
there are many questions and little evidence regarding the diagnosis and treatment of gastroesophageal reflux disease (GERD) in children. The association between GERD and cow's milk protein allergy (CMPA), overuse of abdominal ultrasonography for the diagnosis of GERD, and excessive pharmacological treatment, especially proton-pump inhibitors (PPIs) are some aspects that need clarification. This review aimed to establish the current scientific evidence for the diagnosis and treatment of GERD in children.
Data sourcea search was conducted in the MEDLINE, PubMed, LILACS, SciELO, and Cochrane Library electronic databases, using the following keywords: gastroesophageal reflux; gastroesophageal reflux disease; proton-pump inhibitors; and prokinetics; in different age groups of the pediatric age range; up to May of 2013.
Data synthesisabdominal ultrasonography should not be recommended to investigate gastroesophageal reflux (GER). Simultaneous treatment of GERD and CMPA often results in unnecessary use of medication or elimination diet. There is insufficient evidence for the prescription of prokinetics to all patients with GER/GERD. There is little evidence to support acid suppression in the first year of life, to treat nonspecific symptoms suggestive of GERD. Conservative treatment has many benefits and with low cost and no side-effects.
Conclusionsthere have been few randomized controlled trials that assessed the management of GERD in children and no examination can be considered the gold standard for GERD diagnosis. For these reasons, there are exaggerations in the diagnosis and treatment of this disease, which need to be corrected.
há muitas dúvidas e poucas evidências para o diagnóstico e tratamento da doença do refluxo gastroesofágico (DRGE) na criança. A relação entre a DRGE e a alergia às proteínas do leite de vaca (APLV), o uso exagerado da ultrassonografia abdominal para diagnóstico da DRGE e o excesso de medicamentos, especialmente dos inibidores de bomba de prótons (IBP), são alguns aspectos que necessitam esclarecimentos. Esta revisão tem como objetivo estabelecer as evidências científicas atuais para o diagnóstico e tratamento da DRGE em pediatria.
Fontes dos dadosforam pesquisadas nas bases de dados eletrônicos do Medline, Pubmed, Lilacs, Cochrane Library e Scielo, nas diferentes faixas etárias da pediatria, até maio de 2013, as seguintes palavras-chave: refluxo gastroesofágico, doença do refluxo gastroesofágico, inibidores da bomba de prótons e procinéticos.
Síntese dos dadosa ultrassonografia de abdome não deve ser recomendada para pesquisa de refluxo gastroesofágico (RGE). O tratamento simultâneo da DRGE e da APLV induz, muitas vezes, ao uso desnecessário de medicação ou dieta de exclusão. Não existem evidências suficientes para prescrição de procinéticos em todos os portadores de RGE/DRGE. Poucas evidências fornecem suporte para a supressão ácida, no primeiro ano de vida, para tratamento de sintomas inespecíficos, sugestivos de DRGE. O tratamento conservador traz muitos benefícios e poucos gastos, sem efeitos colaterais.
Conclusõesexistem poucos estudos controlados e randomizados que avaliam a DRGE na criança e nenhum exame pode considerado padrão-ouro para o seu diagnóstico. Por esses motivos, ocorrem exageros no diagnóstico e no tratamento dessa doença, e que necessitam ser corrigidos.
Gastroesophageal reflux (GER) is a condition that most commonly affects the esophagus, and is one of the most frequent complaints in centers of pediatrics and pediatric gastroenterology.1–3
According to the latest guidelines from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN), published in 2009, GER is the passage of the gastric contents into the esophagus, with or without regurgitation and/or vomiting.1 It is a normal, physiological process, which occurs several times a day in infants, children, adolescents, and adults, when it causes few or no symptoms.1 Conversely, it may represent a pathological condition named gastroesophageal reflux disease (GERD), when it causes symptoms or complications that are associated with significant morbidity.1,3 These concepts were recently reinforced in April of 2013 by a new guideline that emphasizes important concepts for the general pediatrician.3
The variability of the clinical manifestations and outcome, the lack of a system that allows patient classification, and the lack of specific diagnostic tests, result in confusion regarding the diagnosis and treatment of GER and GERD in children. For this reason, definition of the basic concepts such as GER and GERD, as well as understanding regarding the different diagnostic methods and therapeutic options, are of utmost importance for the proper guidance of these patients. This is especially true because parents commonly seek pediatric care, as most infants regurgitate in the first months of life, which does not mean that they have the disease.2–4
The diagnosis of GERD is primarily clinical. In spite of the wide range of diagnostic tests available, none is considered as the gold standard.1,3,4 In infants with mild symptoms and no warning signs, drug therapy is unnecessary. These infants are considered “happy spitters” and therefore do not require any medical treatment. In infants and young children with GERD symptoms, non-pharmacological therapy may be the option of choice, due to lack of drugs with proven efficacy.3 In older children and adolescents, in whom symptoms are clearer and more specific, pharmacological treatment is more often used.1
The objective of this review was to establish the existing evidence in the scientific literature, in the light of current knowledge, on the diagnosis and treatment of GERD.
Diagnostic tests: clinical applicationConsidering that GER is a physiological process that occurs daily in all children, infants, adolescents and adults, it is difficult, in some situations, to differentiate this process from the pathological condition, i.e., GERD.1,5
Complementary examinations often do not clarify whether GER is physiological or pathological, as, to date, there are no well established standards for the diagnosis of GERD through definitive diagnostic methods. Significantly, the detection of reflux of gastric contents into the esophagus during an examination does not necessarily mean that the patient has GERD. Therefore, it is crucial to take into account the clinical history and physical examination. According to the latest consensus, the clinical history is enough to confirm the diagnosis in older children and adolescents, who have more specific GERD symptoms. In infants, symptoms are nonspecific (such as crying, irritability, and refusal to eat) and are insufficient to diagnose or predict response to therapy.1
There is a group of pediatric patients that has a higher risk of GERD, with greater severity, and chronic disease and its complications. They are the neurologically impaired, children with overweight and obesity, patients with genetic syndromes, those with operated esophageal atresia, those with chronic lung disease, and premature infants.1,3
Complementary examinations aim to document the presence of GER or its complications; to establish an association between GER and symptoms; to assess treatment effectiveness; and to exclude other conditions. As no diagnostic method can answer all these questions, it is essential to understand the usefulness and limitations of each of the diagnostic tests for adequate patient evaluation, as discussed below, to prevent submitting patients to invasive, expensive, and inappropriate tests.1,5,6
Contrast radiography of the esophagus, stomach and duodenumContrast radiography of the esophagus, stomach and duodenum is a low-cost, easy-to-perform examination, but it is not appropriate for diagnosis of GERD.1 It evaluates only the immediate postprandial GER, and it is unable to quantify the reflux episodes.2 Therefore, its routine use for the diagnosis of GERD1,4 is not justified. Its main role is the anatomical evaluation of the upper digestive tract,4 and should be indicated in selected patients.
Gastroesophageal scintigraphyAs with the radiological evaluation, gastroesophageal scintigraphy assesses only the immediate postprandial GER. Its advantages include the identification of GER even after a diet with neutral pH, gastric emptying evaluation, and detection of pulmonary aspiration.4 However, the detection of slow gastric emptying does not confirm GERD diagnosis and should be studied only in patients with clinical manifestations of gastric retention. Additionally, a normal test result does not exclude the possibility of pulmonary aspiration. Thus, this test should not be required for routine evaluation of GERD in infants and children.1,4
Esophagogastric ultrasoundEsophagogastric ultrasound (US) is not recommended for routine clinical evaluation of GERD in infants and older children, according to the recommendations of the consensus.1 When the results of the esophagogastric US are compared with those of the 24-hour esophageal pH-metry, the sensitivity is 95%, but the specificity is only 11% for the diagnosis of GERD, with no correlation between the frequency of reflux detected by color Doppler US and the reflux index detected by pH-metry.7 Esophagogastric US plays an important role in the differential diagnosis of hypertrophic pyloric stenosis, as the latter can be diagnosed through ultrasonographic evaluation.1
Recently, Savino et al8 published an article on the use of US for the diagnosis of GERD in pediatrics. This study established that the purposes of this examination in the evaluation of GERD are: to evaluate other causes of symptoms such as vomiting, apart from GERD; and to measure the abdominal esophageal length, the esophageal diameter and wall thickness, and the angle of His, providing functional and anatomical data.8 However, the authors emphasize the need to define diagnostic criteria, the standardization of tests, and reported measures.8
What is currently observed in clinical practice is that the esophagogastric US provides information on the presence and number of GER episodes during the examination. This information adds nothing to the investigation, because the reflux may be physiological, i.e., on a full stomach and in the supine position after the child has been fed. Therefore, the US, as it has been used, does not differentiate GER from GERD and is not helpful to the pediatrician and gastroenterologist diagnostic approach. Thus, at the moment, there is no place for US as a routine diagnostic test for GERD in pediatric patients.1,5
Esophageal pH-monitoringThe major advantages of pH-monitoring are: to evaluate the patient under more physiological conditions and for longer periods, to quantify GER, and to correlate episodes of reflux with signs and symptoms.9 Its main limitation is the incapacity to detect non-acid or weakly acidic reflux episodes.1,10,11 Thus, especially in infants who are predominantly or exclusively fed wit milk, postprandial GER may not be detected, due to the neutralization of acid reflux by milk.
According to the previous guidelines of the North American Society of Pediatric Gastroenterology, pH-metry should be performed only in situations that would provide changes in patient diagnosis, treatment, or prognosis.9 In this context, the main indications for GER assessment by pH-metry remain: evaluation of extra-digestive or atypical symptoms of GERD; detection of occult GER; evaluation of response to clinical treatment in patients with Barrett's esophagus or GERD that is difficult to control; and pre- and postoperative assessment of the patient with GERD.4,9,11
When symptoms are typical or when GERD has been diagnosed by other methods such as upper endoscopy, pH-monitoring is not indicated. pH-metry represents a valid quantitative measure of esophageal acid exposure, with well-established reference values.1,3 However, the severity of acid reflux is not consistently correlated with symptom severity or with demonstrable complications.1
Esophageal intraluminal impedanceThis is a new method that detects the retrograde movement of fluids, solids, and air in the esophagus, to any level and at any amount, regardless of pH, that is, regardless of chemical or physical characteristics, as it measures changes in electrical resistance and is performed with multiple channels. Therefore, this new technique may have greater value than pH-metry to monitor the quantity and quality of refluxed material.1,5,12
Currently, it is always used in association with pH monitoring (pH-multichannel intraluminal impedance – pH-MII).12,13 pH-MII is superior to pH monitoring alone to assess the temporal association between symptoms and GER.1 The two techniques used together provide useful measures, but they are yet to be well determined.1
Esophageal manometryEsophageal manometry assesses the motility of the esophagus and is indicated in those patients with symptoms suggestive of esophageal dysmotility, whose main symptoms are dysphagia and odynophagia.1 It may be useful in patients who have not responded to acid suppression and have a negative endoscopic findings in order to detect motor abnormalities such as achalasia the may mimic GERD.1 It can also be used to locate the lower esophageal sphincter (LES) in the pH-metry.
Upper gastrointestinal endoscopy with biopsyUpper gastrointestinal endoscopy allows direct visual examination of the esophageal mucosa and collection of samples for histophatological analysis.1,3 Thus, it is useful for the diagnosis of esophageal complications of GERD (esophagitis, peptic stricture, or Barrett's esophagus), which is important for the implementation of appropriate therapy and for patient prognosis.1–3,5 It also has a key role in the differential diagnosis with other peptic and nonpeptic diseases, such as eosinophilic esophagitis (EoE), fungal esophagitis, duodenal ulcer, gastritis by H. pylori, eosinophilic gastroenteropathy, malformations, and cancer, which can produce symptoms similar to GERD.1
Currently, reflux esophagitis is defined as the presence of mucosal lesions visible on endoscopy, in the esophagus, or immediately above the esophagogastric junction.1 Esophageal mucosa erythema and irregular Z line are not sensitive enough to diagnose reflux esophagitis. Similarly, the histological findings of mild eosinophilia, elongated papillae, basal layer hyperplasia, and dilation of intercellular spaces (spongiosis) are not adequate to make the diagnosis of reflux esophagitis.1 They only constitute nonspecific, reactive changes, which may be found in other types of esophagitis or even in normal subjects.1 Although the histological assessment of reflux esophagitis is not as important, endoscopic biopsies are essential in this group of patients for the differential diagnosis with other diseases, such as EoE.
It should also be considered that the absence of esophagitis on endoscopy does not exclude GERD, as some patients have endoscopy-negative reflux disease (non-erosive reflux disease [NERD]).
Empirical therapeutic test with acid suppressionOlder children and adolescents with typical symptoms of GERD, without warning signs, can be submitted to an empirical therapeutic trial with proton pump inhibitors (PPIs) for four weeks, which can be extended to 12 weeks if there is clinical improvement.1 Typical symptoms are heartburn, burning epigastric pain, chronic cough, especially related to food, nausea and regurgitation, chest pain, and dyspepsia. However, symptomatic improvement does not prove the presence of GERD, as symptoms may respond to placebo or improve spontaneously. The time of response is also controversial and varies from patient to patient. The warning signs that should be investigated are bleeding, weight loss, chronic anemia, asthenia, and prostration. There is no evidence to indicate a therapeutic test in younger children, in whom symptoms are less specific.1
GERD and cow's milk protein allergyGERD and cow's milk protein allergy (CMPA) are common conditions in pediatric patients, especially infants.14 There is currently a large number of infants who are treated concomitantly for GERD and CMPA. There is a subgroup of patients, in general, younger than 6 months, who have CMPA that manifest as vomiting and regurgitation, indistinguishable from GERD. In these infants, the elimination of cow's milk from the infant's or the mother's diet may improve vomiting substantially, and symptoms may recur when milk is reintroduced in the diet.1
The two conditions are difficult to diagnose, as there is a lack of a validated diagnostic test and they may be confused with many other conditions, from hunger to problems in the mother-infant relationship, physiological reflux, and adaptive problems of the digestive system, especially in infants whose symptoms are nonspecific, such as crying, irritability, and difficult sleeping. The simultaneous treatment of both conditions often causes exaggerations, frequently resulting in unnecessary pharmacological treatment or elimination diet.
Several studies support the hypothesis that there is a causal relationship between the two conditions, suggesting that there is a subgroup of infants in whom GERD is attributable to CMPA.14–19 The debate is the logical consequence of the fact that the two conditions require diagnostic examinations.14 Therefore, the consensus of the NASPGHAN/ESPGHAN1 on GERD advises a therapeutic trial of two to four weeks with an extensively hydrolyzed or amino acid formula, and for infants who are breastfed, with a maternal strict CMP elimination diet.1 In these cases, the possibility of GERD caused by CMPA would be excluded without using unnecessary medications. Conversely, the recent consensus on the diagnosis and treatment of food allergy of ESPGHAN states there are insufficient data to support the concept that gastroesophageal reflux may be the only manifestation of CMPA in breast-fed infants.20 This consensus statement, however, cites vomiting and regurgitation as possible symptoms of CMPA, and recommends elimination diet for the mother.20
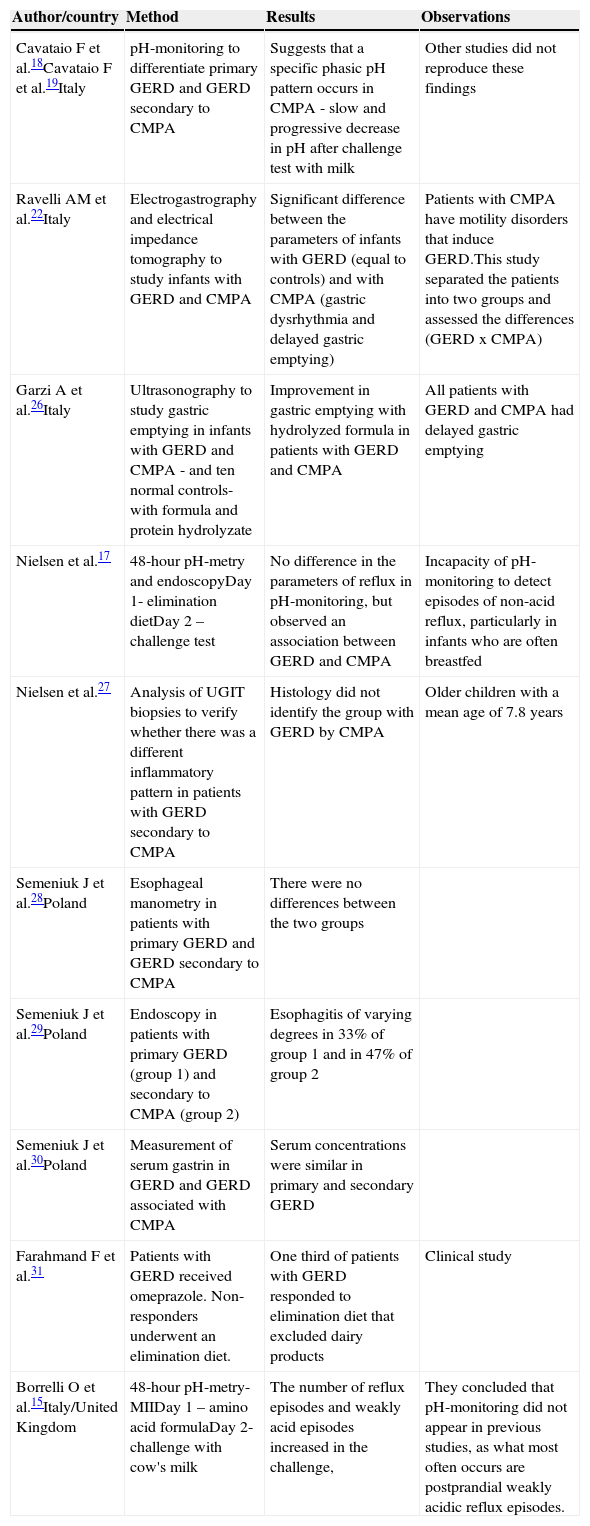
Although it has been estimated that the prevalence of GERD attributable to CMPA is as high as 56%, this association is not scientifically proven.14–17 There are several uncontrolled studies, with very different methodologies, aimed at clarifying the relationship between GERD and CMPA (Table 1).18,19 However, to date, this association remains unclear and there are still many points to be clarified.
Studies of the association between GERD and CMPA.
| Author/country | Method | Results | Observations |
|---|---|---|---|
| Cavataio F et al.18Cavataio F et al.19Italy | pH-monitoring to differentiate primary GERD and GERD secondary to CMPA | Suggests that a specific phasic pH pattern occurs in CMPA - slow and progressive decrease in pH after challenge test with milk | Other studies did not reproduce these findings |
| Ravelli AM et al.22Italy | Electrogastrography and electrical impedance tomography to study infants with GERD and CMPA | Significant difference between the parameters of infants with GERD (equal to controls) and with CMPA (gastric dysrhythmia and delayed gastric emptying) | Patients with CMPA have motility disorders that induce GERD.This study separated the patients into two groups and assessed the differences (GERD x CMPA) |
| Garzi A et al.26Italy | Ultrasonography to study gastric emptying in infants with GERD and CMPA - and ten normal controls-with formula and protein hydrolyzate | Improvement in gastric emptying with hydrolyzed formula in patients with GERD and CMPA | All patients with GERD and CMPA had delayed gastric emptying |
| Nielsen et al.17 | 48-hour pH-metry and endoscopyDay 1- elimination dietDay 2 – challenge test | No difference in the parameters of reflux in pH-monitoring, but observed an association between GERD and CMPA | Incapacity of pH-monitoring to detect episodes of non-acid reflux, particularly in infants who are often breastfed |
| Nielsen et al.27 | Analysis of UGIT biopsies to verify whether there was a different inflammatory pattern in patients with GERD secondary to CMPA | Histology did not identify the group with GERD by CMPA | Older children with a mean age of 7.8 years |
| Semeniuk J et al.28Poland | Esophageal manometry in patients with primary GERD and GERD secondary to CMPA | There were no differences between the two groups | |
| Semeniuk J et al.29Poland | Endoscopy in patients with primary GERD (group 1) and secondary to CMPA (group 2) | Esophagitis of varying degrees in 33% of group 1 and in 47% of group 2 | |
| Semeniuk J et al.30Poland | Measurement of serum gastrin in GERD and GERD associated with CMPA | Serum concentrations were similar in primary and secondary GERD | |
| Farahmand F et al.31 | Patients with GERD received omeprazole. Non-responders underwent an elimination diet. | One third of patients with GERD responded to elimination diet that excluded dairy products | Clinical study |
| Borrelli O et al.15Italy/United Kingdom | 48-hour pH-metry-MIIDay 1 – amino acid formulaDay 2- challenge with cow's milk | The number of reflux episodes and weakly acid episodes increased in the challenge, | They concluded that pH-monitoring did not appear in previous studies, as what most often occurs are postprandial weakly acidic reflux episodes. |
CMPA, cow's milk protein allergy; GERD, gastroesophageal reflux disease; UGIT, upper gastrointestinal tract.
Recently, Borrelli et al.15 evaluated a group of infants with CMPA and suspected GERD (17 children, mean age of 14 months), through 48-hour pH-impedance testing with multiple channels. In the first 24hours, they were treated with CMP elimination diet (amino acid formula, which they had already been receiving to treat CMPA); in the subsequent 24hours, a challenge test with cow's milk (cow's milk formula, with osmolarity and components other than the protein, similar to amino acid formula) was performed. These authors reported that in infants with CMPA and suspected GERD, exposure to cow's milk increased the number of weakly acidic reflux episodes, identifying a subgroup of patients with allergen-induced GER.15 Thus, they recommend pH-impedance testing as a diagnostic test for some cases of infants with GERD and CMPA.15 These data are not fully corroborated and should be interpreted with caution.
The mechanisms by which CMPA induces GER are still poorly understood.15 Data from animal models show neural abnormalities in gastrointestinal motility secondary to immediate hypersensitivity reactions, inducing delayed gastric emptying and changes in gastric acid secretion21 Other studies have shown changes in gastric myoelectric activity in atopic patients, when exposed to cow's milk.22,23 These changes would occur by activation and degranulation of mast cells and eosinophils, causing the release of cytokines and activation of receptors in nerve fibers of the digestive tract mucosa, which would result in contractile and motility abnormalities, triggering reflux episodes secondary to exposure to the antigen.14,15,21–23
Emerenziani and Sifrim,24 evaluating gastric emptying and pH-impedance testing of some patients, observed that the slower the gastric emptying, the higher the pH and proximal extension of reflux episodes. It is well established that non-acidic reflux episodes occur during feeding and in the first hours of the postprandial periods.15,23 Therefore, Borrelli et al.15 speculate that neuroimmune interactions, induced during the challenge test with cow's milk, suppress gastric acid production and alter the motor activity of the stomach, which slows gastric emptying and increases transient relaxation of the lower esophageal sphincter, resulting in an increase in the number of weakly acidic reflux episodes. This could explain how CMPA causes GERD, but it is yet to be proven.
Nevertheless, as these tests are still expensive and not widely available, in addition to being invasive for small infants, probably the most practical test in routine practice when there is doubt is a trial of CMP-elimination diet for two to four weeks in infants with GERD in whom CMPA is suspected.
The variety and availability of different formulas is another important issue in this discussion. The addition of nucleotides, long chain polyunsaturated fatty acids (LC-PUFAS), pre- and probiotics may improve immunity and decrease the incidence of gastrointestinal disorders including food allergies and motility disorders such as GERD and constipation. If the theoretical benefit proclaimed by pharmaceutical companies is real, it should result in clinical benefit, reducing the prevalence of these frequent gastrointestinal complaints; however, further studies are necessary to substantiate these effects,14 and the ESPGHAN and the American Academy of Pediatrics consensus state that there is not enough scientific support to routinely employ these additives in infant formulas.25
The studies that discuss the possible association between GERD and CMPA are shown in Table 1.15,17–19,22,26–31
GERD treatmentThe main objectives of therapy are to promote adequate growth and weight gain, symptom relief, healing of tissue injuries, and to prevent recurrence and complications associated with GERD.
Firstly, it is important to differentiate between physiological GER and GERD. In infants, GERD resolution occurs, in most cases, as the child grows and develops. Spontaneous resolution is common and the course is generally benign, with low incidence of complications. Thus, in this group, clinical treatment with anti-GERD measures, changes in diet and, less often, pharmacotherapy result in clinical resolution. A small percentage of young infants develop more severe pulmonary manifestations due to aspiration, cyanosis, and swallowing disorders, especially premature infants and those with cerebral palsy. Differently, in older children, as well as in adults, GERD has often a chronic and relapsing course, and may lead to complications. There may also be spontaneous resolution in this group.3,6
The decision to treat GERD is influenced by the probability of avoiding negative consequences for the child. The treatment should be implemented progressively, starting with general measures and changes in lifestyle, through drug therapies, and often ending in endoscopic or surgical techniques, which are more invasive.6 It is always essential in the initial consultation to explain to the parents why GER and GERD occur, reassuring and properly advising them, and to closely follow the evolution of the patient. Prolonged or repeated courses of drug treatment should not be prescribed prior to diagnostic confirmation.1
Conservative treatment (non-pharmacological)Recommendations offered to the parents and support to the family are essential measures, especially in small infants who vomit and present adequate growth.1 The lifestyle changes recommended to all pediatric patients with GER and GERD, regardless of severity, include: not wearing tight clothes; diaper changes before breastfeeding, to avoid using drugs that exacerbate GER; slow infusions in children with nasogastric tubes; and to avoid smoking (active or passive), as tobacco exposure induces LES relaxation, increases rates of asthma, pneumonia, apnea, and sudden infant death syndrome; in addition to anti-GER dietary and position guidelines,4 discussed in detail below.
Dietetic recommendationsAdolescents should avoid high-volume and high-calorie meals. Fatty foods are not recommended, as they may slow gastric emptying and reduce LES pressure.1,4 Some foods such as chocolate, soft drinks, tea, and coffee are not advisable. A simple and uncontroversial measure is to refrain from eating a few hours before bedtime, unless there is significant malnutrition. There is no evidence to support the routine elimination of certain foods for the treatment of GERD in older children,1 such as acidic fruit. The recommendation of smaller, more frequent meals is based on the likely correlation between gastric volume and the reflux index. However, this habit increases the frequency of postprandial periods, which are associated with greater number of weakly acidic or non-acid GER episodes.15
pH-monitoring and gastroesophageal scintigraphy studies have demonstrated that thickened feeds are not effective anti-GER measures, although they may decrease the volume and frequency of regurgitation and vomiting.1 While it reduces crying and increases caloric intake, excessive calorie intake is a potential problem of a thickened diet.1,3 Its therapeutic effect has not been determined in patients with GER that do not present vomiting or regurgitation.3 Anti-regurgitation formulas may reduce visible regurgitation, but do not result in measurable decrease in the frequency of reflux episodes.1 A meta-analysis has demonstrated that, in healthy children, thickened formulas are only moderately effective in the treatment of physiological GER.32
Position guidelinesThe prone position is proven to be the most effective anti-GER position.3 However, its association with sudden death in infants, as well as that of the lateral decubitus position, has generated much controversy regarding the best anti-GER position.1,3 Currently, it is recommended that normal infants or patients with GERD should sleep in the supine position, since the risk of sudden death is more important than the benefit brought by the anti-GER position.1,3 Elevating the headboard has been recommended, although not proven beneficial in controlled studies.1–4 The sitting or semi-sitting positions for infants below one year were also not shown to be an effective anti-GER position, due to the muscle tonus of infants.33
For adolescents and adults, it is likely that the best position is the left lateral decubitus position, with the headboard elevated.1,3
Pharmacological treatmentIn general, physiological GER should not be treated with medication, except for cases where the presence of GERD is evident. Pharmacological treatment is directed primarily to acid suppression. PPIs and H2 receptor antagonists effectively increase gastric pH and prevent acid reflux, which is harmful to the esophageal mucosa. However, currently, weakly or non-acid reflux are known to be frequent and to cause symptoms.14,15
There is no algorithm for the treatment of GERD in children that does not provokes discussion and controversy but the recommended drugs are:
- •
Contact antacids, recommended only as symptomatic drugs for sporadic symptoms or to decrease nocturnal acidity.1
- •
Prokinetics, which help to control symptoms, mainly vomiting and regurgitation.
- •
Medications that reduce acid secretion (histamine H2-receptor antagonists or PPIs), when symptoms such as retrosternal pain and heartburn, and/or complications, such as esophagitis, are associated with the presence of the acid in the esophagus or in other organs, such as respiratory tract.
The use of prokinetics is based on the fact that they increase LES tonus and improve esophageal clearance and gastric emptying. However, none of these medications was shown to be effective in decreasing the frequency of transient relaxation of the LES, the main physiopathological mechanism of GER. They are not effective in inducing healing of esophageal lesions and do not have a proven anti-GER effect, rather an anti-regurgitation effect. Thus, the prokinetic medications are often used in children who have a predominance of symptoms of motility abnormalities and who have more regurgitation than pain.
Currently, there is insufficient evidence for the routine use of prokinetics.1 Furthermore, the potential side effects of these drugs are more important than the benefits achieved by their use in the treatment of GERD.1
In daily practice, the use of prokinetics is always associated with antacids in the treatment of GERD. Based on these concepts, each medication has its precise indications, and there is no need and no plausible explanation to justify the indiscriminate use of two medications (prokinetics and acid secretion inhibitors) at the beginning of treatment.
MetoclopramideMetoclopramide improves gastric emptying and esophageal peristalsis, and increases the pressure in the LES, but the narrow margin between therapeutic and adverse effects on the CNS hinders its use in children with GERD. A meta-analysis of seven controlled studies showed that, in children aged 1 month to 2 years, metoclopramide reduces the daily symptoms of GER and GER index in pH-monitoring, but with significant adverse effects.33 The adverse effects of metoclopramide in infants and children include lethargy, irritability, gynecomastia, galactorrhea, and extrapyramidal reactions, which have been reported in 11% to 34% of patients.3,33
BromoprideThere are no controlled trials to support its use or prove its benefits. As bromopride has neurological side effects, such as extrapyramidal changes, it must not be indicated for the treatment of GERD.34 Bromopride is not mentioned in any of the pediatric guidelines.1,3
DomperidoneDomperidone is a prokinetic agent that increases the pressure in the LES and improves motility, but its use is limited in pediatrics given the lack of studies that have demonstrated its effectiveness. A recent systematic review of studies with domperidone identified only four controlled studies in pediatric patients, none of which showed any robust evidence of efficacy in pediatric GERD.1,3,35
Domperidone also causes occasional extrapyramidal side effects.1,35 One of the major side effects is increased irritability and colic in infants, which often worsens the clinical picture or further confuses the pediatrician. The simple action of stopping the use of domperidone in infants who are experiencing side effects of the medication can greatly improve patient symptoms. More recently, the occurrence of cardiovascular events associated with the use of domperidone, including QT prolongation and ventricular arrhythmia, has been demonstrated.36,37
Acid secretion inhibitorsHistamine H2-receptor antagonistsHistamine H2-receptor antagonists are drugs that reduce gastric acidity by inhibiting the histamine H2 receptors on gastric parietal cells. A dose of 5mg/kg of ranitidine increases the gastric pH for 9 to 10hours in infants.1 Gastric pH begins to increase within 30minutes, allowing its use for fast symptom relief.1 Doses of 5mg/kg of ranitidine, every 12hours; or of 3mg/kg, three times a day, have been recommended in children.2,38 According to Orenstein et al.,2 the therapeutic failure of these medications can be attributed to the small doses commonly used in clinical practice.
Studies have demontrated that H2 antagonists (cimetidine, ranitidine, famotidine) are more effective than placebo in relieving GERD symptoms and healing esophageal mucosal injury.1 The effectiveness of H2 blockers in healing erosive lesions is much higher in mild to moderate cases. PPIs are more effective in more severe injuries, even when compared to high doses of ranitidine.1
Regarding side effects of ranitidine, some infants may have headaches, drowsiness, head banging and other side effects which, if interpreted as persistent symptoms of GERD, could result in an inappropriate increase in dosage.1 Furthermore, tachyphylaxis or decrease in the response is a problem for its chronic use.
As ranitidine has a liquid formula, it should be used when necessary in infants. If no satisfactory response is attained, it would be more appropriate to evaluate other diagnostic possibilities before prescribing PPIs.
In infants with nonspecific symptoms such as crying and irritability, diagnostic tests for GERD do not contribute much to the investigation, unless it is a severe case or there are associated comorbidities, such as neurological disease or operated esophagus. The healthy infant that does not respond to conservative measures is unlikely to have GERD.
There is no evidence to justify empiric treatment with acid suppression in infants and young children, as GERD symptoms are less specific.1 Hence, these drugs should be indicated when the diagnosis of reflux esophagitis is established.1
PPIsPPIs are indicated in cases of erosive esophagitis, peptic stricture, or Barrett's esophagus, as well as in children that need a more effective blockade of acid secretion, for instance, in those with severe chronic respiratory disease or neurological problems.1 The differences between the PPIs appear to be very small, and presentation plays a critical role in their selection.
PPIs are superior to H2-receptor antagonists, both in ameliorating symptoms and healing lesions, and both are superior to placebo medication.1 In contrast with H2-blockers, the effect of PPIs does not decrease with chronic use. It maintains gastric pH > 4 for longer periods, and inhibits acid secretion induced by feeding, which are characteristics not presented by H2-blockers. Its potent acid suppression leads to a reduction of intragastric volume for 24hours, which facilitates gastric emptying and decreases reflux volume.1
The currently available PPIs are omeprazole, pantoprazole, esomeprazole, lansoprazole, rabeprazole and dexlansoprazole. They may cause four types of side effects in children: idiosyncratic reactions, interactions with other drugs, hypergastrinemia, and drug-induced hypochlorhydria.1 The idiosyncratic effects occur in approximately 14% of pediatric patients using PPIs:1 the most common are headache, diarrhea, constipation, and nausea, each of them occurs in approximately 2% to 7% of patients.1,3 Parietal cell hyperplasia and hyperplastic polyps of the gastric fundus are benign abnormalities caused by acid blocking and by hypergastrinemia.1 It should be considered that several studies have associated hypochlorhydria due to PPIs to community-acquired pneumonia, gastroenteritis, candidiasis, and even enterocolitis in preterm infants.1,39,40 In adults, they may cause acute interstitial nephritis.1 Moreover, PPIs may alter the patient's intestinal microbiota and some studies suggest that acid suppression may predispose to the development of food allergies.1,41
PPIs also have their limitations, as a consequence of their pharmacological properties. They must be used before the first meal,42 and must be protected from stomach acid by an enteric coating. A major problem of PPIs in Brazil is that there is no liquid formulation. Customized liquid formulations are not tested and therefore, their effectiveness is unknown. Opening the pill or crushing the tablet may inactivate the medication by removing the gastric acid protection, since PPIs need to be intact in order to be absorbed in the duodenum. Multiunit pellet system (MUPS) formulations, since they are soluble and contain a large number of individual microspheres with individual enteric protection, allow for the use of omeprazole and esomeprazole at any age and through a feeding tube, as it is possible to dilute the drug.42
Omeprazole may be used at doses ranging from 0.7 to 3.5mg/kg/day.1,42.43 The maximum dose used in children in published studies was 80mg/day, based on symptoms or esophageal pH-monitoring.43 The pharmacokinetics of omeprazole and other PPIs is not well established in children below 1 year of age.1,43 Extrapolating from adult data, it appears that PPIs may eventually be used, when necessary, as symptomatic drugs. PPIs are widely used in pediatrics, although scientific evidence for the use in this age group is limited.44,45
Long-term PPI administration is not advisable without a previous investigation.1 In cases where acid suppression is required, the minimum possible dose should be used. Most patients require a single daily dose. The routine use of twice daily dose is not indicated. Treatment discontinuation should be attempted whenever possible, as few patients will require long-term treatments.38,40
Hassall et al.,46 in a recent study, demonstrated that 62.5% of patients with erosive esophagitis who had a relapse and required chronic treatment with PPIs had a predisposing disease, such as neurological alterations or esophageal atresia. Only 33% of those who had no predisposing conditions to GERD required prolonged treatment.46
After prolonged use, the dose should be gradually reduced. In some patients, abrupt discontinuation of PPI treatment may cause a rebound effect on acid production, thus it is necessary to gradually wean the patient from the therapy.1 When PPIs are abruptly discontinued, the parietal cell mass that was blocked is released from its suppression and acid hypersecretion rebound occurs.47 This may cause symptom exacerbation, requiring more PPIs,47 an aspect demonstrated in a study of asymptomatic adults that received PPIs for three months and developed gastrointestinal symptoms when the medication was abruptly discontinued.48
Use and abuse of acid suppression therapy in pediatricsGER is a physiological process in most infants. Studies in normal infants have demonstrated reflux episodes as often as 73 times a day,49 with regurgitation associated with reflux episodes in 67% of children in the fourth month of life.50 For the great majority of infants (98%), GER symptoms improve up to 12 to 15 months of age, as the child develops, lower esophageal sphincter maturation occurs, solid food is introduced, muscle tone increases, and the baby spends more time in the upright position.51 In summary, GER symptoms are more common in young infants, with a peak at 4 months of age, and tend to disappear during the second half of the first year of life.50,52 Differently, GERD is not frequent in this age group.
The response of infants to different stimuli, including GER and GERD, are nonspecific and very similar, making it sometimes difficult to establish the cause of irritability or crying. Several studies have demonstrated that acid suppression does not control symptoms such as irritability, crying, and fussiness, which are interpreted as symptoms of GERD.53,54 There is also some evidence that placebo improves symptoms in infants as much as PPIs.53,54 In the largest double-blind, randomized, placebo-controlled trial in which infants with GERD symptoms received a PPI or placebo, the response was exactly the same in both groups. In this study out of the patients who received placebo, as well as those who received PPI (lansoprazole) for four weeks, 54% showed satisfactory response, but the group receiving the active medication had more side effects.53 A smaller placebo-controlled trial with a different PPI showed very similar findings.54
It must not be forgotten that cultural factors affect feeding practices, and studies have shown that infants with GERD should be evaluated in terms of feeding behavior related to maternal practices, problems, and beliefs.
Maternal aspects that must be evaluated are depression, anxiety, feeding problems, and impaired mother–child interaction.55,56 Maladaptive eating behaviors should also receive proper attention. Interventions may be needed before a negative reinforcement, including tests and medications, is created.55,56
According to some studies,38,40,57–59 there is an epidemic of overuse of PPIs in the first year of life in North America; this also appears to be the case in Brazil. A study of 575,000 prescriptions in the United States, demonstrated that the number of gastric acid-suppressing medications prescribed to children under 4 years of age increased 56% between 2002 and 2006.60 They estimated that 3% of all children in this age group were receiving some type of medication for acid suppression.60 The highest increase was among infants below 1 year of age. Another North American study observed an increase of more than seven-fold in PPI use between the years of 1999 and 2004, and the use of a liquid formulation for babies presented a 16-fold increase during this period.60
Reviewers of the Food and Drug Administration (FDA) in the United States published an article in the Journal of Pediatric Gastroenterology and Nutrition61 in January of 2012, reviewing the studies commissioned to the pharmaceutical industry on PPI use in the first year of life. According to these authors, the increase in prescriptions for PPIs in the first year of life was 11-fold between 2002 and 2009.61 They evaluated four randomized controlled trials and concluded that PPIs should not be administered to treat symptoms of GER in normal infants without solid evidence that acid is the cause of the symptoms.61 This article offers the following conclusions:
- •
Normal infants with symptoms of GER should be initially treated with conservative measures (dietary and postural guidelines), and evaluated for CMPA. Most of these infants improve with time and do not have acid-induced disease, and thus they do not benefit from PPIs. If conservative measures fail, and the investigation of another etiology is negative, the patient should be referred to a pediatric gastroenterologist.
- •
The use of PPIs should be reserved for infants with documented acid-induced disease, such as erosive esophagitis. Without proven evidence, the balance between risks and benefits of PPIs is not favorable in this age group, and the long-term effects of their use have not been studied.
- •
Short and long-term safety studies are limited.
- •
The diagnostic tests available and symptoms are not accurate enough to indicate treatment with PPIs in infants.
- •
More studies evaluating PPIs should be performed, especially in infants with erosive esophagitis, cystic fibrosis, short bowel, and extra-esophageal manifestations. In erosive esophagitis, efficacy can be extrapolated from other studies in adults and children.61
Therefore, the main concern with GERD management is related to infants, as presently there are no studies that demonstrate clear efficacy of PPIs for the treatment of nonspecific manifestations as crying and irritability.55,59 This exaggeration regarding the treatment of GERD in infants does not occur without potential adverse effects documented in the literature. Gastric acid is important for protection against infections and for the absorption of certain nutrients.38
Currently, there are very few randomized controlled trials providing support for the use of medications to treat symptoms consistent with GERD in the first year of life.62 However, a study with 1,245 American pediatricians observed that 82% of the respondents agreed that they would start empirical acid suppression before ordering diagnostic tests.63
In this context, the possible benefits of a non-pharmacological conservative treatment, with changes in diet and lifestyle, are important in order to not expose infants to unnecessary medications and to prevent adverse effects and costs.64 Shalaby et al.65 conducted a study in which a nurse, experienced in GER/GERD guidelines, advised parents of infants with suspected symptoms of GERD by telephone on conservative measures. These recommendations reduced symptoms in 26% of infants, thus avoiding the need for consultation with the gastroenterologist.65 Patients were instructed to use thickened and/or extensively hydrolyzed formula, or the mother was instructed to follow a CM and soy elimination diet, to avoid exposure to smoke, and to follow the position guidelines. After two weeks, 78% of patients improved, of whom 59% presented a decrease in at least five items of the symptom questionnaire, and 24% remained free of symptoms.65
Final considerationsInfants have nonspecific responses to different pathological and non-pathological stimuli: crying, irritability, refusal to eat, sleep disorders, back arching, and apparent discomfort.66 Pediatricians have less time to listen to parents and caregivers, rather than taking a complete history that includes behavioral and dietary details and reassuring them. Furthermore there is an additional pressure to “solve the problem” and “do something” which leads the pediatrician to choose the fast track: to prescribe!
It appears to be less risky, but it brings consequences for the patients, as it is less expensive to try a more conservative approach rather than prescribing several medications.67,68 In the light of current knowledge, it would be better to advise patients and their caregivers and to prescribe fewer medications.
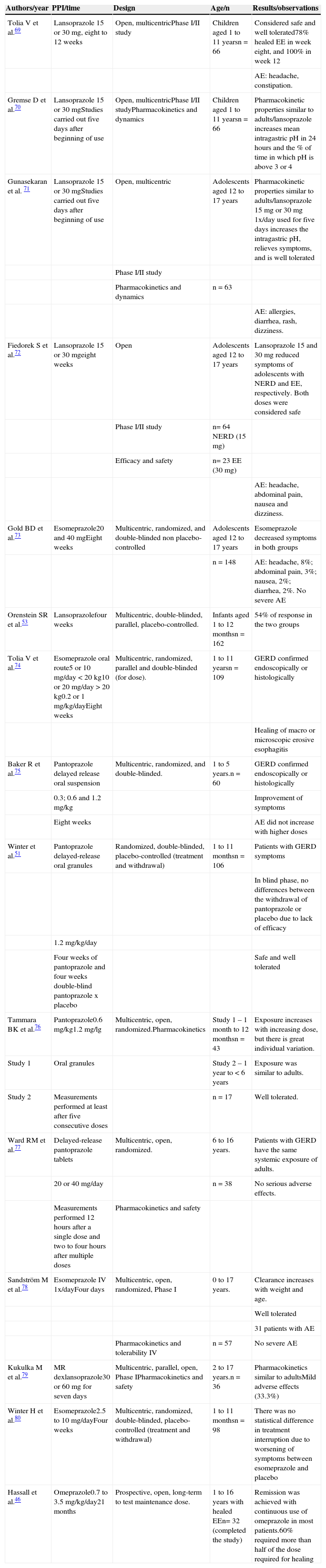
In patients with persistent symptoms, referral to a pediatric gastroenterologist is advised in order to assess the need of diagnostic investigations, and proper pharmacological or possible surgical treatment. Studies on PPI use in children are presented in Table 2.46,51,53,69–80
Studies with PPIs in pediatric GERD.
| Authors/year | PPI/time | Design | Age/n | Results/observations |
|---|---|---|---|---|
| Tolia V et al.69 | Lansoprazole 15 or 30mg, eight to 12 weeks | Open, multicentricPhase I/II study | Children aged 1 to 11 yearsn = 66 | Considered safe and well tolerated78% healed EE in week eight, and 100% in week 12 |
| AE: headache, constipation. | ||||
| Gremse D et al.70 | Lansoprazole 15 or 30mgStudies carried out five days after beginning of use | Open, multicentricPhase I/II studyPharmacokinetics and dynamics | Children aged 1 to 11 yearsn = 66 | Pharmacokinetic properties similar to adults/lansoprazole increases mean intragastric pH in 24hours and the % of time in which pH is above 3 or 4 |
| Gunasekaran et al. 71 | Lansoprazole 15 or 30 mgStudies carried out five days after beginning of use | Open, multicentric | Adolescents aged 12 to 17 years | Pharmacokinetic properties similar to adults/lansoprazole 15mg or 30mg 1x/day used for five days increases the intragastric pH, relieves symptoms, and is well tolerated |
| Phase I/II study | ||||
| Pharmacokinetics and dynamics | n = 63 | |||
| AE: allergies, diarrhea, rash, dizziness. | ||||
| Fiedorek S et al.72 | Lansoprazole 15 or 30 mgeight weeks | Open | Adolescents aged 12 to 17 years | Lansoprazole 15 and 30mg reduced symptoms of adolescents with NERD and EE, respectively. Both doses were considered safe |
| Phase I/II study | n= 64 NERD (15 mg) | |||
| Efficacy and safety | n= 23 EE (30 mg) | |||
| AE: headache, abdominal pain, nausea and dizziness. | ||||
| Gold BD et al.73 | Esomeprazole20 and 40 mgEight weeks | Multicentric, randomized, and double-blinded non placebo-controlled | Adolescents aged 12 to 17 years | Esomeprazole decreased symptoms in both groups |
| n = 148 | AE: headache, 8%; abdominal pain, 3%; nausea, 2%; diarrhea, 2%. No severe AE | |||
| Orenstein SR et al.53 | Lansoprazolefour weeks | Multicentric, double-blinded, parallel, placebo-controlled. | Infants aged 1 to 12 monthsn = 162 | 54% of response in the two groups |
| Tolia V et al.74 | Esomeprazole oral route5 or 10 mg/day < 20 kg10 or 20 mg/day > 20 kg0.2 or 1 mg/kg/dayEight weeks | Multicentric, randomized, parallel and double-blinded (for dose). | 1 to 11 yearsn = 109 | GERD confirmed endoscopically or histologically |
| Healing of macro or microscopic erosive esophagitis | ||||
| Baker R et al.75 | Pantoprazole delayed release oral suspension | Multicentric, randomized, and double-blinded. | 1 to 5 years.n = 60 | GERD confirmed endoscopically or histologically |
| 0.3; 0.6 and 1.2 mg/kg | Improvement of symptoms | |||
| Eight weeks | AE did not increase with higher doses | |||
| Winter et al.51 | Pantoprazole delayed-release oral granules | Randomized, double-blinded, placebo-controlled (treatment and withdrawal) | 1 to 11 monthsn = 106 | Patients with GERD symptoms |
| In blind phase, no differences between the withdrawal of pantoprazole or placebo due to lack of efficacy | ||||
| 1.2 mg/kg/day | ||||
| Four weeks of pantoprazole and four weeks double-blind pantoprazole x placebo | Safe and well tolerated | |||
| Tammara BK et al.76 | Pantoprazole0.6 mg/kg1.2 mg/lg | Multicentric, open, randomized.Pharmacokinetics | Study 1 – 1 month to 12 monthsn = 43 | Exposure increases with increasing dose, but there is great individual variation. |
| Study 1 | Oral granules | Study 2 – 1 year to < 6 years | Exposure was similar to adults. | |
| Study 2 | Measurements performed at least after five consecutive doses | n = 17 | Well tolerated. | |
| Ward RM et al.77 | Delayed-release pantoprazole tablets | Multicentric, open, randomized. | 6 to 16 years. | Patients with GERD have the same systemic exposure of adults. |
| 20 or 40 mg/day | n = 38 | No serious adverse effects. | ||
| Measurements performed 12hours after a single dose and two to four hours after multiple doses | Pharmacokinetics and safety | |||
| Sandström M et al.78 | Esomeprazole IV 1x/dayFour days | Multicentric, open, randomized, Phase I | 0 to 17 years. | Clearance increases with weight and age. |
| Well tolerated | ||||
| 31 patients with AE | ||||
| Pharmacokinetics and tolerability IV | n = 57 | No severe AE | ||
| Kukulka M et al.79 | MR dexlansoprazole30 or 60mg for seven days | Multicentric, parallel, open, Phase IPharmacokinetics and safety | 2 to 17 years.n = 36 | Pharmacokinetics similar to adultsMild adverse effects (33.3%) |
| Winter H et al.80 | Esomeprazole2.5 to 10 mg/dayFour weeks | Multicentric, randomized, double-blinded, placebo-controlled (treatment and withdrawal) | 1 to 11 monthsn = 98 | There was no statistical difference in treatment interruption due to worsening of symptoms between esomeprazole and placebo |
| Hassall et al.46 | Omeprazole0.7 to 3.5 mg/kg/day21 months | Prospective, open, long-term to test maintenance dose. | 1 to 16 years with healed EEn= 32 (completed the study) | Remission was achieved with continuous use of omeprazole in most patients.60% required more than half of the dose required for healing |
AE, adverse effect, EE, erosive esophagitis; GERD, gastroesophageal reflux disease; LRTI, lower respiratory tract infection; NERD, non-erosive reflux disease; PPIs, proton pump inhibitors.
All authors have received honoraria for educational activities organized by Support, Abbott, Danone, and Nestlé Nutrition.
Please cite this article as: Ferreira CT, Carvalho E, Sdepanian VL, Morais MB, Vieira MC, Silva LR. Gastroesophageal reflux disease: exaggerations, evidence and clinical practice. J Pediatr (Rio J). 2014;90:105–18.




