0 | 107 (47.3) | 1.0 | 4 (36.4) | 1.0 |
| Male | 310 (49.1) | 303 (49.6) | 0.6 (0.2–1.4) | 278 (49.1) | 1.0 (0.9–1.0) | 236 (50.9) | 1.1 (1.0–1.2) | 119 (52.7) | 1.1 (0.9–1.4) | 7 (63.7) | 1.8 (0.5–6.1)a |
| Siblings | |||||||||||
| No | 132 (20.9) | 128 (21.0) | 1.0 | 116 (20.5) | 1.0 | 98 (21.1) | 1.0 | 37 (16.4) | 1.0 | 2 (18.2) | 1.0 |
| Yes | 499 (79.1) | 483 (79.0) | 1.1 (0.4–3.1) | 450 (79.5) | 1.0 (1.0–1.1) | 366 (78.9) | 1.0 (0.9–1.1) | 189 (83.6) | 1.3 (1.0–1.8)c | 9 (81.8) | 1.2 (0.3–5.4)a |
| Birth order | |||||||||||
| 1st-2nd position | 447 (70.8) | 434 (71.0) | 1.0 | 400 (70.7) | 1.0 | 325 (70.0) | 1.0 | 148 (65.5) | 1.0 | 6 (54.5) | 1.0 |
| ≥ 3rd position | 184 (29.2) | 177 (29.0) | 1.3 (0.5–3.2) | 166 (29.3) | 1.0 (0.9–1.1) | 139 (30.0) | 1.0 (1.0–1.1) | 78 (34.5) | 1.3 (1.0–1.6)c | 5 (45.5) | 2.0 (0.6–6.6) |
| Gradeg | |||||||||||
| ≥ 2nd year | 404 (64.1) | 392 (64.3) | 1.0 | 359 (63.4) | 1.0 | 285 (61.4) | 1.0 | 140 (62.0) | 1.0 | 3 (27.3) | 1.0 |
| ≤ 1st year | 226 (35.9) | 218 (35.7) | 1.2 (0.5–2.9) | 207 (36.6) | 1.0 (1.0–1.1) | 179 (38.6) | 1.1 (1.0–1.2)c | 86 (38.0) | 1.1 (0.9–1.4) | 8 (72.7) | 4.8 (1.3–17.8)a,c |
| Type of schoolf | |||||||||||
| Private | 296 (47.1) | 286 (47.0) | 1.0 | 263 (46.6) | 1.0 | 204 (44.1) | 1.0 | 87 (38.7) | 1.0 | 3 (27.3) | 1.0 |
| Public | 333 (52.9) | 323 (53.0) | 0.9 (0.4–2.1) | 302 (53.4) | 1.0 (1.0–1.1) | 259 (55.9) | 1.1 (1.0–1.2)c | 138 (61.3) | 1.4 (1.1–1.7)d | 8 (72.7) | 2.4 (0.6–8.9)a |
| Woman's current or most recent partner | |||||||||||
| Father of the child | |||||||||||
| Yes | 404 (64.0) | 393 (64.3) | 363 (64.1) | 1.0 | 301 (64.9) | 1.0 | 137 (60.6) | 1.0 | 4 (36.4) | 1.0 | |
| No | 227 (36.) | 218 (35.7) | 1.5 (0.6–3.7) | 203 (35.9) | 1.0 (0.9–1.0) | 163 (35.1) | 1.0 (0.9–1.1) | 89 (39.4) | 1.2 (0.9–1.4) | 7 (63.6) | 3.1 (0.9–10.5)a,b |
| Raceh | |||||||||||
| White | 199 (31.7) | 192 (31.6) | 1.0 | 182 (32.3) | 1.0 | 143 (31.0) | 1.0 | 71 (31.6) | 1.0 | 2 (18.2) | 1.0 |
| Non-White | 428 (68.3) | 416 (68.4) | 0.8 (0.3–2.0) | 381 (67.7) | 1.0 (0.9–1.0) | 318 (69.0) | 1.0 (0.9–1.1) | 154 (68.4) | 1.0 (0.8–1.3) | 9 (81.8) | 2.1 (0.5–9.6)a |
| Employment status | |||||||||||
| Employed | 434 (68.8) | 427 (69.9) | 1.0 | 388 (68.6) | 1.0 | 315 (67.9) | 1.0 | 145 (64.2) | 1.0 | 7 (63.6) | 1.0 |
| Unemployed | 197 (31.2) | 184 (30.1) | 4.1 (1.7–10.1)d | 178 (31.4) | 1.0 (1.0–1.1) | 149 (32.1) | 1.0 (0.9–1.1) | 81 (35.8) | 1.2 (1.0–1.5)b | 4 (36.4) | 1.3 (0.4–4.2)a |
| Use of alcohol | |||||||||||
| No | 156 (24.7) | 152 (24.9) | 1.0 | 141 (24.9) | 1.0 | 112 (24.1) | 1.0 | 48 (21.2) | 1.0 | 4 (36.4) | 1.0 |
| Yes | 475 (75.3) | 459 (75.1) | 1.3 (0.4–3.9) | 425 (75.1) | 1.0 (0.9–1.0) | 352 (75.9) | 1.0 (0.9–1.1) | 178 (78.8) | 1.2 (0.9–1.6) | 7 (63.6) | 0.6 (0.2–1.9)a |
| Profile of the couple's relationship | |||||||||||
| Duration of couple's relationship (years) | |||||||||||
| > 6 | 420 (66.6) | 407 (66.6) | 1.0 | 373 (65.9) | 1.0 | 311 (67.0) | 1.0 | 140 (62.0) | 1.0 | 3 (27.3) | 1.0 |
| ≤ 6 | 211 (33.4) | 204 (33.4) | 1.0 (0.4–2.6) | 193 (34.1) | 1.0 (1.0–1.1) | 153 (33.0) | 1.0 (0.9–1.1) | 86 (38.0) | 1.2 (1.0–1.5)b | 8 (72.7) | 5.3 (1.4–19.8)a,b |
| Communication between the couple | |||||||||||
| Good | 501 (79.4) | 487 (79.7) | 1.0 | 448 (79.1) | 1.0 | 370 (79.7) | 1.0 | 170 (75.2) | 1.0 | 7 63.6) | 1.0 |
| Poor | 130 (20.6) | 124 (20.3) | 1.6 (0.6–4.2) | 118 (20.9) | 1.0 (0.9–1.1) | 94 (20.3) | 1.0 (0.9–1.1) | 56 (24.8) | 1.3 (1.0–1.6)c | 4 (36.4) | 2.2 (0.6–7.4)a |
| Couple's fights (time per month)g | |||||||||||
| < 1 | 427 (67.8) | 415 (68.0) | 1.0 | 378 (66.9) | 1.0 | 305 (65.9) | 1.0 | 142 (62.8) | 1.0 | 5 (45.4) | 1.0 |
| ≥ 1 | 203 (32.2) | 195 (32.0) | 1.4 (0.6–3.4) | 187 (33.1) | 1.0 (1.0–1.1) | 158 (34.1) | 1.1 (1.0–1.2)b | 84 (37.2) | 1.2 (1.0–1.5)c | 6 (54.6) | 2.5 (0.8–8.2) |
| Intimate partner violence | |||||||||||
| No | 424 (67.2) | 409 (66.9) | 1.0 | 375 (66.2) | 1.0 | 298 (64.2) | 1.0 | 132 (58.4) | 1.0 | 5 (45.4) | 1.0 |
| Yes | 207 (32.8) | 202 (33.1) | 0.7 (0.2–1.8) | 191 (33.8) | 1.0 (1.0–1.1) | 166 (35.8) | 1.1 (1.0–1.2)d | 94 (41.6) | 1.5 (1.2–1.8)e | 6 (54.6) | 2.5 (0.8–8.0) |
As for physical maltreatment, several covariates were associated with this type of violence, such as age < 30 years, lower education, and common mental disorders (related to women); presence of siblings, birth order ≥ 3rd position, public school (related to the child); poor communication, frequency of couple's fights ≥ 1 per month and intimate partner violence (related to the profile couple's relationship).
Severe physical maltreatment was associated with: age <30 years, without a partner, not the head of household, and common mental disorder of the woman, child's grade ≤ 1st year, and couple's relationship time ≤ 6 years.
Table 3 shows the association of maternal educational practice, in the last 12 months, with the child's behavioral and emotional disorders even after adjusting for confounders. Mental health difficulties of child were associated with corporal punishment (adjustedPR=1.5; 95% CI: 1.1–2.1; p = 0.010) and with severe physical maltreatment (adjustedPR=1.9; 95% CI: 1.3–2.8; p = 0.002) compared to children not exposed.
Association between maternal educational practice and the child behavioral and emotional disorders at school age reported by mothers using the Strengths and Difficulties Questionnaire.
| Children's behavioral and emotional difficulties score (n = 631) | |||||
|---|---|---|---|---|---|
| Parent-child conflict tactics scale | n = 631 n (%) | Normal (%) | Abnormal (%) | PR unadjusted (IC 95%) | PR adjusted (IC 95%) |
| Non-violent discipline | |||||
| Yes | 611 (96.8) | 418 (68.4) | 193 (31.6) | 1.0 | |
| No | 20 (3.2) | 14 (70.0) | 6 (30.0) | 0.9 (0.5–1.9) | Not applicable |
| p (value) | 0.882 | ||||
| Psychological aggression | |||||
| No | 65 (10.3) | 52 (80.0) | 13 (20.0) | 1.0 | 1.0 |
| Yes | 566 (89.7) | 380 (67.1) | 186 (32.9) | 1.6 (1.0–2.7) | 1.6 (1.0–2.6) |
| p (value) | 0.052 | 0.064a | |||
| Corporal punishment | |||||
| No | 167 (26.5) | 132 (79.0) | 35 (21.0) | 1.0 | 1.0 |
| Yes | 464 (73.5) | 300 (64.7) | 164 (35.3) | 1.7 (1.2–2.3) | 1.5 (1.1–2.1) |
| p (value) | 0.001 | 0.010b | |||
| Physical maltreatment | |||||
| No | 405 (64.2) | 294 (76.6) | 111 (27.4) | 1.0 | 1.0 |
| Yes | 226 (35.8) | 138 (61.1) | 88 (38.9) | 1.4 (1.1–1.8) | 1.2 (0.9–1.5) |
| p (value) | 0.003 | 0.115c | |||
| Severe physical maltreatment | |||||
| No | 620 (98.3) | 430 (69.4) | 190 (30.6) | 1.0 | 1.0 |
| Yes | 11 (1.7) | 2 (18.2) | 9 (81.8) | 2.7 (2.0–3.6) | 1.9 (1.3–2.8) |
| p (value) | 0.001e | 0.002d | |||
This study evaluated the frequency of mental health disorders in schoolchildren from a low-income community in Northeast Brazil, exposed or not to violent maternal educational practice. Corporal punishment and severe physical aggression, used by the mother as disciplinary educational practices, remained associated with mental health disorders even after controlling for confounding variables.
Non-violent discipline was a frequent practice in conflict resolution that mothers used with their children as well as other studies show.5,25 This maternal attitude is positive because it is a discipline that leads the child to reflect and understand inappropriate behaviors, consequently stimulating the management of emotions and the regulation of behaviors.5,25
However, negative educational practices, such as psychological aggression, corporal punishment, physical aggression, and severe physical punishment, presented high percentages, which reveals the co-occurrence of negative and positive maternal educational practices. This fact suggests the possibility that when non-violent practices do not result in the desired effect on children's behavior, mothers use violent strategies.5
The hypothesis for mothers to use violent educational practices is to teach appropriate behaviors, according to their rules, but studies6 show the ineffectiveness and negative impacts of these practices on socio-emotional development and a greater chance of problems in the mental health of children, as also demonstrated by the present results.
Corporal punishment, as well as psychological aggression, appears as a frequent practice of disciplining children in different countries and cultures,26 both in high-income countries27 and in low- and middle-income countries,28 which supports the results of the present study, carried out in a low-income community. However, corporal punishment, of any severity level, only controls inappropriate behavior due to fear of the aggressor and promotes the resolution of conflicts through violence, favoring the transgenerational transmission of violence, as demonstrated in studies that report that parents with a history of childhood violence use more negative educational practices.29
The prevalence of child behavioral and emotional disorders is higher than in international studies.21 However, it is very similar to other Brazilian studies in which the samples of children evaluated have similar socioeconomic status,19,25 and factors associated with violent parenting practices such as maternal common mental disorders and intimate partner violence.30
The study has some limitations. The prevalence of violent maternal educational practices was high, but it is still possible to have an information bias because the CTSPC scale was reported only by the child's mother, which may underestimate the prevalence of violent practices, especially physical abuse. Therefore, to minimize this limitation, the strategy of interspersing randomly the questions is used to make the objectives of the questions less evident and to reduce the possibility of negative answers regarding the occurrence of violence. This information bias may also have occurred in the prevalence of the child's behavioral and emotional disorders, as it is assessed only from the perspective of the mother who tends to overestimate behavioral changes in her children. Although the study is aligned with a cohort, the cross-sectional study does not allow for the establishment of causality. However, based on the literature, including longitudinal studies,13 there seems to be a strong association between violent parental practices and behavioral and emotional disorders in the child. In addition, cross-sectional studies are faster to be applied and all variables are collected in a single moment so that they can be used to describe the population studied.
Thus, the high prevalence of the violent maternal educational practice, especially corporal punishment and severe physical abuse, and the association with children's mental health problems, as well as the involvement of factors from the family context show the complexity of the theme. Therefore, the results reinforce the need for interventions that promote support and encouragement for parents to effectively use non-violent discipline in conducting the educational process, making it possible to establish healthier relationships between mothers and children to prevent and mitigate the impact of emotional and behavioral problems in childhood. Future studies should involve both parents in the assessment of parenting practices and variables related to the cultural background as this might better represent the child's behavior in the family context.
This study was supported by the Brazilian Federal Government, through the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) do Ministério da Educação e Cultura, Brazil – Grant numbers: 403060/2004-4 and 475240/2011-1, and the Departamento de Ciência e Tecnologia da Secretaria de Ciência, Tecnologia e Insumos Estratégicos do Ministério da Saúde (DECIT), Brazil – Grant number: 473545/2004-7.





