

To evaluate the lifestyle and quality of life in Brazilian children and adolescents during the COVID-19 social distancing period in 2020.
MethodsThis cross-sectional study evaluated children and adolescents (2-18 years of age) and their parents, who voluntarily participated in an online survey. Snowball sampling was used to recruit participants during the first 6 months of the pandemic. A questionnaire was used to characterize the study population. The PedsQL 4.0 and the EUROHIS-QOL 8-item index were used to assess the quality of life (QoL) in children/adolescents and parents, respectively. Data were analyzed using SPSS 18.0 statistical program through the ANOVA with post hoc Bonferroni analysis, student's t test, and the generalized estimating equation.
ResultsMean screen time increased from 2h pre-pandemic to 5h during the pandemic (p < 0.001), which was associated with a decline in PedSQL4.0 scores (from 75.7 ± 2.6 to 71.3 ± 13.7, p < 0.001). Unhealthy eating habits increased from 11% to 34% and were associated with worse QoL scores compared with improved or unchanged eating habits during the pandemic (69.7 ± 13.3 vs 72.80 ± 13.4 vs 76.4 ± 12.6; p < 0.001). Poor sleep quality increased from 9% to 31.7% and was associated with worse QoL scores compared to improved or unchanged sleep quality during the pandemic (67.3 ± 13.1 vs 74.5 ± 13.1 vs 76.8 ± 12.2; p < 0.05). Physical exercise was associated with better PedSQL4.0 scores (77.5 ± 12.3 vs 72.5 ± 14.4; p < 0.001). Children aged 2-4y old had the best QoLscores.
ConclusionsPandemic-related social distancing promoted significant lifestyle changes in children and adolescents, increasing screen time, reducing physical activity, and worsening food and sleep quality, which resulted in worse QoL scores.
On March 2020, COVID-19 was declared a pandemic by the World Health Organization (WHO). Although children can be affected by COVID-19, serious illnesses are less common. Even with an increased number of cases in children observed in the 2nd and 3rd year of the pandemic, the absolute number of cases is quite small compared with the adult population.1,2 According to a systematic review conducted during the beginning of the pandemic and the period of this study, only 1–5% of COVID-19 cases occurred in children < 18 years of age; among these, 5–20% were hospitalized and 0.58–2% were admitted to a pediatric intensive care unit.3 In addition, over time, severity in children was more significant when they were associated with other viral and multisystem inflammatory syndromes related to covid-19.4,5 Although most children are asymptomatic or have mild symptoms, this population may have sequelae of the disease or be indirectly affected by the pandemic.
Social distancing measures such as closing establishments and interrupting services were in accordance with WHO recommendations. This mobility restriction policy was considered the most effective way to decrease the spread of COVID-19 among the population and to prevent the healthcare system from collapsing. Such measures have negative effects on society, such as increased unemployment rates, reduced wages, and closure of schools and recreational environments, among others.6 These changes have been a challenge for families, especially those in conditions of social vulnerability, and children may suffer the most from the consequences.6,7
There are studies currently evaluating mental health and lifestyle changes in the population during the pandemic, but little is said about quality of life (QoL). Existing research demonstrates that COVID-19 has a psychological impact, such as anxiety, stress, and depression associated with fear of disease progression, exposure to COVID-19 information, and adherence to preventive measures.8-10 In addition, studies have reported increases in sedentary lifestyle and screen exposure time, as well as worsening food and sleep quality.11 These findings suggest that the pandemic affects the QoL of children and adolescents through direct or indirect parental influence, as well as by inducing changes in lifestyle and routine.
The WHO defines QoL as “an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.” Factors such as level of physical activity, hours of sleep, healthy eating with daily consumption of fruits and vegetables, not drinking alcohol and not smoking tobacco, and reduced screen time can affect QoL in children and adolescents.12
To better understand this scenario, this study aimed to investigate lifestyle and QoL changes in children and adolescents from several Brazilian cities during the critical period of social distancing.
MethodsA cross-sectional study was conducted in several Brazilian cities using an online survey to evaluate QoL in children and adolescents (2 to 18 years) during the COVID-19 pandemic. The study was approved by the Research Ethics Committee of Hospital de Clínicas de Porto Alegre (CAAE protocol number 32455020.4.0000.5327). Informed consent was obtained from all participants (parents or legal guardians as well as by the older children and adolescents) before responding the online questionnaire.
Between June 23, 2020, and July 12, 2020, the researchers used different platforms of social media (Instagram, Facebook, messaging applications, and email) to send explicit invitations to their contacts and the general public to participate in the study. It was the third and fourth months of the COVID-19 pandemic in Brazil, which is considered a critical period of social distancing. The contacted individuals were stimulated to share the invitation with their network of contacts with the aim of spreading exponentially the invitation. This recruitment method is denominated as Snowballing sampling. The authors intended to include several states and different socioeconomic classes in the study; however, a greater adherence was expected from the states of Rio Grande do Sul and Rio de Janeiro and higher social classes due to the researchers’ area of influence.
Parents or legal guardians of children aged 2 to 18 years who adhered to some social distancing measures and/or underwent routine changes due to COVID-19 prevention measures were considered eligible to participate in the study. To answer the questionnaire, participants accessed the following link: https://docs.google.com/forms/d/e/1FAIpQLScmoR6De_K_E09iEY0gteTcpt2GK_syiUt_jk_6vD-bnsapw/viewform?usp=sf_link.
The initial part of the questionnaire assessed the sociodemographic characteristics of parents/legal guardians, including gender, age, number of children, marital status, level of education, income, profession, and changes in work routine, among others. The second part of the questionnaire included questions about their children's age, level of education, type of school (public or private), and potential changes in behavior and daily activities, such as screen time, level of physical activity, and sleep and food quality. The Brazilian Society of Pediatrics recommends that children should not be exposed to a device screen for more than two hours per day. This cutoff point was adopted in this study to define prolonged exposure to the screen electronic dispositive. Parents and legal guardians answered another questionnaire assessing their and their children's QoL.
To assess QoL in children and adolescents, the Pediatric Quality of Life Inventory version 4.0 (PedsQL 4.0) was used, which is a cross-culturally validated questionnaire with specific versions for different age groups: 2–4 years, 5–7 years, 8–12 years, and 13–18 years.13 The PedsQL 4.0 comprises core health issues succinctly, including the physical, emotional, social, and school functioning dimensions. The instrument asks how much of a problem each item has been during the past month. The questionnaire is comprised of child self-report and parent self-report.13 However, due to the pandemic and upon authorization, the online version was used, which includes only the parent self-report.
To assess QoL in parents and legal guardians, the WHO's European Health Interview Survey – Quality of Life (EUROHIS-QOL) 8-item index was used, which covers issues from each of the four fundamental domains: physical, emotional, social, and environmental. The EUROHIS-QOL 8-item index is composed of 8 questions (overall QoL, overall health, energy level, daily activities, self-esteem, personal relationships, money, and living situation) referring to the 2 weeks prior to the application of the questionnaire.14
Continuous variables were expressed as mean (SD) or median (IQR), and categorical variables were expressed as relative frequency. All data were analyzed in SPSS, version 18.0. The Shapiro-Wilk test was used to assess the normality of variables. Analysis of variance (ANOVA) with post hoc Bonferroni correction was used to determine an association between QoL and age group in children and adolescents. ANOVA and Student's t test were used to determine a correlation between QoL and screen time, level of physical activity, hours of sleep, and healthy eating in children and adolescents. Parent-related variables (age, level of education, income, and QoL, among others) were analyzed using the generalized estimating equation (GEE) with normal distribution. Bivariate analysis was then performed with a cut-off point of p < 0.1 to choose significant variables. The variables were then evaluated using the multivariable GEE method. The level of significance was set at 5%.
ResultsOf 2,685 people who volunteered to participate in the study, 111 were excluded for not having children, resulting in a sample of 2,574 parents and legal guardians. This study included several Brazilian states, but there was greater adherence from the states of Rio Grande do Sul (73.9%) and Rio de Janeiro (10.3%), followed by Santa Catarina (3.9%), São Paulo (2.4%), and other states (9.5%).
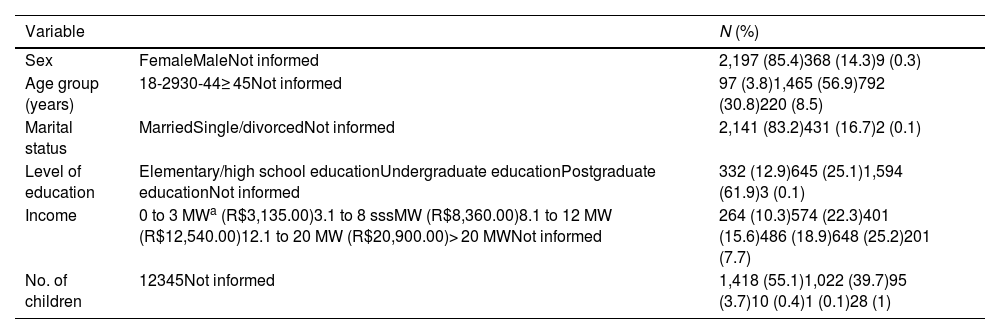
Most participants were women (85.4%), married (83.2%), had only one child (55.1%), had completed postgraduate education (61.9%), and had high purchasing power, that is, more than 20 minimum wages (25.2%) (Table 1).
Demographic characteristics of parents and legal guardians (N = 2574).
| Variable | N (%) | |
|---|---|---|
| Sex | FemaleMaleNot informed | 2,197 (85.4)368 (14.3)9 (0.3) |
| Age group (years) | 18-2930-44≥ 45Not informed | 97 (3.8)1,465 (56.9)792 (30.8)220 (8.5) |
| Marital status | MarriedSingle/divorcedNot informed | 2,141 (83.2)431 (16.7)2 (0.1) |
| Level of education | Elementary/high school educationUndergraduate educationPostgraduate educationNot informed | 332 (12.9)645 (25.1)1,594 (61.9)3 (0.1) |
| Income | 0 to 3 MWa (R$3,135.00)3.1 to 8 sssMW (R$8,360.00)8.1 to 12 MW (R$12,540.00)12.1 to 20 MW (R$20,900.00)> 20 MWNot informed | 264 (10.3)574 (22.3)401 (15.6)486 (18.9)648 (25.2)201 (7.7) |
| No. of children | 12345Not informed | 1,418 (55.1)1,022 (39.7)95 (3.7)10 (0.4)1 (0.1)28 (1) |
A total of 3,221 responses assessing QoL in children and adolescents were obtained, of which 20.9% involved children between 2 and 4 years of age, 22.3% between 5 and 7 years of age, 32.2% between 8 and 12 years of age, and 24.6% between 13 and 18 years of age. During the pandemic, children aged between 2 and 4 years had better QoL scores compared with the other age groups (Table 2). Most study participants attended private schools (85.5%); however, QoL was not statistically significant when comparing private and public schools (73.7 ± 13.1 vs 72.0 ± 13.5, respectively, p = 0.06).
Quality of life assessment (PedsQL) in children and adolescents during the COVID-19 pandemic in Brazil.
| Age group (years) | N (%) | Mean ± SD |
|---|---|---|
| 2–4 | 673 (20.9) | 79.1 ± 11.2a |
| 5–7 | 719 (22.3) | 72.8 ± 12.9 |
| 8–12 | 1,036 (32.2) | 71.6 ± 13.3 |
| 13–18 | 793 (24.6) | 72.4 ± 14.0 |
Analysis of variance (p < 0.001) with post hoc Bonferronia correction (p < 0.05).
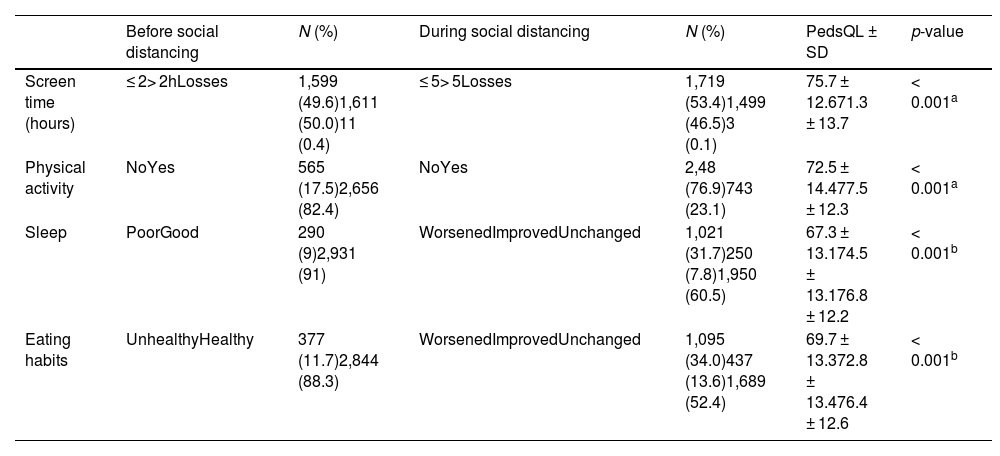
Questionnaire answers revealed that most parents and legal guardians were affected by some type of change in their work routine or job due to social distancing measures. Before March 2020, 86% of respondents were employed, of whom 71% experienced some type of change after social distancing measures were implemented. Among these, 6% reported losing their job, whereas the remaining 65% reported changes in work routines such as reduced or increased working hours, work overload, wage reduction, and transition to remote work, among others. Pandemic-related social distancing also promoted significant lifestyle changes in children and adolescents, such as prolonged screen time, decreased levels of physical activity, and changes in hours of sleep and eating habits (Table 3).
Screen time, physical activity, and sleep and food quality before and during the COVID-19 social distancing period and quality of life during the COVID-19 social distancing period in children and adolescents, Brazil.
| Before social distancing | N (%) | During social distancing | N (%) | PedsQL ± SD | p-value | |
|---|---|---|---|---|---|---|
| Screen time (hours) | ≤ 2> 2hLosses | 1,599 (49.6)1,611 (50.0)11 (0.4) | ≤ 5> 5Losses | 1,719 (53.4)1,499 (46.5)3 (0.1) | 75.7 ± 12.671.3 ± 13.7 | < 0.001a |
| Physical activity | NoYes | 565 (17.5)2,656 (82.4) | NoYes | 2,48 (76.9)743 (23.1) | 72.5 ± 14.477.5 ± 12.3 | < 0.001a |
| Sleep | PoorGood | 290 (9)2,931 (91) | WorsenedImprovedUnchanged | 1,021 (31.7)250 (7.8)1,950 (60.5) | 67.3 ± 13.174.5 ± 13.176.8 ± 12.2 | < 0.001b |
| Eating habits | UnhealthyHealthy | 377 (11.7)2,844 (88.3) | WorsenedImprovedUnchanged | 1,095 (34.0)437 (13.6)1,689 (52.4) | 69.7 ± 13.372.8 ± 13.476.4 ± 12.6 | < 0.001b |
Mean screen time significantly increased from 2h pre-pandemic to 5h during the pandemic (Table 3). Those with more screen time showed a decline in PedSQL4.0 scores (from 75.7 ± 12.6 to 71.3 ± 13.7; p < 0.001).
Before the pandemic, 82.4% of participants practiced regular physical activity, whereas only 23.1% continued practicing physical activity during the pandemic (Table 3). Those who continued practicing physical activity had better PedSQL4.0 scores than those who stopped practicing (77.5 ± 12.3 vs 72.5 ± 14.4, respectively; p < 0.001).
The lack of healthy eating habits increased from 11.7% pre-social distancing to 34% after social distancing measures were implemented (Table 3). The QoL assessment showed that those with worsening eating habits had lower PedSQL4.0 scores than those with improved or unchanged eating habits (69.7 ± 13.3 vs 72.80 ± 13.4 vs 76.4 ± 12.6, respectively; p < 0.001).
Poor sleep quality increased from 9% before the pandemic to 31.7% during the pandemic (Table 3). Of note, those with worsening sleep quality also had worse QoL compared with those with improved or unchanged sleep quality during the pandemic (67.3 ± 13.1 vs 74.5 ± 13.1 vs 76.8 ± 12.2, respectively; p < 0.05).
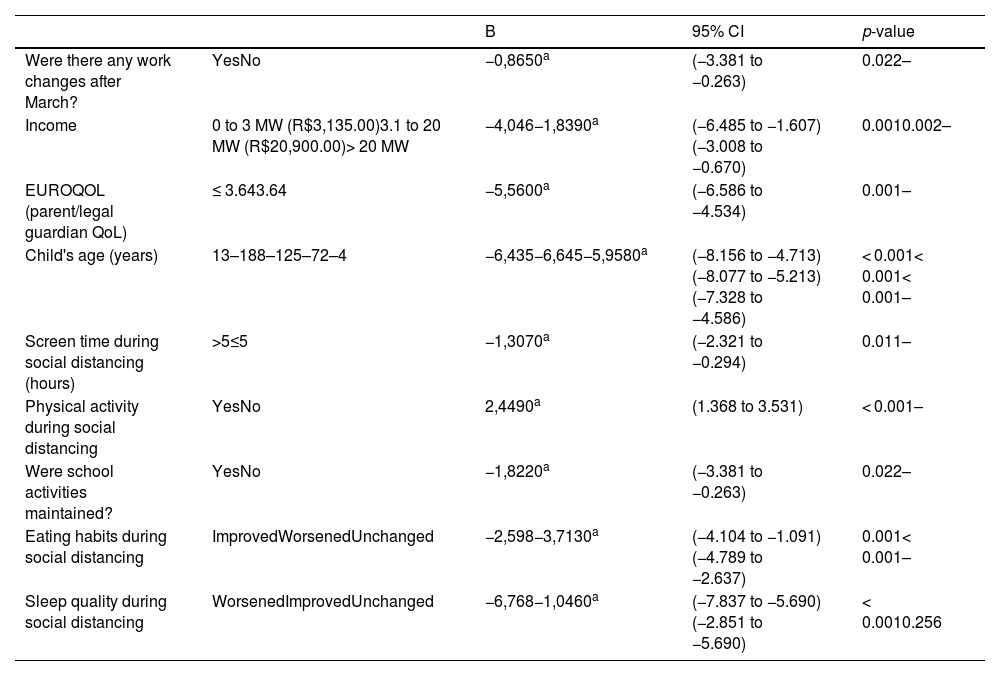
There was a positive association between QoL in children and adolescents and QoL in parents, that is, the higher the QoL in parents, the higher the QoL in children. Likewise, the higher the income and the rates of employment, the higher the QoL in children and adolescents. Table 4 shows the association between the study variables that were significantly correlated with QoL in children and adolescents.
Multivariate analysis of changes in work routine, income, quality of life in parents and legal guardians, children's age, screen time, level of physical activity, sleep quality, and eating habits in relation to quality of life in children and adolescents (dependent variable) during the COVID-19 pandemic.
Similarly to what was described in previous studies,15,16 the present results demonstrated that the COVID-19 pandemic affected the lifestyle of both adult and children/adolescent populations. There were relevant changes in the work pattern of parents and legal guardians, with possible repercussions on economic aspects and family lifestyle. Social isolation and changes in the family lifestyle also affected the behavior of children and adolescents, resulting in increased length of screen exposure time, reduced levels of regular physical activity, and worsened sleep and food quality. Interestingly, children aged between 2 and 4 years old were less impacted with these changes. Parents and legal guardians, mostly mothers with high schooling and high socioeconomic status, with higher QoL were protective factors to preserve better QoL in children and adolescents. However, it should be remarked that the sample was predominantly composed of females with a high educational degree and socioeconomic level.
The Brazilian Society of Pediatrics and several authors recommend avoiding screen exposure in children < 2 years and limiting screen time to 1-3 hours per day according to the age group.17 The 150% increase in mean screen time (from 2h to 5h) observed in this study is likely associated with the social distancing policy, which included the closing of schools and recreational environments, consequently reducing leisure options and social interaction among children and adolescents.11,18 Increased screen exposure time and significantly reduced levels of regular physical activity are associated with delayed language development, sleep disorders, and changes in mental health. They can lead to noncommunicable diseases such as overweight and obesity, myopia, and high blood pressure, among others, which could explain a possible worsening QoL in the study population17,18
Physical activity and sedentary behavior have also been widely discussed since before the COVID-19 pandemic.19 A large systematic review showed that higher levels of physical activity and reduced time of screen-based sedentary behavior, such as watching television and using smartphones, lead to improved QoL in the population of children and adolescents without chronic diseases such as obesity.20 Such behavior was associated with better physical and mental well-being and may benefit several health conditions. Sedentary behaviors were associated with several negative consequences, such as an increased prevalence of noncommunicable diseases such as obesity, cardiovascular diseases, and psychological problems, in addition to contributing to developmental delay and poor school performance among children and young people.20
The social distancing measures implemented during the COVID-19 epidemic, which included the closing of schools, gyms, parks, and playgrounds, significantly reduced the levels of physical activity, further aggravating this health problem.11 Corroborating these data, the rates of physical inactivity in this study increased from 17.5% pre-pandemic to 76.9% during the social distancing period. Increased physical inactivity was associated with worsening QoL, highlighting the consequences of a sedentary lifestyle.11,21
Of note, 34% of adolescents and children reported worsening quality of food, which was also associated with worsening QoL. This resulted from changes in eating behaviors caused by the pandemic. Some studies reported that COVID-19-related stress led parents to modify their eating habits, consequently modifying the eating habits of their children as well.22,23 Some parents became more permissive, allowing the child/adolescent to be more autonomous, whereas other parents increased the supply of non-nutritive foods. Some parents engaged in emotional eating and used a method of reward. In addition, changes in appetite, frequent snacking, emotional excesses, increased purchases of non-nutritious foods to stock up, and increased consumption of fast food were observed.17,22,23 Conversely, some families planned and created food-oriented routines, increasing the number of family meals because of remote work and the responsibility of taking care of their children, which could benefit children's diet and justify the improved QoL in those with improved eating habits.22,23
Regarding sleep quality, most study participants reported worsening sleep quality, which was associated with worse QoL. Depression, confinement, and stress are known to negatively impact sleep quality. The COVID-19 pandemic has increased the incidence of mental health-related disorders, with higher rates of insomnia, anxiety, depression, and suicidal thoughts.9 In addition, studies have shown changes in the sleep pattern of children and adolescents due to routine changes promoted by the closure of schools.24 Worsening sleep quality may also have been influenced by screen exposure time, levels of physical activity, eating habits, reduced social interactions, and parental stress.24
As referred before, children between 2 and 4 years old presented better QoL scores when compared to older children. There are few studies during the pandemic enrolling this young group of children. However, it is well known that parenting has different influences along the child's period of age and development. Therefore, dysfunctional families are associated with mental distress and harmful parenting behaviors for children.25 On the contrary, constructive parenting practices are associated with better family dynamics with consequent improvement in child development. Studies have shown that families with better socioeconomic levels have reorganized themselves in order to create a routine in the home environment aiming to reduce the harm in the lives of their children, including the use of the media as a way to promote physical activity in younger children, for example.26 Therefore, this finding may be associated with the fact that this age group receives more attention and care from parents, does not have high expectations regarding socialization, and does not undergo many lifestyle changes compared with older children.25
Noteworthy is that 71% of interviewed parents reported changes in their employment relationship, of whom 6% reported losing their job. Such changes were associated with worse QoL in children and adolescents. After all, work-related changes are known to cause social and economic concerns and impact the mental health of parents, with worsening health-related QoL, which can indirectly interfere with the environment where they live, thus corroborating the results.16,27
Likewise other studies, the present study corroborates the close and positive association between QoL in children and QoL in parents.28,29 In addition, there is an association between child and parent self-report. However, the levels of agreement can be affected by the child's age, investigated domains, and parent QoL.30
The present study presents some limitations, a) mainly related to the characteristics of the sample recruited. The present results demonstrated that a very particular portion of the society was included and analyzed. The great majority of families involved presented a high scholarly level and belonged to the most elevated economical stratus, which is quite far from the average Brazilian population; b) the voluntary and spontaneous adherence questionnaire, which may have attracted participants who were significantly impacted by social distancing, thus influencing the prevalence and proportionality of some results, and c) the cross-sectional nature of the study, which prevents us from stating whether the findings result solely from social distancing measures and whether QoL impairment is permanent, that is, there is no causal inference. Despite these limitations, the sample size (over 2,500 responses) and the use of validated instruments strongly suggest that the present data are very close to the reality of children and adolescents whose routine was impacted by the COVID-19 pandemic and the widespread and prolonged period of social distancing. Additionally, longitudinal studies involving this population are necessary because some habits acquired during the pandemic may be in force, and mental changes require continuous monitoring by health professionals.
Considering the definition of QoL proposed by the WHO (“an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns”), the authors can state that changes in family routine and society have a key role in changing living standards, which can directly impact QoL in children and adolescents. Pandemic-related social distancing promoted significant lifestyle changes in children and adolescents, increasing screen time exposure, reducing physical activity, and worsening food and sleep quality, which resulted in worse QoL scores. The authors believe that the present results corroborate the importance of re-analysis and reassessment of the measures implemented to combat the COVID-19 pandemic and their consequences on QoL, especially in children and adolescents, to mitigate any adverse effects.
The authors thank Vania Naomi Hirakata Vhirakata for assisting in the statistical analysis.
Institution: Programa de pós-graduação em saúde da criança e do adolescente, Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, Brasil.





