


to determine, by Doppler-echocardiography, the frequency of cardiac diastolic dysfunction in asymptomatic and clinically stable pediatric patients with vertical infection by the human immunodeficiency virus (HIV), from the cardiovascular viewpoint.
Methodsthis was an observational, prospective, and cross-sectional study, performed at a regional referral clinic for patients with HIV, in a convenience sample of 94 individuals, assessing biventricular diastolic function by Doppler-echocardiography, and weight, blood hemoglobin, and percentage of lymphocytes T-CD4+.
Resultsfifty patients had diastolic dysfunction. Left ventricular dysfunction occurred in 38.7%, and the predominant type of dysfunction was decreased myocardial compliance. Right ventricular dysfunction was observed in 29.4% of the sample, and abnormal relaxation was the most prevalent type. Simultaneous biventricular dysfunction occurred in 14.1% of the individuals. There was no association between dysfunction and the immune status.
Conclusionsdiastolic dysfunction occurred, individually or simultaneously, with no association with immune status; decreased myocardial compliance was predominant in the left ventricle, and abnormal relaxation in the right ventricle.
verificar, por meio do ecocardiograma com Doppler, a frequência de disfunção cardíaca diastólica em pacientes com infecção vertical pelo vírus da imunodeficiência humana na faixa pediátrica, assintomáticos e clinicamente estáveis do ponto de vista cardiovascular.
Métodosestudo observacional, prospectivo e transversal, realizado em um Ambulatório de Referência Regional para pacientes portadores do vírus da imunodeficiência humana, com uma amostra de conveniência de 94 pacientes, avaliados pelo sexo, idade, peso, função diastólica biventricular ao Doppler, hemoglobina sanguínea e percentual de linfócitos T-CD4+.
Resultadosapresentaram disfunção diastólica 50 pacientes. Disfunção ventricular esquerda ocorreu em 38,7% deles, e o tipo de disfunção predominante foi diminuição da complacência miocárdica. A disfunção ventricular direita foi evidenciada em 29,4% da amostra, sendo o tipo relaxamento anormal o mais prevalente. Disfunção biventricular simultânea ocorreu em 14,1% dos indivíduos. Não houve associação da disfunção com o estado imunológico.
Conclusõesfoi verificada disfunção diastólica, isolada ou simultânea, sem associação com o estado imunológico, sendo a diminuição da complacência miocárdica mais comum no ventrículo esquerdo e relaxamento anormal no ventrículo direito.
Cardiovascular manifestations often occur in children with vertical infection by the human immunodeficiency virus (HIV), and the most likely cause is multifactorial. In a prospective study, the cumulative five-year incidence of cardiac dysfunction in children ranged from 18% to 39%, and was the HIV-related cause of death in 11.8%.1–4
Subclinical cardiac abnormalities may develop in early HIV infection, even among individuals with asymptomatic disease or without cardiac dysfunction.1,4–9
The resolution of dilated cardiomyopathy in vertically infected children has been reported in those treated with a combination of drugs.6,10–12 It is possible that a change in diastolic function will precede systolic dysfunction, as observed in other clinical conditions, both in adults and in children and adolescents.3,13–23
The aim of this study was to determine the frequency of diastolic dysfunction in children vertically infected with HIV, both symptomatic and asymptomatic, and clinically stable from the cardiovascular perspective. The association between diastolic dysfunction and immunological status, malnutrition, and anemia was also investigated.
MethodsThis was an observational, cross-sectional study performed in a regional pediatric outpatient clinic for follow-up of patients with the acquired immunodeficiency syndrome (AIDS), consisting of a convenience, non-probabilistic sample.
The protocol and the informed consent were approved by the institutional ethics committee, and all participants consented to the study through their legal guardians. From June to November of 1999, 139 children vertically infected with HIV were evaluated, of whom 94 were selected according to the inclusion criteria. Age ranged from 20.3 to 170.6 months (mean 69.7 months) and 52 (55.0%) were males.
The definitive diagnosis was made according to the parameters of the Centers for Disease Control and Prevention (CDC, Atlanta, United States) of 1994: positive enzyme-linked immunoassay test (ELISA) and confirmatory test (Western blot).24
Forty-five patients were excluded from the analysis due to at least one of the following conditions: congenital heart disease; congestive heart failure; arrhythmia; aneuploidy; HIV-related infections; use of medications, including digitalis, beta-blockers, vasodilators, and antiarrhythmic drugs; use or previous use of cardiotoxic chemotherapeutic agents; percentage of T CD4+lymphocytes obtained at intervals greater than four months before or after the date of inclusion; and legal guardian's refusal of patient's participation in any phase of the study.
After obtaining the informed consent and determining patient eligibility for the study, blood samples were collected and the Doppler study was completed.
VariablesThe following variables were observed and recorded: gender, age (months), weight/age Z-scores25 using the software Epi Info™ 6.04 (GA, USA), blood hemoglobin level (g/dL), percentage of T CD4+lymphocytes, peak velocity of the E and A waves in the mitral and tricuspid valves (cm/s), and their ratios. The normal reference values used for the analysis of diastolic function in both ventricles were obtained from the available literature.26,27
Cardiac variables were obtained by pulsed Doppler in the apical four-chamber view, using a commercially available electronic transducer with a frequency of 3.5 or 5.0MHz (SI450 Sonoline; Siemens- Germany), guided by two-dimensional echocardiography and performed by one of the authors (MLS).
All measurements were the mean result of three consecutive cardiac cycles, and were performed on the equipment display screen and printed on X-ray films.
Statistical analysis was performed with Statistica 5.0 software (StatSoft, Brasil). Descriptive statistics and estimation of parameters were calculated (with 95% confidence intervals of [95% CI]), using factorial analysis (through the analysis of the main components) and multiple correlation analysis.
The ratios of E/A velocities of the atrioventricular valves were considered the main variables. Severe anemia and moderate or severe protein-calorie malnutrition were considered confounders.
ResultsOf the 94 children studied, 52 (55%) were males. There was a predominance of preschoolers, followed by school-aged children, but no differences were found between genders. Age ranged from 20.3 to 170.6 months (mean 69.7±31.7 months, and median 65.3 months).
Immunological status evaluation showed that the majority of children (57.4%) were non-immunocompromised (CD4+≥ 25%). Moderate immunological impairment (CD4+of 15% to 25%) was observed in 29 (30.9%), and severe immunological impairment (CD4+<15%) in 11 (11.7%).
Blood levels of hemoglobin (g/dL) ranged from 5.4 to 14.2, with a mean of 11.7+1.3, median of 11.7, and no significant differences between genders.
It was observed that ten (10.9%) children, five of each gender, had moderate or severe protein-calorie malnutrition (z-score ≤ -2.0).
As for the mitral E/A ratio, ten children had values below the minimum normal value (1.1), 26 were above the maximum normal value (3.9), and the remaining 57 were normal. When analyzing the tricuspid E/A ratio, normal values were found in 65 children. In contrast, in 15 the ratio was lower than the minimum normal value (1.58), and 12 had values above the maximum normal value (3.1).
As shown in Tables 1 and 2, the upper category of the mitral E/A ratio included 26 children (28.0%), and when assessing the association between the age groups, a slight predominance of preschoolers was observed (14.0%). The same occurred in the lower category, with eight of ten children. The upper tricuspid E/A ratio occurred in eight of 12 preschoolers and the lower in ten of the 15 individuals in this age group.
Categories of mitral valve E/A ratio according to age groups.
| Age groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Infant | Preschooler | School-aged | Adolescent | Total | ||||||
| MV E/A | n | % | n | % | n | % | n | % | n | % |
| Normal | 1 | 1.1 | 36 | 38.7 | 14 | 15.1 | 6 | 6.4 | 57 | 61.3 |
| Lower | 0 | 0.0 | 8 | 8.6 | 2 | 2.1 | 0 | 0.0 | 10 | 10.7 |
| Upper | 1 | 1.1 | 13 | 14.0 | 7 | 7.5 | 5 | 5.4 | 26 | 28.0 |
| Total | 2 | 2.2 | 57 | 61.3 | 23 | 24.7 | 11 | 11.8 | 93 | 100.0 |
MV-E/A, ratio between the peak velocities of E wave/A wave in the mitral valve; Infant, ≥ 18 and <24 months; Preschooler, ≥ 24 and <60 months; School-aged, ≥ 60 and <120 months; Adolescent, ≥ 120 and <180 months.
Categories of tricuspid valve E/A ratio according to age groups.
| Age groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Infant | Preschooler | School-aged | Adolescent | Total | ||||||
| TV-E/A | n | % | n | % | n | % | n | % | n | % |
| Normal | 2 | 2.2 | 38 | 41.3 | 15 | 16.3 | 10 | 10.9 | 65 | 70.7 |
| Lower | 0 | 0.0 | 10 | 10.8 | 5 | 5.4 | 0 | 0.0 | 15 | 16.2 |
| Upper | 0 | 0.0 | 8 | 8.7 | 3 | 3.3 | 1 | 1.1 | 12 | 13.1 |
| Total | 2 | 2.2 | 56 | 60.8 | 23 | 25.0 | 11 | 11.8 | 92 | 100.0 |
TV-E/A, ratio between the peak velocities of E wave/A wave in the tricuspid valve; Infant, ≥ 18 and <24 months; Preschooler, ≥ 24 and <60 months; School-aged, ≥ 60 and <120 months; Adolescent, ≥ 120 and <180 months.
When compassing the E/A ratio of both valves with the immunological status, nutritional status, and blood hemoglobin levels, no trend of association was observed.
The comparison between the mitral and tricuspid E/A ratios showed no association. The left heart abnormalities were not associated with abnormalities in the right side. Fifty of the 92 children had right and/or left ventricular dysfunction during the study.
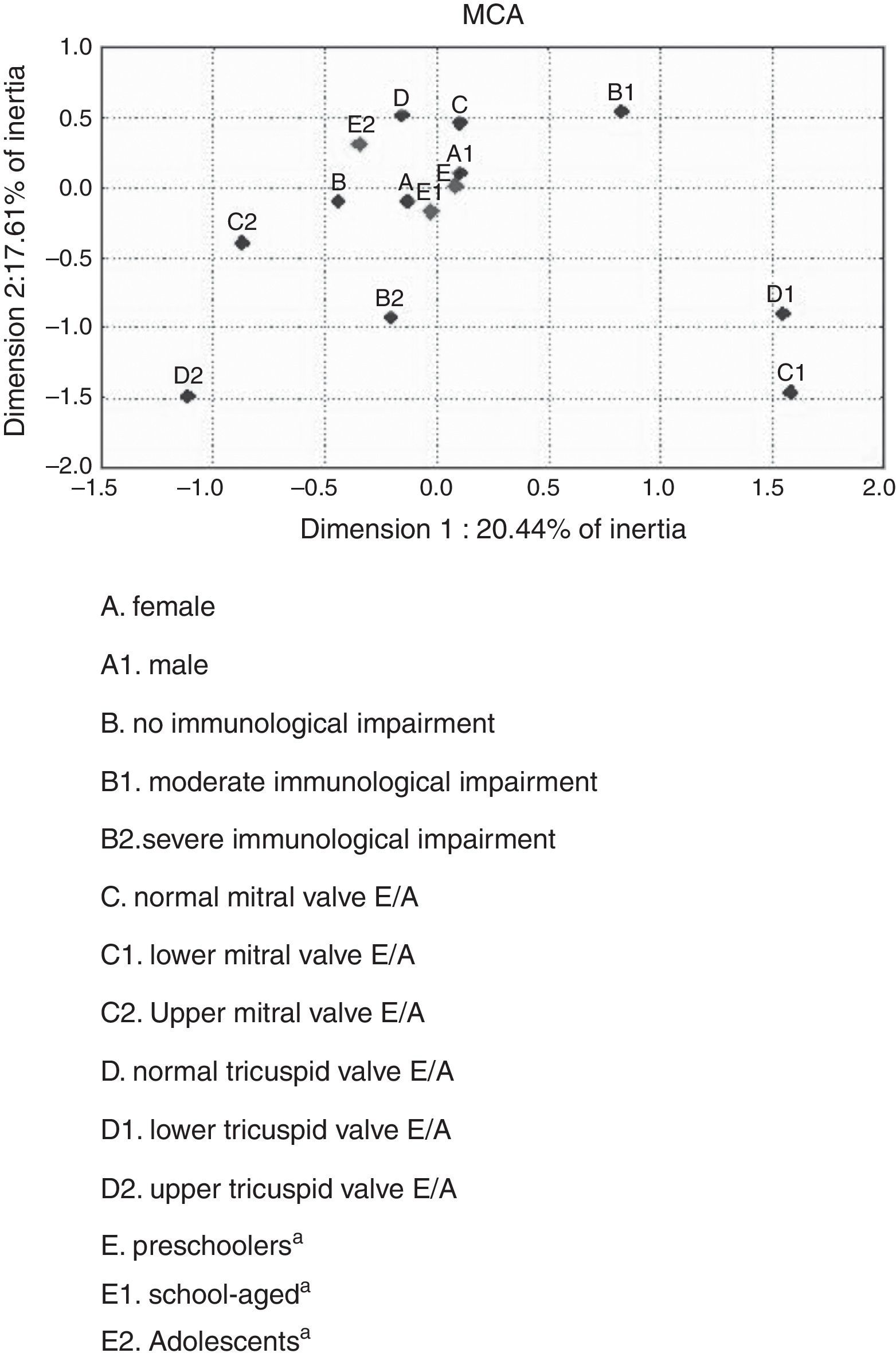
Factorial analysis identified two distinct groups of children who were slightly separated, indicating that they would need further clinical evaluation, as they probably constituted two classes with distinct characteristics.
The results of the multiple correlation analysis for all seven possible dimensions demonstrated that the first dimension had the highest percentage of inertia, or 20.44% of the total inertia. After including the second dimension analysis, the percentage of inertia increased to 38.05%.
The numbers generated from the simple and inertia values for all dimensions of the 11 independent variables, in two dimensions, contributed to the categorical behavior analysis. However, data generated by multiple correlation analysis showed an independent behavior, with no association between categorical variables (Fig. 1).
Discussion between categorical variables. aSupplementary variables.")
HIV-infected children are predisposed to cardiac dysfunction as an independent predictor of all-cause mortality, and the exact pathogenesis of cardiac events remains uncertain, but it is most likely multifactorial.9,28
To prevent complications, the assessment of subclinical cardiac abnormalities is suggested. In adults, an independent association between diastolic dysfunction and HIV infection was reported in a series of studies, even among asymptomatic HIV-infected patients in the early stages of the disease.3,16–20
It is possible that the diastolic alterations may be an early finding, but their impact on the clinical course of the disease and the possible reversibility of severe complications still need to be elucidated.3,13–17,29
Diastolic dysfunction was found in 50 (54.3%) children, regardless of the side. When the left and right sides were evaluated separately, it was observed that 38.7% (95% CI: 28.8%-48.6%) had left diastolic dysfunction and 29.4% (95% CI: 20.1%-38.7%) had right diastolic dysfunction. On the left side, there was a predominance of decreased myocardial compliance (28.0%; 95% CI: 8.9%-37.1%) compared to 10.7% of abnormal relaxation (95% CI: 4.4%-17.0%). The situation was the opposite on the right side of the heart, with a slight predominance of abnormal relaxation (16.3%; 95% CI: 8.7%-23.7%) compared to the decrease in compliance (13.1%; 95% CI: 6.2%-20.0%).
Plein et al.23 reported abnormalities in the left ventricular filling pattern, such as reduction in the maximum velocity of the E wave and increased deceleration time, consistent with diastolic dysfunction in HIV-infected children, classified as stage C according to the classification reviewed by the CDC.
Reports on left ventricular diastolic dysfunction in children are limited, and the existing are almost always associated with systolic dysfunction, as they are usually symptomatic.22,30
The fact that the immunological status and physical examination did not show a direct association with cardiac involvement demonstrates that HIV-infected children and adolescents should be submitted to Doppler echocardiographic study as part of the evaluation, even when asymptomatic from a cardiovascular perspective.
Limitations of this study are related to the design, since a non-probabilistic, convenience sample was used, limiting the external validity of these results. The selection bias, inherent to investigations in referral centers, was considered in the sample composition, when the authors planned to study all potentially eligible children.
This sample was characterized as a more selective group. Potential confounders, including severe anemia and moderate to severe protein-calorie malnutrition, showed low frequencies, and it was not possible to assess their influence as associated causes of cardiac dysfunction. However, this fact reflects the studied group's stable condition, as anemia and malnutrition are still prevalent conditions in Brazil.
Cardiac diastolic dysfunction occurred in patients with the selected characteristics, and there was no association with immunological status. Decreased myocardial compliance was more frequent in the left ventricle and abnormal relaxation in the right ventricle.
FundingThe study was funded by the authors. Hospital Infantil Joana de Gusmão (HIJG) provided the equipment to perform the echocardiography assessment and the material for the documentation of examinations (X-ray films). Laboratory tests were performed as part of patients’ routine outpatient care, with no additional costs for the institution (HIJG). The Infectious Disease Department of HIJG authorized the use of its facilities for the primary care of patients and for the explanation necessary to the informed consent.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Silva ML, Nassar SM, Silva AP, Ponce LL, Pires MM. Biventricular diastolic function assessed by Doppler echocardiogram in children vertically infected with human immunodeficiency virus. J Pediatr (Rio J). 2014;90:403–7.





