
To analyze the trend of hospitalizations for asthma in children and adolescents by region and age group in Brazil, from 2008 to 2017.
MethodThis is a time-series study with secondary data regarding hospitalizations for asthma in children and adolescents, according to age, region, and gender. Descriptive statistics procedures were used with measures of central tendency to calculate the variation between the periods of 2008 and 2017. Rates of hospitalizations were calculated specifically by age group and region. Time trend analysis was performed by simple linear regression, considered as stationary (p>0.05), declining (p<0.05 and negative regression coefficient), or ascending (p<0.05) and positive regression coefficient).
ResultsThe present study identified a higher proportion of hospitalizations for asthma in Brazil in children aged 5–9 years. Regarding gender, there were more hospitalizations in boys. The region that presented the highest proportion of hospitalizations, in all age groups investigated, was the Northeast. As for the trend analysis, this article showed that, in Brazil, there was a trend toward a reduction in hospitalization rates for asthma.
ConclusionIn Brazil, there was a tendency to reduce hospitalizations for all investigated age groups. The Northeast was the only region that showed a decline in all age groups.
Chronic respiratory diseases represent one of the most frequent pathologies in the world population. Among these, asthma is the most common, as it affects approximately 300 million people.1 It has a high morbidity rate and affects mainly children and adolescents, which results in high health care costs and school absenteeism.2
Due to its high prevalence in several developing countries, asthma has been recognized as a serious public health problem, being the target of interventions by public health policies.3 The forecast for the next ten years is that there will be an additional 100 million new cases in the world.1 Among the causes identified for the increased asthma burden, behavioral, genetic, and environmental factors stand out.4
Asthma is a chronic inflammatory disease caused by hyper responsiveness and obstruction of airflow in the airways, along with various physiological events in response to chemical and cellular mediators.5 Currently, it is classified as controlled, partially controlled, or uncontrolled, according to the frequency and intensity of symptoms. It is usually associated with airway hyperresponsiveness to direct or indirect stimuli. These characteristics usually persist even when symptoms are absent or lung function is normal, but they can normalize with treatment. Despite notable advances in the treatment and prevention of asthma, many countries do not have an optimistic outlook.1
Latin America has a high prevalence of asthma, with 40 million people with this diagnosis. Since most countries have serious problems with their health systems, there are high rates of exacerbations, with increased demand for emergency units and high rates of hospitalizations.2
In Brazil, asthma is now the fourth cause of hospitalization in the Unified Health System (Sistema Único de Saúde [SUS]), and among children and adolescents, it is characterized as the third cause. The number of hospitalizations for asthma is an important indicator of morbidity that has been decreasing in countries that have implemented asthma control plans.1 Asthma hospitalization rates have declined in the past decade. However, in many Brazilian capitals, high rates of hospitalization and re-admission still persist.6
Nonetheless, despite the data regarding hospitalizations being freely available in the Hospital Information System (SIH-SUS), hospitalizations of Brazilian children and adolescents are still poorly studied, especially regarding analysis of Brazilian regions. Thus, this study aims to analyze the trend of hospitalizations for asthma in children and adolescents by region and age group in Brazil, from 2008 to 2017.
MethodsThis is a time series study with secondary data referring to hospitalizations for asthma in children and adolescents, according to age group and region. Data were obtained through the SIH-SUS.
Population information for calculating hospitalization rates per 10,000 inhabitants was obtained from the Brazilian Institute of Geography and Statistics (IBGE), projected for 2020. Chapter X of the International Classification of Diseases (ICD-10), code J45.0 (Asthma) was considered for children and adolescents living in all Brazilian regions. The following variables were used for analysis: year, region, federative unit, date of birth, race/color, municipality of residence, sex, main asthma diagnosis according to the ICD-10 classification. Children were considered to be individuals with ages ranging from birth to 9 years of age. Adolescents were considered individuals between 10 and 19 years old.
The information for each month and the Federated Units (Unidades da Federação [UF]) was expanded from the database container (DBC) file to the database file (DBF) format in the Tabwin v. 3.4 program. Subsequently, the data were exported to the statistical package Stata v. 14 (Stata Corporation) in the DTA format. In the descriptive analysis, the percentage of hospitalization for asthma was calculated according to the years of hospitalization, region, sex, and race. The population was categorized into three age groups: 5–9 years, 10–14 years, and 15–19 years.
Descriptive statistics procedures (simple frequencies) were used, and the percentage variation between the periods of 2008 and 2017 was calculated. Hospitalization rates (asthma) were calculated, specifically by age group and region.
The temporal trend analysis was performed by simple linear regression, since the residues showed normal distribution. In the modeling process, the hospitalization rates for asthma were considered as a dependent variable (Y) and the years of hospitalization as the independent variable (X). The values of β, R-squared (R2), their 95% confidence intervals, and their respective p-values were presented. The trend analysis of was performed by region and age group, considered as stationary (p>0.05), declining (p<0.05 and negative regression coefficient), or ascending (p<0.05 and positive regression coefficient).
As there are no ethical or moral implications for the use of secondary and grouped data, available in the public domain on the official website of the Ministry of Health in which there is no information that identifies individuals, the present study was not referred to the Ethics Committee.
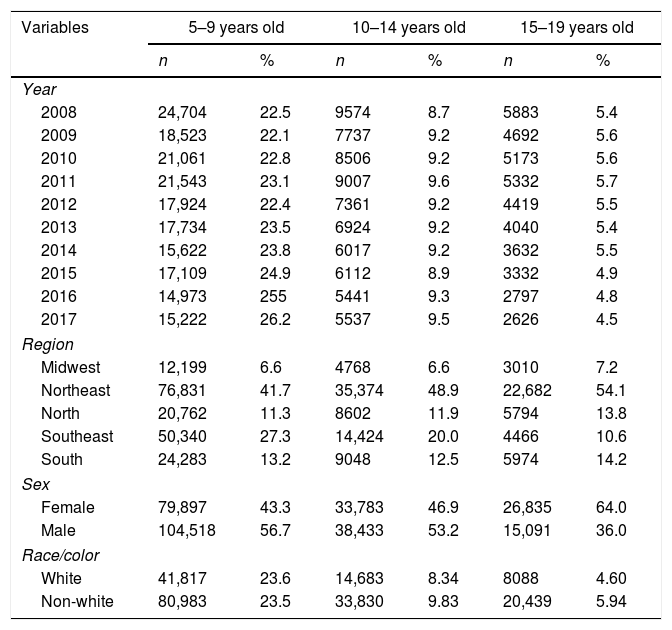
ResultsIn Brazil, 785,477 hospitalizations for asthma in children and adolescents were recorded between 2008 and 2017. Table 1 shows the characteristics of hospitalizations for asthma in children and adolescents. In relation to the years studied, it is observed that the proportion of hospitalizations was higher in children aged 5–9 years in 2008. The male gender presented a higher percentage of hospitalization, with about 56.7% in the age group of 5–9 years. The Northeast region had the highest distribution and the Midwest region had the lowest proportion.
Absolute number and percentage of hospitalizations for asthma according to year, age group, region, and sex. Brazil, 2008–2017.
| Variables | 5–9 years old | 10–14 years old | 15–19 years old | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Year | ||||||
| 2008 | 24,704 | 22.5 | 9574 | 8.7 | 5883 | 5.4 |
| 2009 | 18,523 | 22.1 | 7737 | 9.2 | 4692 | 5.6 |
| 2010 | 21,061 | 22.8 | 8506 | 9.2 | 5173 | 5.6 |
| 2011 | 21,543 | 23.1 | 9007 | 9.6 | 5332 | 5.7 |
| 2012 | 17,924 | 22.4 | 7361 | 9.2 | 4419 | 5.5 |
| 2013 | 17,734 | 23.5 | 6924 | 9.2 | 4040 | 5.4 |
| 2014 | 15,622 | 23.8 | 6017 | 9.2 | 3632 | 5.5 |
| 2015 | 17,109 | 24.9 | 6112 | 8.9 | 3332 | 4.9 |
| 2016 | 14,973 | 255 | 5441 | 9.3 | 2797 | 4.8 |
| 2017 | 15,222 | 26.2 | 5537 | 9.5 | 2626 | 4.5 |
| Region | ||||||
| Midwest | 12,199 | 6.6 | 4768 | 6.6 | 3010 | 7.2 |
| Northeast | 76,831 | 41.7 | 35,374 | 48.9 | 22,682 | 54.1 |
| North | 20,762 | 11.3 | 8602 | 11.9 | 5794 | 13.8 |
| Southeast | 50,340 | 27.3 | 14,424 | 20.0 | 4466 | 10.6 |
| South | 24,283 | 13.2 | 9048 | 12.5 | 5974 | 14.2 |
| Sex | ||||||
| Female | 79,897 | 43.3 | 33,783 | 46.9 | 26,835 | 64.0 |
| Male | 104,518 | 56.7 | 38,433 | 53.2 | 15,091 | 36.0 |
| Race/color | ||||||
| White | 41,817 | 23.6 | 14,683 | 8.34 | 8088 | 4.60 |
| Non-white | 80,983 | 23.5 | 33,830 | 9.83 | 20,439 | 5.94 |
Data source: Sistema de Internações Hospitalares (SIH-SUS).
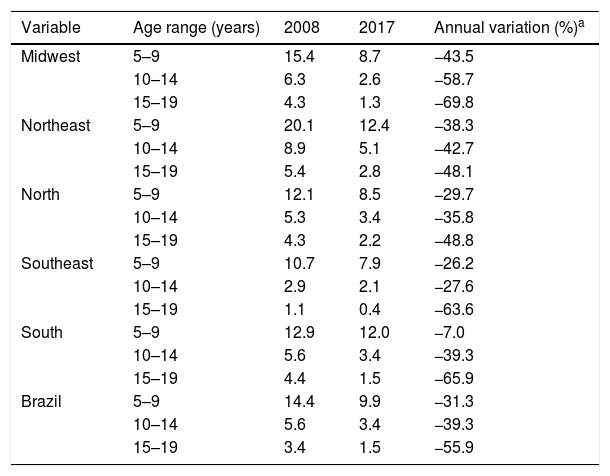
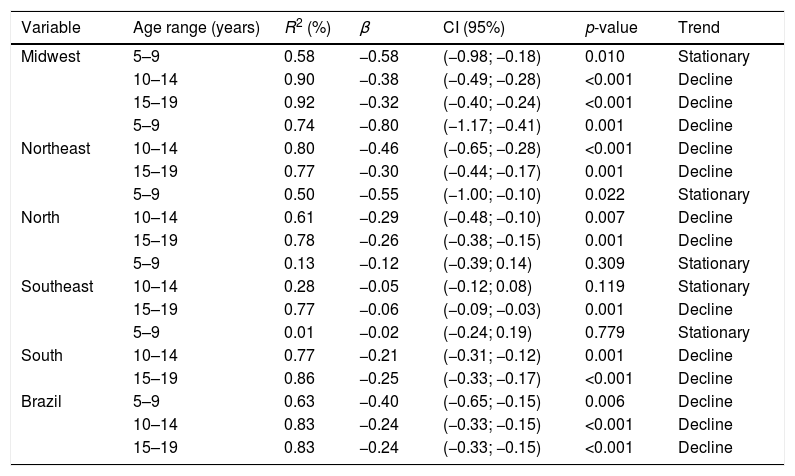
From 2008 to 2017 there was a decrease in the hospitalization rate in all regions and age groups investigated. Table 2 shows the rates of hospitalizations for asthma and the annual percentage change. In all regions and age groups, there is a reduction in hospitalization rates for asthma, with an emphasis on the 15–19 age group in the Midwest region (−69.7%), and the 5–9 age group in the South (−7.7%). The annual percentage variation of each region showed similarities when compared to the total values in Brazil. Table 3 shows the data related to the analysis of the trend of hospitalizations for asthma, according to regions and age group.
Hospitalization rate and annual percentage variation of asthma according to region and age group. Brazil, 2008–2017.
| Variable | Age range (years) | 2008 | 2017 | Annual variation (%)a |
|---|---|---|---|---|
| Midwest | 5–9 | 15.4 | 8.7 | −43.5 |
| 10–14 | 6.3 | 2.6 | −58.7 | |
| 15–19 | 4.3 | 1.3 | −69.8 | |
| Northeast | 5–9 | 20.1 | 12.4 | −38.3 |
| 10–14 | 8.9 | 5.1 | −42.7 | |
| 15–19 | 5.4 | 2.8 | −48.1 | |
| North | 5–9 | 12.1 | 8.5 | −29.7 |
| 10–14 | 5.3 | 3.4 | −35.8 | |
| 15–19 | 4.3 | 2.2 | −48.8 | |
| Southeast | 5–9 | 10.7 | 7.9 | −26.2 |
| 10–14 | 2.9 | 2.1 | −27.6 | |
| 15–19 | 1.1 | 0.4 | −63.6 | |
| South | 5–9 | 12.9 | 12.0 | −7.0 |
| 10–14 | 5.6 | 3.4 | −39.3 | |
| 15–19 | 4.4 | 1.5 | −65.9 | |
| Brazil | 5–9 | 14.4 | 9.9 | −31.3 |
| 10–14 | 5.6 | 3.4 | −39.3 | |
| 15–19 | 3.4 | 1.5 | −55.9 |
Trend analysis of hospitalizations for asthma according to region and age group. Brazil, 2008–2017.
| Variable | Age range (years) | R2 (%) | β | CI (95%) | p-value | Trend |
|---|---|---|---|---|---|---|
| Midwest | 5–9 | 0.58 | −0.58 | (−0.98; −0.18) | 0.010 | Stationary |
| 10–14 | 0.90 | −0.38 | (−0.49; −0.28) | <0.001 | Decline | |
| 15–19 | 0.92 | −0.32 | (−0.40; −0.24) | <0.001 | Decline | |
| 5–9 | 0.74 | −0.80 | (−1.17; −0.41) | 0.001 | Decline | |
| Northeast | 10–14 | 0.80 | −0.46 | (−0.65; −0.28) | <0.001 | Decline |
| 15–19 | 0.77 | −0.30 | (−0.44; −0.17) | 0.001 | Decline | |
| 5–9 | 0.50 | −0.55 | (−1.00; −0.10) | 0.022 | Stationary | |
| North | 10–14 | 0.61 | −0.29 | (−0.48; −0.10) | 0.007 | Decline |
| 15–19 | 0.78 | −0.26 | (−0.38; −0.15) | 0.001 | Decline | |
| 5–9 | 0.13 | −0.12 | (−0.39; 0.14) | 0.309 | Stationary | |
| Southeast | 10–14 | 0.28 | −0.05 | (−0.12; 0.08) | 0.119 | Stationary |
| 15–19 | 0.77 | −0.06 | (−0.09; −0.03) | 0.001 | Decline | |
| 5–9 | 0.01 | −0.02 | (−0.24; 0.19) | 0.779 | Stationary | |
| South | 10–14 | 0.77 | −0.21 | (−0.31; −0.12) | 0.001 | Decline |
| 15–19 | 0.86 | −0.25 | (−0.33; −0.17) | <0.001 | Decline | |
| Brazil | 5–9 | 0.63 | −0.40 | (−0.65; −0.15) | 0.006 | Decline |
| 10–14 | 0.83 | −0.24 | (−0.33; −0.15) | <0.001 | Decline | |
| 15–19 | 0.83 | −0.24 | (−0.33; −0.15) | <0.001 | Decline |
CI, confidence interval; R2, determination coefficient.
The descriptive results of this study showed that children under 9 years had a higher proportion of hospitalization than other age groups. Other studies conducted in several Brazilian regions have shown similar data.7,8 In Belo Horizonte, a municipality located in the southeastern region of Brazil, hospitalization occurred more frequently in this age group, and among boys.8
Studies show an association between influenza and hospitalizations for asthma in pediatric patients,9–13 with the influenza virus being the most commonly found in asthma patients admitted to the United States.14 The National Immunization Program and the Centers for Disease Control and Prevention recommend the influenza vaccine for children with asthma older than six months15,16 and the advancement of Brazilian public policies has shown that improving surveillance and prevention with the introduction of pneumococcal and influenza vaccines contributed to the reduction of hospitalizations for asthma in children.7,17
A higher frequency of asthma was identified in boys. Other studies on asthma confirm the findings of this study.13,18–20 One reason for this greater susceptibility to asthma in males can be explained by the anatomical difference in the airways, which have a smaller diameter in males.21 Similar to the findings of this study, other studies have shown an association between asthma and the female gender in adolescence.22,23 Some factors interfere with the higher occurrence of asthma among adolescent girls, such as psychosocial, environmental, and hormonal changes.23,24
In Brazil, the trend analysis of hospitalizations for asthma in childhood and adolescence, over the ten years of study, showed a decline. As for the regions, the Northeast showed a significant decline in all age groups. The Midwest, North, Southeast, and South regions showed a decreasing trend in hospitalizations for asthma; however, there was a stationary trend in the age group of 5–9 years. In the Southeast region there was also a stationary trend in the 10–14 age group.
Despite the decline in hospitalizations for asthma, the Northeast of Brazil was the region with the highest proportion of hospitalizations for asthma. This region has three types of climate (tropical, semi-arid, and humid equatorial). It is characterized by drought, marked by an intense summer with high temperatures, and periods of very irregular rain.20 It is also a region known for populations with lower family income who live in poor urban areas, with poor housing conditions, and who use wood stoves, which can be a trigger for asthma exacerbation crises. Studies indicate that hospitalizations for asthma in children and adolescents are more frequent in regions with serious vulnerabilities and social disparities.1,7,25 In addition, another factor that favors the highest number of hospitalizations for asthma is the geographical location of the Northeast, since regions close to the equator have greater episodes of asthma exacerbations.26 Another possible explanation for the number of hospitalizations for asthma in the Northeast may be the greater access and use of health services. In this region, there has been an expansion of FHS and expansion of primary care services. In 2016, eight out of ten residents in the Northeast were covered by the FHS.27
The Southeast region showed a decline in hospitalizations for asthma in the 15–19 age group but showed an important proportion of hospitalizations. In Brazil, this is one of the regions with the most populous cities and with a high concentration of industries that emit great quantities of environmental pollutants. A study conducted in Hong Kong showed an association between hospitalizations for asthma and places that have a high concentration of pollutants.15 Another factor that draws attention is the increase in rural-urban migration and the growing urbanization of this region of Brazil, which could increase asthma cases.28
Despite the trend results of this study that point to a decline in hospitalizations for asthma in the Midwest region and a lower proportion of hospitalizations for asthma in relation to other regions, there is a high prevalence of asthma in children and adolescents.29 The predominant biome in this region is the cerrado, which is characterized by a dry season (low humidity and hot) and a rainy season (high humidity and hot). During the period of high humidity, there is a greater growth of mold spores, while the low relative humidity of the air (<30%) in the dry period can cause difficulties in the functioning of the airways. This region also presents high levels of pollution due to the burning of sugarcane.30 Thus, these conditions cause breathing problems, including asthma.
Concerning the South, hospitalization rates are still high, but have shown a significant drop. A study carried out in Porto Alegre showed that 44.5% of asthma cases are not controlled, and this fact is associated with climatic conditions.26 The climate of this region presents temperatures that are generally the lowest in the country. It has a subtropical climate, high thermal amplitude in some points like the mountains, and temperatures below zero. However, a study that evaluated the performance of the Family Health Strategy in the South region pointed out that the FHS program's actions were more appropriate in the South than in other Brazilian regions.28
In Brazil, some factors have contributed to the decrease in hospitalization rates for asthma, such as improving the diagnosis of asthma, the implementation of asthma control plans, and compensatory policies, such as the Bolsa Família Program. The National Asthma Control Plan (PNCA), created in 1999, enabled better management of the disease and trained health professionals, with an emphasis on basic units, mainly in the Family Health Strategy.28
With the creation of the Popular Pharmacy Program (PFP) in 2004, the SUS started to make free inhaled corticosteroids available, which contributed to the reduction of severe asthma cases.8 Another measure adopted in 2012 was the Brasil Carinhoso Program, which provided for the free distribution of three drugs for the treatment of asthma (ipratropium bromide, beclomethasone, and salbutamol). In addition, the positive impact on vaccination coverage helped to reduce hospitalizations for conditions sensitive to primary care.7,12,18
In 2008, the Ministry of Health launched the Brazilian List of Hospitalizations for Conditions Sensitive to Primary Care. Among the group of respiratory causes is asthma. This means that this is a condition that can be diagnosed and treated in primary care, reducing morbidity and the number of hospitalizations. Studies investigating the Brazilian List of Hospitalizations for Conditions Sensitive to Primary Care show a significant decrease in hospitalization rates in some disease groups, with an emphasis on asthma.18,20
Some researchers have shown an association between increased coverage of the Family Health Strategy and reduced hospitalizations for conditions sensitive to primary care.26 Research carried out in Espírito Santo, with the aim of describing hospitalizations for conditions sensitive to primary care, identified that there was a reduction in the rates of these hospitalizations as the coverage rate of the Family Health Strategy increased 8.0% between 2000 and 2014).28
This study has some limitations. It was not possible to identify asthma severity, as a secondary database was used. However, it should be noted that most hospitalizations for asthma are severe cases. The data referring to hospitalizations for asthma can be duplicated, since the same child ages several times, which can cause an overestimation of the prevalence of the disease. Other important factors are the underreported cases of asthma that may constitute a possible information bias. In addition, there are possible limitations in the diagnosis of asthma and inaccurate data in completing the AIH. However, currently, information systems have been used as important tools to measure the quality of public health in Brazil.
The present study identified a higher proportion of hospitalizations for asthma in Brazil in children aged 5–9 years. Regarding gender, there were more hospitalizations in boys, except in the 15–19 age group. Regarding race/color, most hospitalized children were white, while in adolescence more hospitalizations were observed in non-whites. The region with the highest proportion of hospitalizations for asthma, in all age groups, was the Northeast of Brazil. As for the analysis of trends, in Brazil there was a reduction in hospitalization rates for asthma in most age groups and regions investigated.
However, hospitalization rates in Brazilian regions are still high, and considering it is a disease sensitive to management by primary care, hospitalizations for illness are considered preventable, suggesting the need of more resolute actions in public health, especially in the context of primary care.
FundingThe author Larissa Silva Magalhães received a master's scholarship of the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
Conflicts of interestThe authors declare no conflicts of interest.




