
To describe the users’ drug abuse characteristics, problematic behaviors associated with addiction, the motivation of teenagers and young adults to quit cocaine and/or crack abuse, and then compare these characteristics.
MethodsA cross-section study was conducted with 2390 cocaine/crack users (teenagers from 14 to 19 years of age, and young adults from 20 to 24 years of age); 1471 were young adults and 919 were teenagers who had called a phone counseling service between January 2006 and December 2013. Semi-structured interviews were performed via phone calls. The questionnaires included sociodemographic information; assessment of the characteristics of cocaine/crack abuse; assessment of the problematic behaviors; also, the Contemplation Ladder was used to evaluate the stages of readiness to cease substance abuse.
ResultsParticipants reported using cocaine (48.2%), crack and other smoking forms (36.7%) and combined consumption of both drugs (15%). Young adults were more prone to using crack or crack associated with cocaine (OR=1.9; CI 95%=1.05–1.57) and they were exposed to substance abuse for longer than two years (OR=3.45; CI 95%=2.84–4.18), when compared to teenagers. On the other hand, they showed higher readiness to quit.
ConclusionData shows important differences in drug abuse characteristics, problematic behaviors and motivation to cease substance abuse between teenager and young adult cocaine and/or crack users. Behaviors displayed by young adults involve greater physical, mental and social health damages. These findings reinforce the importance of public policy to act on prevention and promoting health, to increase protection factors among teenagers and lower risks and losses during adult life.
Descrever as características de consumo, comportamentos problemáticos associados ao uso e motivação para cessar o consumo entre adolescentes e jovens usuários de cocaína e/ou crack e comparar essas características.
MétodosRealizou-se um estudo transversal, com 2.390 usuários de cocaína/crack (adolescentes: 14 – 19 anos e jovens: 20 – 24 anos) sendo 1471 jovens e 919 adolescentes, que ligaram para um serviço de aconselhamento telefônico entre janeiro de 2006 e dezembro de 2013. Foram realizadas entrevistas semiestruturadas por telefone. Os questionários incluíram informações sociodemográficas; avaliação das características do consumo de cocaína/crack; avaliação dos comportamentos problemáticos e escala de Contemplação Ladder para avaliar os estágios de motivação.
ResultadosOs participantes relataram uso de cocaína (48,2%), crack e outras formas fumadas (36,7%) e uso associado de ambas as formas (15%). Os jovens faziam maior uso de crack ou crack associado à cocaína (OR = 1,19; IC 95% = 1,05-1,57) e estavam expostos ao uso da droga havia mais de 2 anos (OR=3,45; IC 95% = 2,84-4,18) quando comparados aos adolescentes. Por outro lado, mostraram-se mais motivados para cessar o consumo.
ConclusãoOs dados mostraram haver importantes diferenças nas características de consumo, comportamentos problemáticos e motivação para cessar o consumo entre adolescentes e jovens usuários de cocaína e/ou crack. Os jovens apresentaram comportamentos que envolvem maiores prejuízos para a saúde física, mental e aspectos sociais. Esses achados reforçam a importância de ações de políticas públicas de prevenção e promoção de saúde para aumentar os fatores de proteção entre os adolescentes e reduzir riscos e prejuízos para a vida adulta.
The 2015 World Drug Report showed that while cocaine/crack use has stabilized in the rest of the world, there has been an increase in consumption in South America.1 By 2014, in the United States, approximately one million individuals over the age of 12 have been classified as cocaine addicts or abusers.2 Regarding Brazil, the country ranks second in the cocaine trade and first in crack consumption, accounting for 20% of the world's consumption.3
Approximately 200,000 young Brazilians reported using intranasal cocaine in the last 12 months, and 150,000 young individuals used crack or similar drugs at least once.3 According to a study carried out to describe the profile of users of crack and/or similar drugs in Brazil, in 2012, the age group with highest prevalence was that of 18–24 years (31.32%).4
Adolescence/young adulthood is an evolutionary phase that brings many obstacles and can lead individuals to engage in risky activities, such as drug use.5 According to the World Health Organization (WHO), young individuals aged 10–19 years are considered adolescents, and between 20 and 24 years of age, as young adults.6
It is known that drug experimentation usually begins in adolescence.7 However, at this stage of development, when major body changes occur, especially in the central nervous system (CNS), drug use may impair brain function, affecting cognitive and learning ability.7 Delaying or preventing the onset of psychoactive substance use by young individuals has been a worldwide challenge for those responsible for public health policies. Many studies have shown the risks related to drug experimentation, use, and abuse among adolescents and young adults.8,9 Early use of cocaine and/or crack increases the risk of developing a substance use-related disorder, as well as other mental disorders during adolescence and young adulthood.10 Understanding the patterns of cocaine and/or crack use among adolescents and young adults can assist in the planning of targeted and more effective prevention actions, as well as in the development of more effective treatment strategies.11
The present study aimed to describe the characteristics of drug use, problem behaviors associated to this use, and readiness to cease consumption among adolescents and young users of cocaine and/or crack, and to compare these characteristics between the two groups.
MethodsA cross-sectional study was conducted with a convenience sample of 2390 cocaine/crack users (adolescents between 14 and 19 years of age and young individuals between 20 and 24 years of age), who reported using drugs associated or not with other substances and called a counseling service number aiming at seeking help to stop this consumption. The “Ligue 132” (Call 132) is a telephone counseling service that aims to assist users of psychoactive substances during the consumption cessation process. Data collection occurred from January 2006 to December 2013, and during this period, 3272 young individuals and adolescents called the service. A total of 892 adolescents and adolescents who reported being under the effect of drugs during the call were excluded, as well as those with cognitive difficulties to understand or respond to the tools, and those who did not agree to participate in the study.
The users accepted to participate in the study through an informed consent process, carried out verbally, with implicit acceptance after learning about the project objectives and purpose. The consent was requested during the first call made by the user. Oral acceptance was duly recorded in the computerized protocols.12 The present study was approved by the Ethics and Research Committee of Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), process No. 942/12.
Data collection was carried out by consultants, who were university students from different health areas trained to work at the call center and to apply the intervention to the users under the supervision of healthcare professionals. The training process consisted of: (a) theoretical classes as a continuing education course on how to approach chemical dependency (40h); (b) theoretical–practical training in the call center for software familiarization (20h) and motivational interview training; and (c) continuous training to maintain the quality of the provided information.13 The training model was adapted from the Medical Education Model for the Prevention and Treatment of Alcohol Use Disorders.14
Semi-structured interviews were carried out by telephone, with a mean duration of 50min. The questionnaires included: (a) the general treatment protocol, containing information such as gender, age, marital status, profession, family income, level of schooling, and city and state where the call originated; (b) assessment of cocaine/crack consumption, with questions that characterized the amount (grams/stones of cocaine/crack) used per occasion, frequency, and pattern of consumption. For this purpose, a questionnaire created by the World Health Organization (WHO), which has been widely adopted in Brazil, was used15; and (c) assessment of problem behaviors due to cocaine/crack use, a questionnaire created by the National Household Survey on Drug Abuse (NHSDA)16 to assess problems related to cocaine/crack use, chosen because it is utilized in drug use surveys in Brazil. This questionnaire shows six problem behaviors, according to the DSM-5. For data collection, the subjects’ consumption is defined as mild (two to three symptoms), moderate (four to five symptoms), and severe (over six symptoms); and (d) the Contemplation Ladder, used to qualitatively assess motivation using five statements that seek to identify an individual's willingness to cease consumption through the motivational stages (pre-contemplation, contemplation, preparation, action/maintenance).17
The univariate descriptive analysis shows sociodemographic data, cocaine and/or crack consumption markers, motivation indexes, and information on drug-related problem behaviors as mean±standard error of the mean (SEM), whereas the qualitative data are shown as n and percentages. In the bivariate analyses, the chi-squared test, odds ratio (OR), and 95% confidence interval (95% CI) were used for comparisons of data between adolescents and young individuals and to differentiate between cocaine and crack users. To compare the substance amounts used between the age groups, the t-test for independent samples was used.
A multivariate analysis was performed to confirm the main differences between the age groups, and all variables with p<0.20 in the bivariate analysis were included in the logistic regression analysis (sought help before calling the service, type of preparation – crack or cocaine, time of use, frequency, dependence, drug use-related problems, and stages of change). p-Values <0.05 were considered statistically significant. Spearman's bivariate correlation analysis was performed. The analyses were performed using the IBM SPSS Statistics 19.0 software.
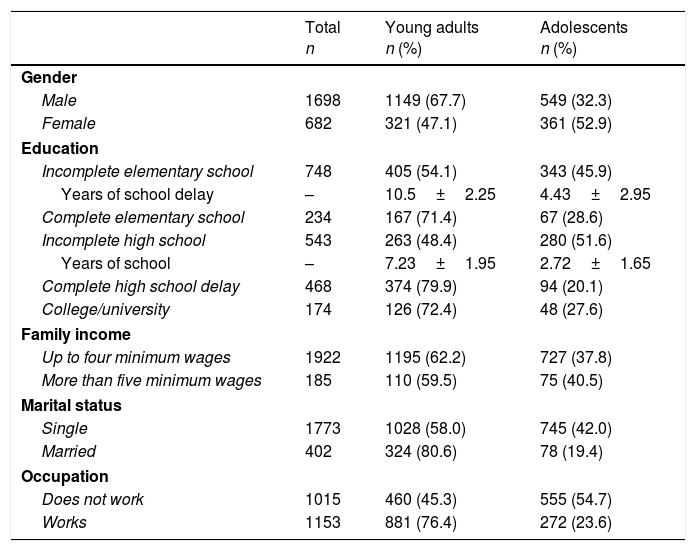
ResultsThe mean age was 22.1 years (SD=1.39) among young individuals and 17.3 years (SD=1.36) among adolescents. When analyzing the participants’ level of schooling, in general, it was observed that most of them, both young adults and adolescents, did not finish their studies. Only 10% of the participants reported having finished elementary school and 20.7% had finished high school. Among those who did not finish their studies, it was observed that 62.5% of the young adults and 67.3% of the adolescents showed poor academic performance. There was a direct correlation between school delay and severity of problems related to cocaine/crack use (r=0.063; p=0.002); age of participants (r=0.238; p=0.000) and amount of cocaine consumed (r=0.158, p=0.000), with all correlations being weak. A weak indirect correlation was also found between school delay and amount of crack consumed (r=−0.142, p=0.000). When asked about occupation, 22.6% of the participants said they were students (most of them were adolescents), 21.1% reported being unemployed (young adults, mostly), and 56.3% said they performed some work activity. The sociodemographic characteristics of the participants are summarized in Table 1.
Comparison of the sociodemographic characteristics between young adults and adolescentsa who used cocaine/crack.
| Total n | Young adults n (%) | Adolescents n (%) | |
|---|---|---|---|
| Gender | |||
| Male | 1698 | 1149 (67.7) | 549 (32.3) |
| Female | 682 | 321 (47.1) | 361 (52.9) |
| Education | |||
| Incomplete elementary school | 748 | 405 (54.1) | 343 (45.9) |
| Years of school delay | – | 10.5±2.25 | 4.43±2.95 |
| Complete elementary school | 234 | 167 (71.4) | 67 (28.6) |
| Incomplete high school | 543 | 263 (48.4) | 280 (51.6) |
| Years of school | – | 7.23±1.95 | 2.72±1.65 |
| Complete high school delay | 468 | 374 (79.9) | 94 (20.1) |
| College/university | 174 | 126 (72.4) | 48 (27.6) |
| Family income | |||
| Up to four minimum wages | 1922 | 1195 (62.2) | 727 (37.8) |
| More than five minimum wages | 185 | 110 (59.5) | 75 (40.5) |
| Marital status | |||
| Single | 1773 | 1028 (58.0) | 745 (42.0) |
| Married | 402 | 324 (80.6) | 78 (19.4) |
| Occupation | |||
| Does not work | 1015 | 460 (45.3) | 555 (54.7) |
| Works | 1153 | 881 (76.4) | 272 (23.6) |
Some participants did not answer all questions.
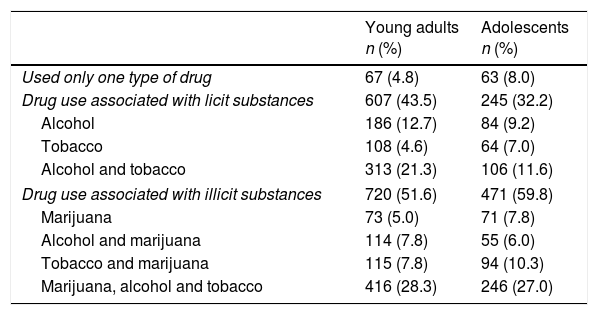
When data on drug use were analyzed, participants reported using cocaine (48.2%), crack and other smoked forms (36.7%), and associated use of both forms (15%). Cocaine/crack use associated with other licit or illicit drugs was reported by 94.5% of the participants, and only 6% of the participants used only one type. When analyzing the use associated with other drugs of abuse, 39.5% of the users reported the association with licit drugs and 54.6% declared use associated with other illicit drugs (Table 2). The associations showed significant statistical differences between young adults and adolescents. Young adults were less likely to associate illicit drugs when compared with adolescents (OR=0.61, 95% CI=0.51–0.74). The association between cocaine/crack use and with alcohol and/or tobacco was more frequent among young adults, while adolescents more frequently reported associations of cocaine/crack with marijuana.
Drug use associated with other substances: comparison between young adults and adolescentsa using cocaine/crack.
| Young adults n (%) | Adolescents n (%) | |
|---|---|---|
| Used only one type of drug | 67 (4.8) | 63 (8.0) |
| Drug use associated with licit substances | 607 (43.5) | 245 (32.2) |
| Alcohol | 186 (12.7) | 84 (9.2) |
| Tobacco | 108 (4.6) | 64 (7.0) |
| Alcohol and tobacco | 313 (21.3) | 106 (11.6) |
| Drug use associated with illicit substances | 720 (51.6) | 471 (59.8) |
| Marijuana | 73 (5.0) | 71 (7.8) |
| Alcohol and marijuana | 114 (7.8) | 55 (6.0) |
| Tobacco and marijuana | 115 (7.8) | 94 (10.3) |
| Marijuana, alcohol and tobacco | 416 (28.3) | 246 (27.0) |
Some participants did not answer all questions.
Age according to age groups=adolescents (14–19 years), young adults (20–24 years).
The variable drug use associated with licit substances refers to the total number of young adults and adolescents who reported the concomitant use of cocaine and/or crack with alcohol and/or tobacco.
The variable drug use associated with illicit substances refers to the total number of young adults and adolescents who reported the concomitant use of cocaine and/or crack with marijuana, alcohol and/or tobacco.
In relation to the amount of drug used per occasion, young adults used on average 8.11g (SE=0.45) of cocaine, 14.3 crack stones (SE=0.72) and, when used concomitantly, 6.9g (SE=0.3). For adolescents, the mean amount of cocaine was 12.1g (SE=1.1), 10.1 crack stones (SE=1.18) and both, 8.3g (SE=0.83), without statistical differences.
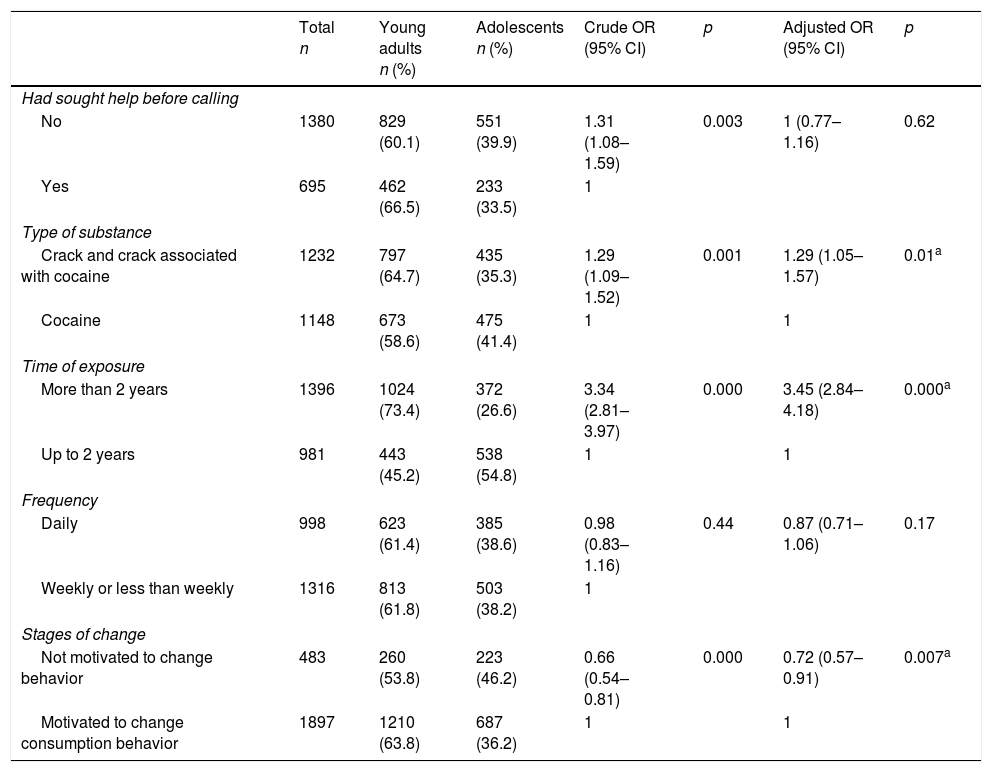
Crude and adjusted bivariate analyses were performed to verify statistical differences between young adults and adolescents regarding the consumption characteristics. It was observed that most young adults and adolescents sought help for the first time when they called the service. Young adults used crack or crack associated with cocaine and had been using drugs for a longer period of time when compared with adolescents, with a statistically significant difference. Regarding the frequency of use, groups indicated a weekly or less than weekly frequency. In turn, although young adults had a greater probability of using drugs, when the motivational stages to cease consumption was assessed, it was observed that young adults were more likely to be motivated to change the cocaine/crack use behavior than adolescents (Table 3).
Characteristics of cocaine/crack consumption: comparison between young adults and adolescents.
| Total n | Young adults n (%) | Adolescents n (%) | Crude OR (95% CI) | p | Adjusted OR (95% CI) | p | |
|---|---|---|---|---|---|---|---|
| Had sought help before calling | |||||||
| No | 1380 | 829 (60.1) | 551 (39.9) | 1.31 (1.08–1.59) | 0.003 | 1 (0.77–1.16) | 0.62 |
| Yes | 695 | 462 (66.5) | 233 (33.5) | 1 | |||
| Type of substance | |||||||
| Crack and crack associated with cocaine | 1232 | 797 (64.7) | 435 (35.3) | 1.29 (1.09–1.52) | 0.001 | 1.29 (1.05–1.57) | 0.01a |
| Cocaine | 1148 | 673 (58.6) | 475 (41.4) | 1 | 1 | ||
| Time of exposure | |||||||
| More than 2 years | 1396 | 1024 (73.4) | 372 (26.6) | 3.34 (2.81–3.97) | 0.000 | 3.45 (2.84–4.18) | 0.000a |
| Up to 2 years | 981 | 443 (45.2) | 538 (54.8) | 1 | 1 | ||
| Frequency | |||||||
| Daily | 998 | 623 (61.4) | 385 (38.6) | 0.98 (0.83–1.16) | 0.44 | 0.87 (0.71–1.06) | 0.17 |
| Weekly or less than weekly | 1316 | 813 (61.8) | 503 (38.2) | 1 | |||
| Stages of change | |||||||
| Not motivated to change behavior | 483 | 260 (53.8) | 223 (46.2) | 0.66 (0.54–0.81) | 0.000 | 0.72 (0.57–0.91) | 0.007a |
| Motivated to change consumption behavior | 1897 | 1210 (63.8) | 687 (36.2) | 1 | 1 | ||
Some participants did not answer all questions.
For a more detailed analysis, in the assessment of the consumption characteristics, the sample was differentiated between users of crack and cocaine, comparing the age groups. Among crack users, young adults were nearly three times more likely to have been consuming the substance for more than two years when compared with adolescents (OR=2.84, 95% CI=2.16–3.73). Likewise, it was observed that among cocaine users, young adults were four times more likely to have been using the drug longer than adolescents (OR=4.38; 95% CI=3.30–5.82). Data on motivation were also maintained among young adults who were crack users (OR=0.63, 95% CI=0.45–0.88); however, there was no significant difference between young adults and adolescents who were cocaine users.
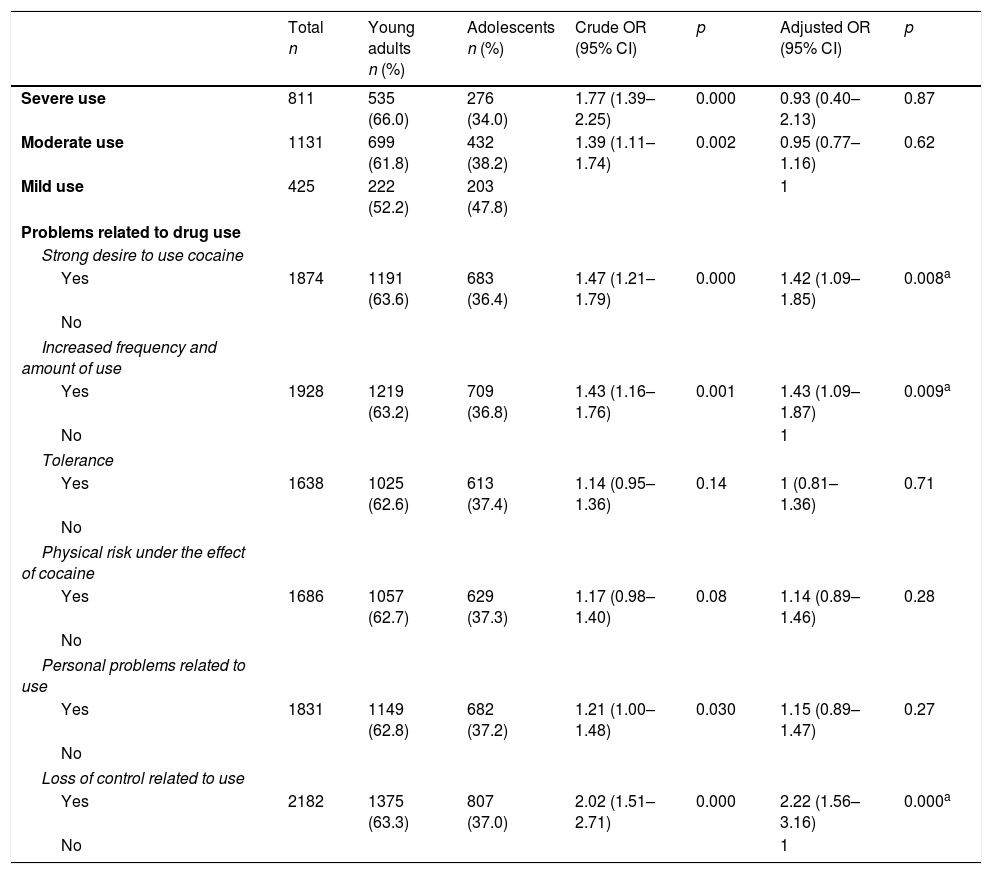
When assessing the severity of problem behaviors due to cocaine/crack use, 1131 users (47.8%) met the criteria for moderate use and 811 users (34.3%) for severe use. When assessing problem behaviors related to drug use in the last 12 months, young adults were more likely to crave the drug, to increase the frequency of use or the amount of the drug, and lose control over the use (OR=1.42, p=0.008; OR=1.43, p=0.009; and OR=2.22, p=0.000, respectively), as shown in Table 4. When analyzing the associations between problem behaviors related to use in the last 12 months, it was observed that among young adults, the loss of control was associated with a strong desire to use cocaine and/or crack (p=0.000), increased frequency of use (p=0.003), tolerance to substance effects (p=0.01), exposure to physical risks (p=0.005), and personal problems related to the substance use (p=0.000). For adolescents, loss of control was associated with a strong desire to use cocaine and/or crack (p=0.04) and personal problems related to the substance use (p=0.003).
Characteristics of problem behaviors related to cocaine/crack use: comparison between young adults and adolescents.
| Total n | Young adults n (%) | Adolescents n (%) | Crude OR (95% CI) | p | Adjusted OR (95% CI) | p | |
|---|---|---|---|---|---|---|---|
| Severe use | 811 | 535 (66.0) | 276 (34.0) | 1.77 (1.39–2.25) | 0.000 | 0.93 (0.40–2.13) | 0.87 |
| Moderate use | 1131 | 699 (61.8) | 432 (38.2) | 1.39 (1.11–1.74) | 0.002 | 0.95 (0.77–1.16) | 0.62 |
| Mild use | 425 | 222 (52.2) | 203 (47.8) | 1 | |||
| Problems related to drug use | |||||||
| Strong desire to use cocaine | |||||||
| Yes | 1874 | 1191 (63.6) | 683 (36.4) | 1.47 (1.21–1.79) | 0.000 | 1.42 (1.09–1.85) | 0.008a |
| No | |||||||
| Increased frequency and amount of use | |||||||
| Yes | 1928 | 1219 (63.2) | 709 (36.8) | 1.43 (1.16–1.76) | 0.001 | 1.43 (1.09–1.87) | 0.009a |
| No | 1 | ||||||
| Tolerance | |||||||
| Yes | 1638 | 1025 (62.6) | 613 (37.4) | 1.14 (0.95–1.36) | 0.14 | 1 (0.81–1.36) | 0.71 |
| No | |||||||
| Physical risk under the effect of cocaine | |||||||
| Yes | 1686 | 1057 (62.7) | 629 (37.3) | 1.17 (0.98–1.40) | 0.08 | 1.14 (0.89–1.46) | 0.28 |
| No | |||||||
| Personal problems related to use | |||||||
| Yes | 1831 | 1149 (62.8) | 682 (37.2) | 1.21 (1.00–1.48) | 0.030 | 1.15 (0.89–1.47) | 0.27 |
| No | |||||||
| Loss of control related to use | |||||||
| Yes | 2182 | 1375 (63.3) | 807 (37.0) | 2.02 (1.51–2.71) | 0.000 | 2.22 (1.56–3.16) | 0.000a |
| No | 1 | ||||||
Some participants did not answer all questions.
The results demonstrate that there are important differences in the consumption characteristics, problem behaviors related to the use, and motivation to cease consumption among young adults and adolescents who use cocaine/crack. Young adults were more likely to use crack, to have been using drugs for a longer period, and to have more problem behaviors related to consumption, while adolescents were more likely to use other illicit drugs and to have less motivation to change the problem behavior. Furthermore, an association was found between levels of schooling and severity of problems with cocaine and crack use.
The data showed that most of the young adults and adolescents did not complete their studies. It is known that drug use is strongly related to poor academic performance, and the continuity of use is associated with poor school results, often leading to school abandonment. Epidemiological studies have shown a high association between school dropout rates and mental health problems,18,19 illicit activities,19 and a particularly increased risk for problems related to the use of alcohol, cigarettes, marijuana and other illicit drugs.20 School delay was associated with the severity of problems related to the consumption and amount of used cocaine, as well as age; that is, the older the user, the greater the school delay, the more problems with consumption, and the greater the amount of cocaine used.
In the present study, young adults were more likely to use crack or a combination of crack and cocaine, and more likely to have been using the drug for more than two years. It can be hypothesized that these young adults started using crack after their experiences with cocaine and marijuana during adolescence. A study that aimed to assess the sociodemographic profile and pattern of cocaine use among hospitalized drug users found similar results. Among the 440 interviewed patients, 29.8% were cocaine addicts, 38.4% were crack addicts and 31.8% used both forms of cocaine (inhaled and smoked).21 Another study that sought to investigate the prevalence of cocaine use and dependence in Brazil and possible associations with sociodemographic factors showed that 45% of the sample started using cocaine before the age of 18 years.22 A study that investigated the use of other drugs of abuse in 20 crack users identified that substance consumption had begun with licit drugs (alcohol and tobacco), progressing to other illicit drugs, such as marijuana and cocaine. Cocaine was the third most commonly used drug, whereas crack was the last drug to be used in half of the assessed cases.23 The literature has pointed out that the progression of use usually occurs in adolescence, with the experimental use of licit drugs (alcohol and tobacco) and then progressing to the use of illicit drugs (marijuana and inhaled cocaine).24
The results of the present study indicated that adolescents showed a higher risk for associations with other illicit drugs and that almost 100% used more than one drug. A study among cocaine and crack users who sought treatment showed a 25% prevalence of dependence on one substance, 32.6% dependence on two, and 22.4% dependence on three drugs.25 These findings reinforce the urgency of interventions, since it is known that the longer the time of exposure to a substance, the greater the damage to the development of young individuals.26
The findings of this study did not show significant differences between age groups regarding the severity of problems related to substance use, i.e., both groups showed moderate to severe problems related to cocaine and/or crack use. The association between early use and increased risk for psychiatric illnesses has been demonstrated in the literature.24 Another important finding was the association of problem behaviors related to cocaine/crack use. Statistically significant associations were observed in all six assessed behaviors among young adults, which raises the question about the severity of the abuse. Although adolescents reported problem behaviors, they did not show loss of control associated with frequency of use, tolerance to effects, and exposure to physical risks. This finding may be explained by the fact that they had been exposed to the substance for a shorter period, when compared with young adults. However, it is important to emphasize the importance of early interventions aiming to prevent drug use, as well as preventing the progression of experimentation to other drugs that represents greater risks regarding drug use-related problems and severity related to frequent consumption. Community- and school-based prevention programs and specific health care strategies for adolescents and young adults can contribute to a healthier psychosocial development, preventing more severe losses in adult life.27
The profile of young individuals in the present study do not differ from that presented in the literature (moderate to severe use, users of more than one drug, with poor school performance); however, when assessing the readiness to modify the behaviors, young adults reported higher motivation, a fact that can be understood by the possible perception of the losses related to the consumption. Adolescents, in turn, were more likely to be in the pre-contemplation and contemplation stages, that is, with low motivation to change the behavior. Adolescents are still immature in their ability to assess risks, consider consequences and organize the cause-effect association in a temporal manner; this occurs because the brain structures responsible for impulse control and temporal perception are still maturing.28 Due to these characteristics, adolescents may not realize the need to change their consumption or are not ready to make such decision.
Most young adults and adolescents sought help for the first time by calling the telephone counseling service. It is known that, generally, this population does not spontaneously seek help, especially when they have low motivation to change their behavior. However, anonymity and easy access to advice devoid of prejudice and judgments may have stimulated them to seek help. The literature shows that telephone contact has become an advantageous alternative for healthcare services,29 and these treatment alternatives have proven effective for cessation and reduction of drug use.30
The present study has some limitations. The first to be highlighted is the sample selection process, which occurred by convenience. The study was carried out with users who had access to information about the existence of a free and anonymous telephone service and who called the telephone number. It is not possible to know how many young individuals received information about the service and did not call it. Therefore, the impact of a selection bias cannot be estimated. In turn, as the information about the telephone service was widely disseminated by television, internet, and radio at a national level, it can be assumed that there was an opportunity for young individuals from every Brazilian region to seek contact through the service.
No other risk factors, such as the presence of comorbidities, violence, school dropout, and parental relationship, were assessed. These factors are important for the overall understanding of drug use by young individuals. However, as this study aimed to investigate the difference in consumption patterns, dependence, and motivation among adolescents and young individuals, it is believed that the fact that the other risk factors were not investigated had no interference on the results.
The findings of the present study showed important differences in the characteristics of drug consumption, problem behaviors, and motivation to cease consumption among adolescents and young adults that used cocaine and/or crack. Young adults, despite showing a lower association of cocaine and/or crack use with illicit drugs, showed a more frequent use of crack and had been using these substances for a longer time, in addition to showing behaviors that involve greater damages to the physical and mental health in addition to damages related to the social aspects. Regarding the motivation to cease consumption, adolescents were less motivated to do so than young adults. These findings reinforce the importance of seeking more appropriate methodologies for early interventions, aiming to increase protective factors among adolescents and reduce the risks and damages to adult life.
FundingNational Secretariat of Drug Use Policies (SENAD) and Associação Mario Tannhauser de Ensino Pesquisa e Assistência (AMTEPA).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Bisch NK, Moreira TC, Benchaya MC, Pozza DR, Freitas LC, Farias MS, et al. Telephone counseling for young Brazilian cocaine and/or crack users. Who are these users? J Pediatr (Rio J). 2019;95:209–16.
Study linked to “Ligue 132” (“Call 132”) phone service, Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Porto Alegre, RS, Brazil.




