

To analyze the follow-up, in specialized outpatient clinics, of infants reported with congenital syphilis during the penicillin shortage.
MethodA cross-sectional study was carried out in ten public maternity hospitals affiliated with the Brazilian Unified Health System in the city of Fortaleza, state of Ceará. Clinical records of infants reported with congenital syphilis who were born alive in 2015 were used to describe correlates of attendance at recommended clinical follow-up appointments.
ResultsA total of 469 infants reported with CS from January 1/2015 to December 31/2015 were included in the analysis. The results show that most infants did not attend the follow-up visits (368/469, 78.5%) and the main associated factors are that the follow-up clinic is located in a different hospital from that where the infant was born (OR: 3.7; CI: 2.20–6.22; p < 0.001) and the use of illicit drugs by the mother (OR: 3.2; CI: 1.57–6.87; p = 0.002). Only 33.7% (34/101) were followed until discharge.
ConclusionThe majority of infants with reported congenital syphilis during this period did not attend the follow-up visits. Public health efforts aimed at reaching the parents of infants with CS should be a priority to ensure appropriate clinical identification and management of the associated outcomes of this vertically transmitted infection.
The elimination of Congenital Syphilis (CS) as a public health problem has been proposed by national and international institutions for years1; however, this condition remains an important challenge, considering the high incidence rates, especially in poor and developing countries.2
Brazil and other countries faced a serious problem of penicillin shortage in 2015, which is why many infants whose mothers had syphilis during pregnancy were not treated or received drugs other than penicillin,3 whose effectiveness for the treatment of CS is not proven. In the same year, approximately 22,800 cases of CS were recorded in 37 countries in the Americas, with an incidence rate of 1.7 cases per 1,000 live births. Brazil contributed considerably to the increase in this rate, having reported 19,228 cases, with an incidence rate of 6.5 cases per 1,000 live births, much higher than that recommended by the World Health Organization, which is less than 0.5 cases per 1,000 live births.2
In 2015, the Brazilian Ministry of Health (MOH) still did not clearly specify the level of care in which infants with CS should be monitored, leaving this decision up to the states and municipalities, which usually referred them to specialized outpatient clinics. The concern with CS control is mainly related to the consequences of the infection for the newborn. Although most infants are asymptomatic at birth, clinical manifestations can appear up to two years of age, which constitutes early CS, or after this age range, as late CS. Symptoms are usually associated with dermatological, bone, ophthalmological, auditory, neurological, and dental disorders, in addition to laboratory alterations.4–6
As the clinical manifestations of CS can occur after the neonatal period, it is necessary that even when treated in the maternity ward, the infant be referred to and have outpatient follow-up ensured until 18 months of age, when a non-treponemal test, investigation of signs and symptoms compatible with CS, ophthalmological, neurological and audiological assessments are performed.6
The clinical follow-up of infants with CS is dependent on both referral and counter-referral networks. Communication between the maternity hospitals and the outpatient clinics is essential to guarantee the planning of care for the referred infants. In fact, the problem is even more serious, as many infants are not even referred for follow-up at the time of discharge from the maternity hospital, a fact corroborated by a study carried out in the state of Minas Gerais, which found that 79% of infants with CS were not referred for follow-up.7 Additionally, even among the referred ones, many do not complete the recommended appointment schedule, a situation disclosed by a study carried out in the municipality of Porto Alegre, state of Rio Grande do Sul, Brazil, which analyzed the follow-up of infants with CS for a period of five years and identified a loss to follow-up rate of 50%.4
Therefore, this study aims to analyze the follow-up, in specialized outpatient clinics, of infants reported with CS in the city of Fortaleza during the penicillin shortage period.
The municipality of Fortaleza is located in the Northeast region of Brazil and has a population of 2,687,000 inhabitants.8 In the year these infants were notified, the incidence rate of CS in the municipality was 17.8 cases per 1000 live births.9
MethodThis was a cross-sectional study, carried out in specialized outpatient clinics for the follow-up of infants with CS in Fortaleza, located in the same maternity hospital where the infant was born or in another hospital service. The city of Fortaleza Municipal Health Secretariat defined a flow of referrals of infants with CS to these outpatient clinics, as shown in Figure 1.

Maternity hospitals and respective follow-up outpatient clinics for the referral of infants with CS. MEAC, Maternidade Escola Assis Chateaubriand; HGCC, Hospital Geral César Calls; HMZA, Hospital e Maternidade Zilda Arns; HGF, Hospital Geral de Fortaleza; HNSC, Hospital Nossa Senhora da Conceição; HGMM, Hospital Gonzaga Mota de Messejana; HGMJW, Hospital Gonzaga Mota do José Walter; HGMB, Hospital Gonzaga Mota da Barra do Ceará; HJMA, Hospital José Martiniano de Alencar.
The CS cases were notified by the Health System in the maternity hospital at the time of birth, according to the criteria recommended by the MOH.10 The infants were included in the analysis if the definition of CS was met as follows:
- •
A child whose mother had, during prenatal care or at the time of the delivery, a reactive non-treponemal syphilis test with any titration and a reactive treponemal test, and who was not treated or received inadequate treatment.
- •
A child whose mother was not diagnosed with syphilis during pregnancy and, if the maternity hospital was not able to perform the treponemal test, had a reactive non-treponemal test with any titration at the time of delivery.
- •
A child whose mother was not diagnosed with syphilis during pregnancy and, if the maternity hospital was not able to perform the non-treponemal test, had a reactive treponemal test at the time of delivery.
- •
A child whose mother had a reactive treponemal test and a non-reactive non-treponemal test at the time of delivery, with no record of previous treatment.
Infants with comorbidities were excluded due to the possibility of interference with the assessment of the clinical manifestations of CS. Those with medical records that could not be located were excluded, as well as those residing outside Fortaleza. Neonatal deaths were also excluded.
Data collection took place from January to December 2018, from the medical records of the infants in the aforementioned outpatient clinics. The variables collected about the child's follow-up were: the place where the child was referred to (maternity ward or outpatient clinic of another service), whether they attended the appointment, number of appointments, age of the child at the beginning and at the end of the follow-up, whether the recommended tests were performed and their results, observed clinical manifestations and complications, whether syphilis retreatment was necessary and whether they were discharged from follow-up. The evaluated outcome was discharged, considered when two consecutive negative VDRL (Venereal Disease Research Laboratory) tests were identified, regardless of the age at which the child initiated the serological follow-up.
Considering that the mother's sociodemographic profile, as well as the quality of prenatal care and the child's birth conditions, can interfere with follow-up attendance, these data were included in the analysis and collected from the notification forms and the mother and newborns’ medical records. The following variables were collected from the mother's record: age, marital status, level of schooling, whether they had paid work, use of illicit drugs, whether they attended prenatal care, number of prenatal care appointments, time of syphilis diagnosis, whether they were treated for syphilis during prenatal care. The following variables were collected from the newborn's record: whether VDRL was performed, VDRL result, VDRL titration, the clinical manifestation of CS (prematurity, low birth weight, hepatomegaly with or without splenomegaly, skin lesions, jaundice with level of phototherapy, serosanguineous rhinitis or pseudoparalysis of the limbs) and the treatment provided in the maternity ward.
The data were entered and analyzed using the SPSS statistical program (Statistical Package for the Social Sciences), version 22. A descriptive analysis was performed using frequency distribution for categorical variables and the calculation of means and standard deviations for numerical variables. For the bivariate analysis, Pearson's χ2 test and Fisher's exact test were used, with a significance level of 5% and a confidence interval of 95%.
Multiple logistic regression analysis was performed using the STATA statistical package, version 10.0, using the stepwise technique. For the adjusted analysis, variables that had a p value < 0.20 were included and those with a p value < 0.05 remained. The odds ratio (OR) was used as a measure of effect size, with a confidence interval of 95%.
This study was approved by the Ethics and Research Committee of the University of Fortaleza and by the Ethics and Research Committee of each maternity hospital.
ResultsIn 2015, 575 infants notified with CS were born alive in the city of Fortaleza, Ceará. Forty-three infants were excluded because it was not possible to locate their medical records or the notification form, 26 because they did not live in the city of Fortaleza, and 28 because they had comorbidities (HIV, hepatitis B and C, toxoplasmosis, rubella, cytomegalovirus, congenital virus infection, herpes simplex and Zika virus infection). Therefore, 469 cases were considered eligible for this study. All these infants were born to mothers who were untreated or inadequately treated for syphilis during prenatal care.
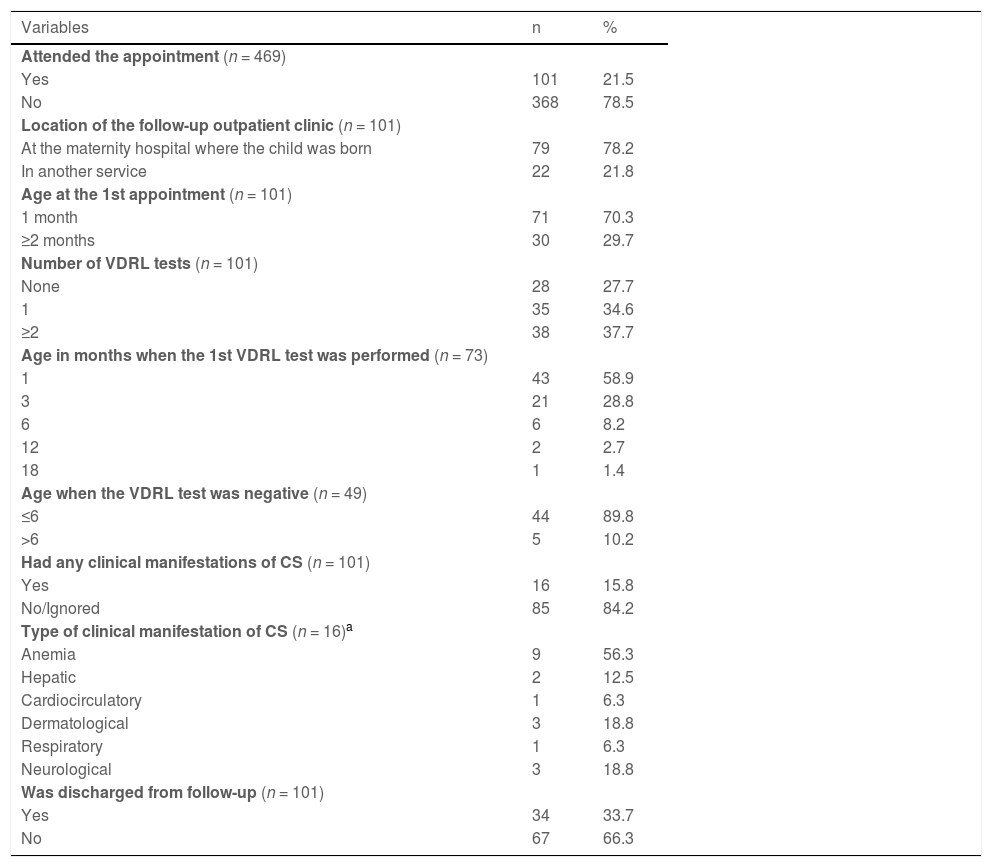
Table 1 shows the data related to the follow-up of infants with CS in specialized outpatient clinics. Of the 469 notified cases, 101 (21.5%) attended at least one appointment. Seventy-nine cases (78.2%) underwent follow-up in the same maternity hospital where they were born, and 22 (21.8%) in outpatient clinics located in other hospital services.
Follow-up data of infants reported with congenital syphilis in referral outpatient clinics. Fortaleza, Ceará, 2015–2017.
| Variables | n | % |
|---|---|---|
| Attended the appointment (n = 469) | ||
| Yes | 101 | 21.5 |
| No | 368 | 78.5 |
| Location of the follow-up outpatient clinic (n = 101) | ||
| At the maternity hospital where the child was born | 79 | 78.2 |
| In another service | 22 | 21.8 |
| Age at the 1st appointment (n = 101) | ||
| 1 month | 71 | 70.3 |
| ≥2 months | 30 | 29.7 |
| Number of VDRL tests (n = 101) | ||
| None | 28 | 27.7 |
| 1 | 35 | 34.6 |
| ≥2 | 38 | 37.7 |
| Age in months when the 1st VDRL test was performed (n = 73) | ||
| 1 | 43 | 58.9 |
| 3 | 21 | 28.8 |
| 6 | 6 | 8.2 |
| 12 | 2 | 2.7 |
| 18 | 1 | 1.4 |
| Age when the VDRL test was negative (n = 49) | ||
| ≤6 | 44 | 89.8 |
| >6 | 5 | 10.2 |
| Had any clinical manifestations of CS (n = 101) | ||
| Yes | 16 | 15.8 |
| No/Ignored | 85 | 84.2 |
| Type of clinical manifestation of CS (n = 16)a | ||
| Anemia | 9 | 56.3 |
| Hepatic | 2 | 12.5 |
| Cardiocirculatory | 1 | 6.3 |
| Dermatological | 3 | 18.8 |
| Respiratory | 1 | 6.3 |
| Neurological | 3 | 18.8 |
| Was discharged from follow-up (n = 101) | ||
| Yes | 34 | 33.7 |
| No | 67 | 66.3 |
Seventy-one (70.3%) infants started the follow-up at one month of life; of these, 43 (60.5%) underwent the VDRL test, of which 13 (30.2%) had a positive result. Twenty-two (31.0%) infants did not return for subsequent appointments. The age at the first appointment ranged from 1 to 24 months (mean 1.8; SD 2.5) (data not shown in a table).
Twenty-eight (27.7%) infants did not undergo any VDRL test during the follow-up. Most infants (89.8%) had a negative VDRL test up to 6 months of age.
Seventeen infants (16.8%) underwent the VDRL test at one and three months of age, and when the test results were discordant, they were repeated at six and twelve months, until they were negative (data not shown in a table).
Thirty-four (33.7%) infants were discharged with completed follow-up. Sixteen (15.8%) infants had clinical manifestations related to CS during the follow-up, with anemia being the most frequent finding (56.3%). In 71 (70.3%) cases, there was no record regarding the clinical manifestations of CS in the medical file, making it impossible to identify the presence of any alteration.
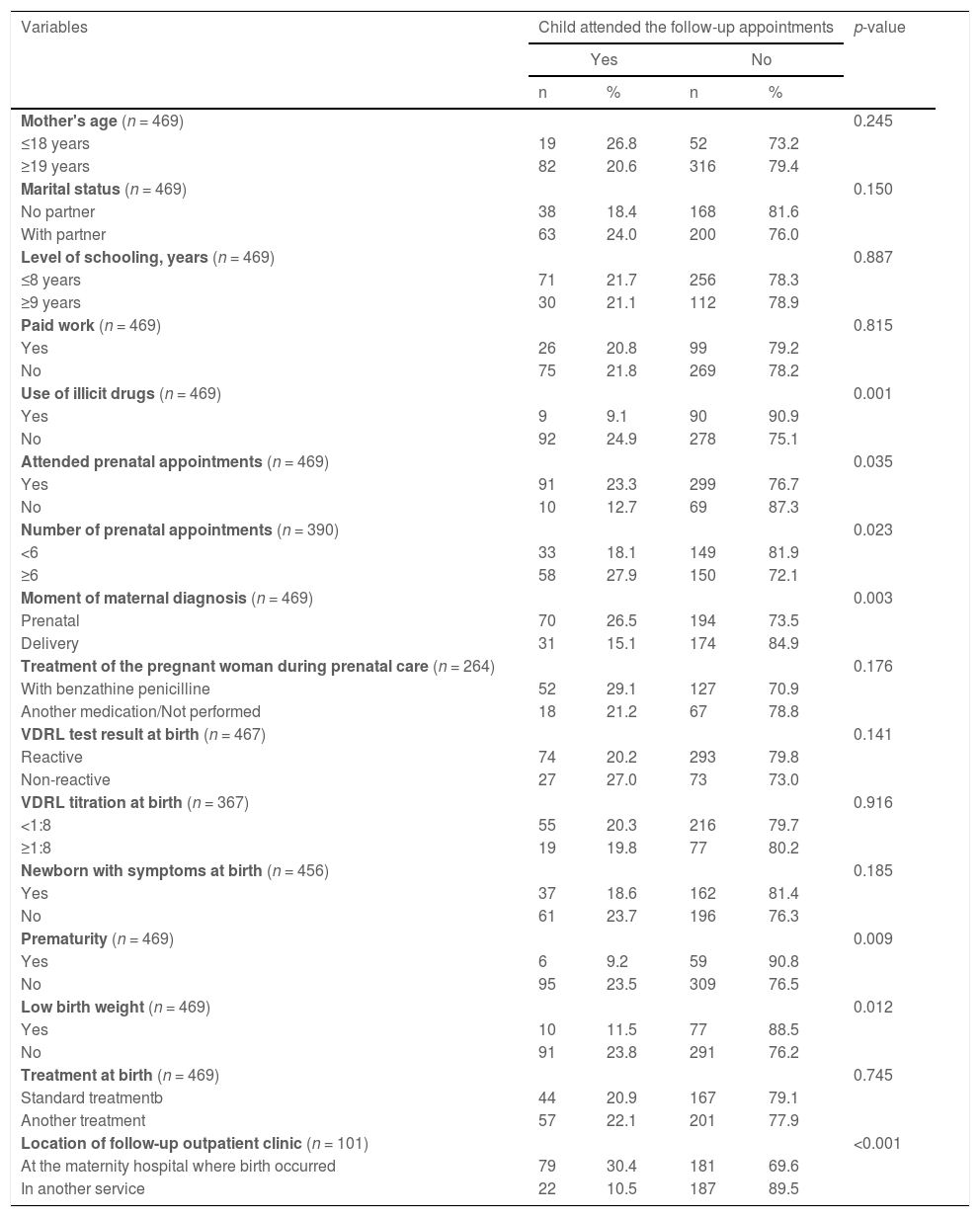
Table 2 shows the factors associated with the child's non-attendance of follow-up in relation to the mother's sociodemographic and prenatal care data and the child's birth conditions. A statistically significant association was found between infants who did not attend the follow-up and mothers who used illicit drugs (p = 0.001), did not attend prenatal care (p = 0.035), attended fewer than six prenatal appointments (p = 0.023), were diagnosed with syphilis at the time of delivery (p = 0.003), had a preterm birth (p = 0.009), had a newborn with low birth weight (p = 0.012) and were referred to follow-up in an outpatient clinic other than the maternity hospital where the infant was born (p < 0.001).
Factors related to non-attendance of appointments in follow-up outpatient clinics for congenital syphilis. Fortaleza, Ceará, 2015–2017.
aAt least one dose (2.4 to 7.2 million IU).
bCrystalline Penicillin or Procaine 10 days or single-dose Benzathine Penicillin.
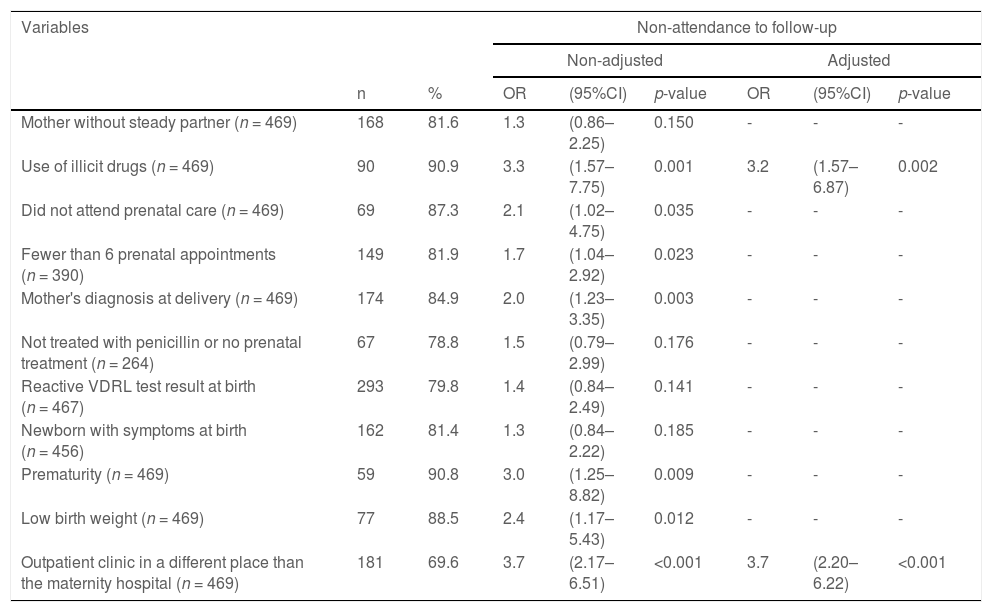
Table 3 shows the unadjusted and adjusted multiple logistic regression analysis of the factors related to the child's non-attendance to specialized outpatient clinics. The chance of a child not attending any follow-up appointment was 3.2 times greater when the mother was an illicit drug user (OR: 3.2; CI: 1.57–6.87; p = 0.002) and 3.7 times higher when the follow-up clinic was located in a service other than the maternity hospital where the infant was born (OR: 3.7; CI: 2.20–6.22; p < 0.001).
Multiple, unadjusted and adjusted logistic regression analysis of child attendance at the follow-up and maternal, laboratory, newborn clinical and location of the follow-up outpatient clinic variables. Fortaleza, Ceará, 2015–2017.
This study is significant to the understanding of the challenges experienced with infant follow-up in Ceará, Brazil, a state with a high maternal prevalence of syphilis and a limited supply of benzathine penicillin at the time of the study.
It was verified that the majority of infants notified with CS did not attend the outpatient follow-up at specialized services and those few who attended, did not receive care as recommended by the MOH. This is a matter of great concern, considering that the mothers of these infants were not treated or were treated inappropriately for CS.
Although the majority of the mothers had attended prenatal care, the coverage of this assistance was lower than that found in other studies of pregnant women with syphilis.11,12 This study reinforces that the quality of prenatal care is not related to the number of attended appointments, as it was identified that, despite the fact that most of them attended six or more appointments, a considerable proportion was not diagnosed or treated.
These missed opportunities in care seem to occur not only with the mothers during prenatal care but also in the referral and follow-up of these mothers and their newborns after delivery. It is necessary to consider that there is a strong correlation between these gaps within the health system and the infants' non-attendance to follow-up appointments.
The data on the birth of the newborns reported with CS shows that most of them had a positive VDRL test at birth and an important percentage had higher titers, which may suggest active syphilis. However, it is not known whether the VDRL titers of the newborns were higher than those of the mothers at delivery, which would constitute a diagnostic criterion.6
Almost 50% of the infants are not symptomatic at birth and prematurity and low birth weight may be the only disease manifestations. This finding reinforces the importance of the follow-up, considering that CS symptoms may occur later.4,6,13
The follow-up of infants with CS, especially in the context of penicillin shortage, becomes imperative, since the necessary tests and clinical evaluations must be carried out to assess the evolution of their health status. It was evidenced that 78.5% did not attend any of the appointments, a situation also identified among the 77.9% who received some alternative treatment. In the specific case of these infants, it is essential to carry out an active search for absentees to assess the need for retreatment. Faced with the shortage of penicillin, the MOH issued a note recommending the use of ceftriaxone as an alternative treatment for CS, but acknowledged the lack of evidence of its effectiveness and recommended that infants treated with alternative drugs be followed at shorter intervals, due to the possibility of therapeutic failure.10
It was found that the probability of the child not attending the follow-up is greater when the outpatient clinic is located in a service other than the maternity unit where the child was born. The greater demand by mothers for outpatient clinics located in the same maternity hospital where the birth occurred was possibly due to the bond established with the service. Every infant with CS is expected to have their first follow-up appointment already scheduled when they are discharged from the maternity ward after birth. When the mother is instructed to seek another service and the appointment is not scheduled, she may experience access difficulties, which interferes with the infant's follow-up.
As shown in this study, in the city of Fortaleza, all infants notified with CS were referred for follow-up at referral outpatient clinics, requiring the mother to travel long distances, and entailing expenses with transportation, which may have compromised adherence to follow-up. The municipal managers must make an effort to ensure the link between the child and the service, especially after the current recommendation of the MOH, which is to carry out the follow-up in primary care. However, another study carried out in Fortaleza showed a low adherence of infants also at this level of care12 and for this reason, it is considered essential that doctors and nurses in primary care be trained to include the specificities of the follow-up of infants with CS into the childcare routine.
The use of illicit drugs by the mothers was associated with the lack of infant follow-up. The mothers’ profile is similar to that found in other national studies, showing they are young women without paid work.11,14 These women seem to live in a context of vulnerability, aggravated by the use of illicit drugs, which requires specialized attention from primary care professionals who carry out prenatal care. Drug use and its consequences are not always adequately addressed in prenatal care.15,16 These pregnant women need to be advised regarding the importance of adherence to health care, allowing their referral to a specialized service that can help them to cope with the drug habit.
The use of these substances favors care neglect, such as low adherence to prenatal care17 and can contribute to the fact that many mothers do not feel able to take responsibility and care for their infants,18 which may result in giving the infant up for adoption or losing the infant's custody, situations that may hinder their presence at the follow-up. It is important to emphasize that Social Services and Child Protection Services have an important role to ensure the follow-up of these infants.
Ensuring an adequate follow-up seems to be a major challenge. In this study, when analyzing the follow-up of infants who attended at least one appointment, it was observed that the proportion of those who abandoned the follow-up was quite high, similar to that found in other studies carried out in Porto Alegre, Minas Gerais, Fortaleza and Paraná.4,7,12,19 Most infants did not attend all recommended appointments, did not undergo VDRL tests or these were not performed within the recommended time periods. This is a matter of concern and makes it unfeasible to ensure the health of these children, considering that discharge from follow-up depends on VDRL exams being carried out.6
It is necessary to bring these infants to the appointments to assess their current health status, their clinical manifestations, treatment effectiveness, and case evolution. It is noteworthy that non-adherence to follow-up appointments may also be related to the lack of active search for these infants. These cases should be considered a priority by the health services.
The most frequent alteration identified during the follow-up was the presence of anemia, a result similar to that found in Tanzania and in the Porto Alegre cohort.4,20 However, the possibility of under-recording of other clinical manifestations of CS cannot be ruled out, considering the high proportion of medical records without information about the presence or absence of these symptoms.
The scarcity of information due to the lack of recorded data in the medical files on infant care represents a limitation of this study. It is necessary to emphasize that all efforts were made to obtain such information. Missing medical care documentation is recognized as a persistent problem in clinical services. This may reflect additional deficiencies in the quality of clinical care of both mothers and infants, which the authors were not able to assess.
ConclusionIt was observed that many infants with CS do not attend the follow-up appointments at specialized outpatient clinics and that the fact of not showing up for the appointments is associated with maternal illicit drug use and the location of the referral outpatient clinic. This fact is a matter of great concern since the majority of these infants did not receive the recommended treatment for CS during hospitalization after birth due to the penicillin shortage, emphasizing the importance of clinical and laboratory follow-up.
Public health efforts aimed at reaching the parents of infants with CS should be a priority to ensure appropriate clinical identification and management of the associated outcomes of this vertically transmitted infection.
Institution where the study was carried out: Universidade de Fortaleza – UNIFOR, Fortaleza, Brazil.





