
Verify the association between metabolic risk profile in students with different levels of cardiorespiratory fitness and body mass index, as well as the nutritional status of their parents.
MethodsA cross-sectional study comprising 1.254 schoolchildren aged between seven and 17 years. The metabolic risk profile was calculated by summing the standardized values of high density lipoproteins and low density lipoproteins, triglycerides, glucose and systolic blood pressure. The parents’ nutritional status was evaluated by self-reported weight and height data, for body mass index calculating. The body mass index of schoolchildren was classified as underweight/normal weight and overweight/obesity. The cardiorespiratory fitness was assessed by 9-minute running/walk test, being categorized as fit (good levels) and unfit (low levels). Data were analyzed using prevalence ratio values (PR).
ResultsThe data indicates a higher occurrence of developing metabolic risk in schoolchildren whose mother is obese (PR: 1.50; 95% CI: 1.01, 2.23), and even higher for those whose father and mother are obese (PR: 2, 79, 95% CI: 1.41; 5.51). Students who have low levels of cardiorespiratory fitness and overweight/obesity have higher occurrence of presenting metabolic risk profile (PR: 5.25; 95% CI: 3.31; 8.16).
Conclusionthe occurrence of developing metabolic risk in schoolchildren increase when they have low levels of cardiorespiratory fitness and overweight/obesity, and the presence of parental obesity.
Verificar se há associação entre o perfil de risco metabólico em escolares com diferentes níveis de aptidão cardiorrespiratória e índice de massa corporal, bem como com o perfil nutricional de seus pais.
MétodosEstudo transversal constituído por 1.254 escolares com idade entre sete e 17 anos. O perfil de risco metabólico foi calculado por meio da soma dos valores estandardizados de lipoproteína de alta densidade e lipoproteína de baixa densidade, triglicerídeos, glicose e pressão arterial sistólica. O perfil nutricional dos pais foi avaliado pelos dados autorreferidos de peso e estatura, calculando-se posteriormente o índice de massa corporal. O índice de massa corporal do escolar foi classificado em baixo peso/peso normal e sobrepeso/obesidade. A aptidão cardiorrespiratória foi avaliada através do teste de corrida/caminhada de 9 minutos, sendo categorizada em apto (bons níveis) e inapto (baixos níveis). Os dados foram analisados através dos valores de razão de prevalência (RP).
ResultadosOs dados apontam maior ocorrência de desenvolvimento de risco metabólico em escolares que apresentam mãe com obesidade (RP: 1,50; IC 95%: 1,01; 2,23) e, maior ainda, em escolares que possuem pai e mãe obesos (RP: 2,79; IC 95%: 1,41; 5,51). Escolares que apresentam baixos níveis de aptidão cardiorrespiratória e sobrepeso/obesidade possuem maior ocorrência de perfil metabólico de risco (RP: 5,25; IC 95%: 3,31; 8,16).
Conclusõesa ocorrência de desenvolvimento de risco metabólico em escolares aumentam quando estes apresentam baixos níveis de aptidão cardiorrespiratória e sobrepeso/obesidade, assim como na presença de obesidade dos pais.
The rapid increase in the prevalence of overweight and obesity in Brazilian children and adolescents1 has resulted in a growing interest about the role of lifestyle in the development of the metabolic risk profile (MRP) in children and adolescents. Based on the records of this alarming increase in overweight and obesity, their consequences for health have been demonstrated, such as the occurrence of metabolic syndrome (MS), which represents a condition of adulthood related to cardiovascular morbidity. However, MS has also been identified in children and adolescents, showing a direct association with excess weight.2–4 Studies have shown that metabolic risk develops during childhood and adolescence, leading to an increased risk of cardiovascular events and occurrence of type 2 diabetes.2,3
Consequently, studies that aim to explore the risk factors of cardiovascular diseases in children and adolescents are being emphasized, focusing on the centralization of prevention – considering, in addition to the life styles of young individuals, the influence of family involvement.5 It has therefore been verified that adults with low cardiorespiratory fitness are associated with cardiovascular risk factors such as hypercholesterolemia, obesity, and type 2 diabetes.6 However, the evidence is not yet clear in children and adolescents, but suggests that the association between obesity and cardiovascular risk is mediated by aerobic fitness since childhood.7 It can also be observed that the cardiometabolic risk is higher in children and adolescents with overweight and obesity who perform light physical activity than in those who practice vigorous activity.8
Several studies have shown that low cardiorespiratory fitness (CRF) is a significant independent risk factor for future cardiometabolic disease in adulthood. No less importantly, it is suggested that the parental nutritional profile is an important predictor of overweight and obesity in children and adolescents.9 Nevertheless, considering the consequences of this disorder, there is already evidence of an association between the parents’ lifestyle and nutritional profile with an early risk of developing a metabolic risk profile.10,11 The possibility of obese parents of having children with high cardiometabolic risk is explained by the likely influence not only of family involvement, but also of genetic factors, which account for approximately 30%–40% of factors responsible for early development of diseases in childhood and adolescence. However, it is worth mentioning the importance of focusing research on factors related to lifestyle, both of young individuals and their parents, in order to obtain data to better organize interventions.
The above statements justify the importance of studies that seek to understand the early development of MS in children and adolescents and the need to include a large number of potential associated factors. Thus, it is suggested that low cardiorespiratory fitness may be an independent risk factor for future cardiometabolic disease in adulthood.12 Nevertheless, when prevention is considered, some factors have been highlighted as being both important and modifiable, results that justify the need to comprehend the association between obesity7 and parents’ nutritional profile11vs. cardiorespiratory fitness in a young Brazilian population.
Thus, the present study aims to determine whether there is an association between MRP in students with different levels of cardiorespiratory fitness (CRF) and body mass index (BMI), as well as with the nutritional status of their parents.
MethodsThe population of schoolchildren and adolescents consists of approximately 20,540 students, from public and private elementary and high Schools, of whom 11,679 are state-operated, 6813 are municipal, and 2048 are private school located in the municipality of Santa Cruz do Sul, state of Rio Grande do Sul, Brazil, stratified by rural and urban areas and the latter by downtown and periphery: north, south, east, and west. Data were collected from the 6th Regional Coordinator of Education and the Municipal Secretariat of Education of Santa Cruz do Sul. To be representative of the municipality, a sample of approximately 400 students was estimated, based on a statistical power of 0.80, a level of significance of 5%, and the prevalence of overweight and obesity of approximately 30% for Brazilian children and adolescents.1
This research is part of a longitudinal study called Schoolchildren's Health, consisting of a random sample by conglomerates of approximately 2000 schoolchildren and adolescents, aged 7–17 years, attending 19 schools (center, north, south, east, and west of the rural area) of the municipality of Santa Cruz do Sul-RS. Of these, 1254 participated in this study, considering as inclusion criterion the students’ complete data regarding the selected variables, as well as their parents’. Thus, students whose parents did not report their weight and height, those who did not allow the collection of blood, and those who had a physical problem that prevented them from performing the test to assess CRF were removed from the sample.
After providing detailed information about the project and explanations about the procedures to which the schoolchildren and adolescents would be submitted, all participants provided the informed consent signed by parents/guardians, agreeing to participate in the study, which was approved by the Ethics Committee of Universidade Santa Cruz do Sul – UNISC under No. 2525/10.
The nutritional profile of parents was self-reported through a survey that included their height and weight for subsequent BMI calculation, which was classified according to the World Health Organization criteria13 as normal BMI (18.50–24.99kg/m2), overweight (25.00–29.99kg/m2), or obesity (≥30.00kg/m2).
Blood was collected through venipuncture by a trained technician after eight hours of fasting. Blood samples were centrifuged and the serum was stored in pre-labeled Eppendorf tubes at −20°C until the time of the analysis. The biochemical analyses (glucose, high-density lipoprotein [HDL], and triglycerides [TG]) were performed using DiaSys commercial kits (DiaSys Diagnostic Systems, Germany), in a Miura One device (I.S.E., Rome, Italy). Low-density lipoprotein (LDL) was calculated according to the Friedewald–Fredrickson–Levy formula.14
For blood pressure assessment, the parameters of the VI Brazilian Guidelines on Hypertension15 were used, based on the auscultatory method, with aneroid devices calibrated for less than three months at the time of the evaluations. The researchers had three different cuff sizes in order to select the most suitable cuff for the circumference of each arm, while considering a width/length proportion of 1:2.
CRF was assessed by the distance traveled by the student (in meters) using the nine-minute walk/run test carried out on a race track, according to the protocol recommended by the Sport Brazil Project.16 Subsequently, subjects were categorized into good levels (fit) and low levels (unfit) of cardiorespiratory fitness, according to the cutoff point of PROESP-BR (Project Sport Brazil),16 considering gender and age.
BMI was defined by applying the formula: BMI=weight/height2 (kg/m2). Weight and height were evaluated in the early morning in fasting state, with the subject wearing light clothing and no shoes. BMI classification followed the protocol for Brazilian children and adolescents, established by Conde and Monteiro,17 considering the categories underweight/normal weight and overweight/obese for this study.
The CRF/BMI association was established considering the following categories: 1) fit/low weight-normal weight; 2) fit/overweight-obesity; 3) unfit/low weight-normal weight; 4) unfit/overweight-obesity.
The metabolic risk was calculated by the sum of the standardized values (Z-score) of each of the risk factors for cardiovascular disease: HDL and LDL, TG, glucose, and systolic blood pressure (SBP), not including the BMI. The Z-score of HDL was multiplied by −1, as it indicates an inverse association with cardiovascular risk factors. MRP was considered when values were equal to or greater than one standard deviation, according to the criteria established by Andersen et al.18 and used by Mota et al.19
Data were analyzed in the statistical program SPSS (IBM SPSS Statistics for Windows, Version 23.0. IBM Corp., NY, USA). Descriptive analyses are shown as mean/standard deviation and frequency for categorical variables. The prevalence ratio between the MRP and the independent variables was calculated using bivariate logistic regression models, considering the high MRP values as the risk category to calculate the prevalence ratio The model included the following predicting factors: BMI/CRF and BMI of the parents. The risk categories were used as reference categories. All models were adjusted for age. Knowing that several factors are associated with the development of the MRP, such associations were analyzed by multivariate analysis, whereupon multiple variables are analyzed in a single association.20 Thus, different regression models were assessed, considering the possibility of error associated with multicolinearity between three variables: father's BMI, mother's BMI, and parents’ BMI. A 5% significance level was considered for all analyses.
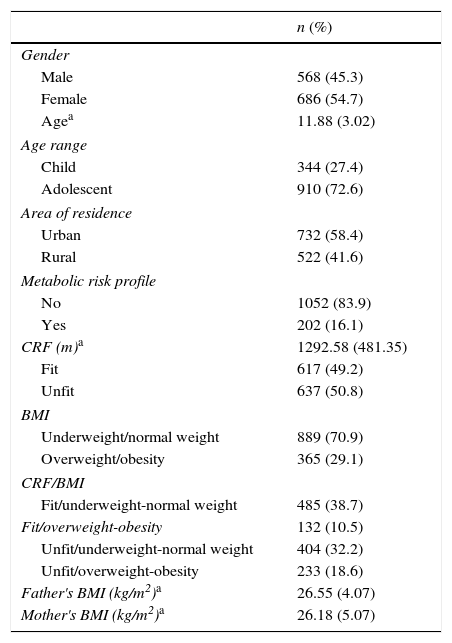
ResultsTable 1 shows the characteristics of the subjects that comprise the study sample. A total of 1254 schoolchildren and adolescents participated in the study; of these, 27.4% were children and 72.6% adolescents; the mean age was 11.88 years, 54.7% were females, and 58.4% lived in the urban area. It can be observed that 16.1% of the students had metabolic risk, 50.8% had low levels of CRF, and 29.1% had overweight/obesity.
Descriptive characteristics of the subjects.
| n (%) | |
|---|---|
| Gender | |
| Male | 568 (45.3) |
| Female | 686 (54.7) |
| Agea | 11.88 (3.02) |
| Age range | |
| Child | 344 (27.4) |
| Adolescent | 910 (72.6) |
| Area of residence | |
| Urban | 732 (58.4) |
| Rural | 522 (41.6) |
| Metabolic risk profile | |
| No | 1052 (83.9) |
| Yes | 202 (16.1) |
| CRF (m)a | 1292.58 (481.35) |
| Fit | 617 (49.2) |
| Unfit | 637 (50.8) |
| BMI | |
| Underweight/normal weight | 889 (70.9) |
| Overweight/obesity | 365 (29.1) |
| CRF/BMI | |
| Fit/underweight-normal weight | 485 (38.7) |
| Fit/overweight-obesity | 132 (10.5) |
| Unfit/underweight-normal weight | 404 (32.2) |
| Unfit/overweight-obesity | 233 (18.6) |
| Father's BMI (kg/m2)a | 26.55 (4.07) |
| Mother's BMI (kg/m2)a | 26.18 (5.07) |
CRF, cardiorespiratory fitness; BMI, body mass index.
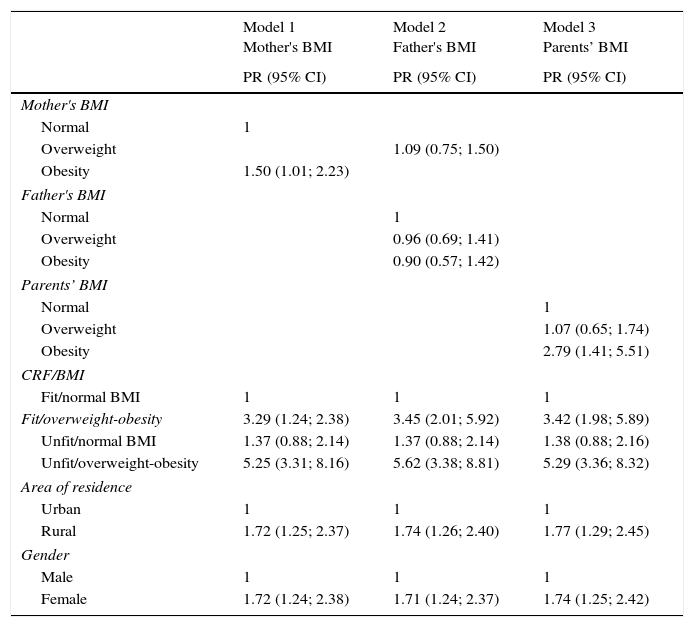
Table 2 shows three models of binary logistic regression, taking into account that the independent variables, which represent the parents’ characteristics, show a high association with each other (multicolinearity). All models were adjusted for the area of residence, age and gender of the subject, and also contain the grouped variables CRF/BMI. The results show higher incidence in students whose mothers had obesity (PR: 1.50; 95% CI: 1.01, 2.23) – model 1, and even higher in students who had an obese father and mother (PR: 2.79; 95% CI: 1.41, 5.51) – model 3. There was no association between the fathers’ obesity and their children's MRP – model 2.
Association between CRF, BMI, mother's BMI, father's BMI and parents’ BMI with students’ metabolic risk profile.
| Model 1 Mother's BMI | Model 2 Father's BMI | Model 3 Parents’ BMI | |
|---|---|---|---|
| PR (95% CI) | PR (95% CI) | PR (95% CI) | |
| Mother's BMI | |||
| Normal | 1 | ||
| Overweight | 1.09 (0.75; 1.50) | ||
| Obesity | 1.50 (1.01; 2.23) | ||
| Father's BMI | |||
| Normal | 1 | ||
| Overweight | 0.96 (0.69; 1.41) | ||
| Obesity | 0.90 (0.57; 1.42) | ||
| Parents’ BMI | |||
| Normal | 1 | ||
| Overweight | 1.07 (0.65; 1.74) | ||
| Obesity | 2.79 (1.41; 5.51) | ||
| CRF/BMI | |||
| Fit/normal BMI | 1 | 1 | 1 |
| Fit/overweight-obesity | 3.29 (1.24; 2.38) | 3.45 (2.01; 5.92) | 3.42 (1.98; 5.89) |
| Unfit/normal BMI | 1.37 (0.88; 2.14) | 1.37 (0.88; 2.14) | 1.38 (0.88; 2.16) |
| Unfit/overweight-obesity | 5.25 (3.31; 8.16) | 5.62 (3.38; 8.81) | 5.29 (3.36; 8.32) |
| Area of residence | |||
| Urban | 1 | 1 | 1 |
| Rural | 1.72 (1.25; 2.37) | 1.74 (1.26; 2.40) | 1.77 (1.29; 2.45) |
| Gender | |||
| Male | 1 | 1 | 1 |
| Female | 1.72 (1.24; 2.38) | 1.71 (1.24; 2.37) | 1.74 (1.25; 2.42) |
CRF, cardiorespiratory fitness; BMI, body mass index; fit, good levels of cardiorespiratory fitness; unfit, low levels of cardiorespiratory fitness.
Models 1, 2 and 3 were adjusted for age.
Nagelkerke R Square: model 1 (7.4%), model 2 (7.1%) and model 3 (13.4%).
An association was observed in all models for the CRF/BMI variable, considering as reference category the fit/low weight-normal weight students. High metabolic risk was found both in unfit/overweight-obesity (PR: 5.29; 95% CI: 3.31, 8.16) and fit/overweight-obesity students (PR: 3.42; 95% CI: 1.24, 2.38). This study did not verify an increased risk in unfit/low weight-normal weight in comparison to fit/low weight-normal weight students.
Regarding the students’ characteristics, girls (PR: 1.74; 95% CI: 1.24, 2.38) and residents of the rural area (PR: 1.77; 95% CI: 1.25, 2.37) had a higher incidence of MRP development. On the other hand, birth weight, time of breastfeeding, and age were not associated with MRP.
DiscussionThis study aimed to determine whether there is an association between levels of CRF/BMI and parents’ nutritional profile with students’ MRP. It was observed that children and adolescents with an obese father and mother had higher incidence of MRP in comparison to those who had only the father or mother with obesity. It is noteworthy that these results were independent from the CRF/BMI levels of the young individuals. However, satisfactory aerobic fitness levels were shown to be an important mediator of the risk of obese young individuals to develop MRP.
The multifactorial causes of early cardiovascular risk factor development in childhood have been demonstrated in recent years.21 In addition to the genetic contribution to the development of cardiovascular risk factors,22 parental behavior has been strongly associated with the behavior adopted by their children.11 Studies indicate a significant association of parental nutritional profile with overweight and obesity in their children.9,23 In fact, the importance of parents’ obesity as a predictor for obesity in their children seems clear.
A study by Efstathiou et al.10 carried out in Greece, including a sample of children and adolescents and their parents, obtained as the main result the possibility of low weight, reduced head size, and family history of overweight and obesity as possible factors associated with the detection of children with chance of developing MRP in adolescence. It should be noted that this study used a metabolic risk score similar to that used in this study; however, contrary to the present results, low birth weight was the main predictor. Another study found that obesity in childhood increases the cardiometabolic risk profile, but satisfactory levels of cardiorespiratory fitness tend to attenuate the association between obesity and cardiometabolic risk.24
As a result of these statements, studies that indicate the chances of children and adolescents who have a parent or both parents with overweight and obesity developing not only early overweight and obesity, but additionally a metabolic risk profile, are highlighted.10,11,25 In the present study, there was a higher occurrence of students who had an obese father and mother in the development of early metabolic risk profile. Additionally, it was found that when analyzed individually, only the mothers’ behavior was associated with the children's, while the fathers’ behavior does not show such association. In the study by Jiang et al.,9 the mothers’ nutritional profile showed a strong association with their children's obesity. As justification for these results, the authors suggest the possibility that mothers are usually more involved in their children's daily activities and feeding habits and, thus, can have a higher influence than the parents’ lifestyle.
However, other factors that comprehend the lifestyle of children and adolescents have been suggested as risk factors for early development to cardiovascular diseases. In this context, Khanolkar et al.11 observed that both the smoking habits of parents as well as the physical activity levels were shown as predictors of cardiovascular disease risk factors. These results explain the limitations of the present study, as it only analyzed the parents’ nutritional profile, which indicate, along with the CRF/BMI ratio, a variance in the MRP of approximately 15%, confirming the need to include other variables that may explain this early metabolic risk, together with certain genetic characteristics. Nevertheless, it appears important to suggest that obesity vs. low levels of aerobic fitness added to the parents’ obesity were able to explain almost one-third of what is expected to be the non-genetic contribution to metabolic syndrome in young individuals.
Additionally, the present study observed a strong association between CRF/IMC with the MRP of the students, and the occurrence of MRP in unfit students with overweight/obesity was higher compared those who were fit and had normal BMI. However, contrary to what was expected, and in accordance with what was suggested by Eisenmann et al.,7 children and adolescents with normal BMI, but with low CRF, did not show a higher incidence of MRP in relation to those with good levels of CRF and normal BMI. That is, it appears that normal weight in children and adolescents is considered a prevalent factor of cardiometabolic risk when compared with the role of aerobic fitness.
However, the occurrence of MRP among children and adolescents with overweight and obesity was attenuated by healthy levels of CRF. That is, while children and adolescents with overweight and obesity who were unfit showed a 5-fold higher occurrence of MRP development in relation to fit children with underweight/normal weight, those with overweight and obesity that were fit had a lower occurrence, approximately three-fold lower. Therefore, it is suggested that, in accordance with the study by Eisenmann et al.,7 particularly in children and adolescents with overweight and obesity, maintaining a healthy level of CRF seems to protect against the early development of risk factors for cardiovascular disease.
The results of this study suggest that changes in lifestyle are crucial to modify harmful behaviors that may trigger metabolic risks. Among the lifestyle factors, it was possible to observe the important role of favorable levels of aerobic fitness as prevention of early development of cardiometabolic factors, especially among young individuals that have the highest risk, i.e., the obese. Thus, the school is seen as an ideal setting to modify habits, particularly those related to dietary factors, promotion of an active life, reduction in sedentary activities, and the attainment of adequate levels of physical fitness, variables that are important for health such as flexibility, strength, agility, and aerobic fitness. Thus, the regular practice of physical exercise and the promotion of an active life must be supported at school and should start to be regarded as an enjoyable practice, offered to all children and adolescents at moderate and appropriate amounts for each age group.26
Finally, the occurrence of metabolic risk development is higher in girls among students from rural areas and, in fact, both the parents’ BMI and CRF/BMI ratio are important predictors associated with risk factors for cardiovascular disease in students. It is worth mentioning the two important findings of this study: children with obese fathers and mothers are at greater risk than their peers with only an obese mother or father and, furthermore, a high level of cardiorespiratory fitness seems to be a protective factor in a population already at risk, as in the case of children and adolescents with overweight and obesity.
However, it should be noted that the present study has some limitations. Direct assessment of the parents’ weight and height could not be performed due to the large sample of students evaluated in the study; so we chose the self-reported information of these variables by the parents, allowing the calculation of BMI. Also, the students’ sexual maturation stage was not assessed, with sexual dimorphism being capable of influencing the analyzed associations. Despite some limitations, this study reinforces the importance of the associations found and suggests that experimental studies be performed to establish a cause-and-effect association.
We conclude that the parents’ nutritional profile, as well as obesity and low levels of cardiorespiratory fitness are risk factors for early development of metabolic risk in children and adolescents and should be considered in future intervention studies.
FundingUniversidade de Santa Cruz do Sul (UNISC).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Todendi PF, Valim AR, Reuter CP, Mello ED, Gaya AR, Burgos MS. Metabolic risk in schoolchildren is associated with low levels of cardiorespiratory fitness, obesity, and parents’ nutritional profile. J Pediatr (Rio J). 2016;92:388–93.





