

Developing and validating a disease-specific instrument in the Brazilian Portuguese language to assess the Health-Related Quality of Life of children with functional constipation, applied to parents/caregivers.
MethodsThe process of developing the questionnaire was carried out in the following steps: items generation concerning functional constipation; elaboration of the preliminary questionnaire; assessment by health professionals; identifying problems or inconsistencies by the researchers; improvement of the questions; obtaining a final questionnaire named Pediatric Functional Constipation Questionnaire-Parent Form (PedFCQuest-PR) with 26 questions divided into four domains. Responses options use a Likert scale based on the events of the last four weeks. The process of validation was an observational, cross-sectional study in a sample of 87 parents/caregivers of children from 5 to 15 years of age diagnosed with Functional constipation according to the Rome IV Criteria. The questionnaire was applied simultaneously to the Pediatric Quality of Life Inventory 4.0 (PedsQL TM 4.0) as a control.
ResultsThe questionnaire validation included 87 parents/caregivers. The children's median age was 8.2 years, with a long time of constipation symptoms associated with fecal incontinence in approximately two-thirds. Internal consistency reliability for the Total Scale Score of PedFCQuest-PR by Coefficient Alpha of Cronbach score was 0.86. Convergent and divergent validity of PedFCQuest-PR was demonstrated by correlating the domains of both questionnaires.
ConclusionThis study provides evidence that PedFCQuest-PR is a reliable instrument. The results showed a high degree of internal consistency and validity of the instrument for future applications.
Pediatric Functional Constipation (PFC) is a major global health problem with a reported pooled prevalence of 9.5% (95% CI 7.5-12.1).1 In Brazil, the prevalence varies from 10 to 18%.2,3 Additionally, PFC occurrence is associated with geographical location, lifestyle factors, and is more related to physical and psychological trauma, school-related, family-related, stressful life events (health problems of a sibling, illness of a member of the family, less outdoor play).4 Certainly, PFC is challenging to treat, and around 25% maintain symptoms until adulthood.5
The Health-Related Quality of Life (HRQoL) of PFC was evaluated in few pediatric studies.6,7 In the study's setting, applying a generic form, the Child Health Questionnaire-Parent Form, a significant decrease in psychological and physical well-being aspects of PFC was observed.8 Recently, a systematic review showed that HRQoL pooled total scores of PFC were lower compared with the healthy reference.9
Assessment of HRQoL, in both research and clinical practice, can facilitate communication; discover problems that affect these patients, help improve patient's symptoms, and rehabilitation. Thus, this study is devoted to two objectives: First, development, and Second, validation a disease-specific instrument in the Brazilian Portuguese language to assess HRQoL in Pediatric Functional Constipation.
MethodsFirst objective. Questionnaire developmentThis questionnaire was developed in ten steps, according to literature recommendations.10–12
Step 1. “Constipation”, “HRQoL” and “Questionnaires” were used as keywords to search related terms on Pubmed and Scielo databases.
Step 2. A literature review related to these terms was conducted to generate 420 phrases. Translation from English into Portuguese was done considering the cultural adaptation, by authors of the study with fluency in English and Portuguese.
Step 3. The list of phrases was converted in the Preliminary Questionnaire (PQ) 1, with 57 questions divided into five domains: physical, emotional, social, school and family; including a general health question and a question about the children's behavior. The questions were directed to events of the last four weeks, considering the diagnosis of PFC through the Rome IV Criteria.13 The answer options were organized on a four-point Likert scale format assessing frequency (0 = never; 1 = occasionally; 2 = frequently; 3 = always), intensity (0 = nothing; 1 = little; 2 = quite; 3 = extremely), agreement (0 = completely disagree; 1 = partially disagree; 2 = partially agree; 3 = completely agree) and quality/rating (0 = very poor; 1 = poor; 2 = good; 3 = very good).
Step 4. On PQ 2, redundant, inappropriate words or questions were eliminated. All steps were discussed between the authors of the study and two more guests (a general pediatrician with experience in treating children with constipation and a child psychologist who works in specific constipation outpatient clinics). The meetings were specific and discussed until consensus was reached on the topic to be excluded, included, or modified in the questionnaire. In addition, terms that induce a specific response, negative phrases, vague words, double meaning, and indefinite questions were avoided, resulting in 37 questions.
Step 5. On PQ 3 the quality of the questions was improved, organized from the easiest to the most difficult, from concrete to abstract, from least to most sensitive. In addition, short sentences and straightforward words were used to the level of respondents. Besides, were emphasized essential words, using bold, and the number of the questions reduced, considering an ideal literature number from 15 to 30 questions.
Step 6. PQ 4 was a semi-structured questionnaire with 26 questions and submitted simultaneously to 11 health professionals experienced in pediatric care in order to improve the clarity of the questionnaire.
Step 7. On PQ 5 the domains were renamed to Physical, Behavioral (formerly Emotional), Social (including questions from the previous "Family" domain), and School, with 26 questions. The answer options, organized on a four-point Likert scale format, were interspersed with standardization for even and odd questions.
Step 8. PQ 5 was administrated to 45 parents/caregivers (40 mothers, 01 father and 04 caregivers), and a semi-structured interview was conducted, to assess the acceptability, comprehensiveness, clarity of writing, relevance, and ambiguity of items. Test-retest reliability was evaluated at this step in nine mothers with 7 to 14 days between requests. There was no statistical difference between responses for the total score and Items (p > 0.05).
Step 9. After a few adjustments in language, the specific HRQoL questionnaire was titled "The PFCQuestionnaire - Parent Report" (PedFCQuest-PR), consisting of 26 questions considering four domains: Physical, Behavioral, Social and School; including a general health question and a question about the child's behavior. The answers were organized in a four-point Likert scale, assessing frequency, intensity, agreement, and quality.
Step 10. The Questionnaire PedFCQuest-PR was qualified in forty-five parents/caregivers in a preliminary study.
Second objective. Questionnaire validationAfter questionnaire development, a single-center, observational, cross-sectional study for the validation of PedFCQuest-PR applied to parents/caregivers of a convenience sample of consecutive cases of children/adolescents, referred from 2018 to 2019, from the same geographic area to a tertiary outpatient Pediatric Gastroenterology Clinic of the Brazilian Public Health System (SUS).
Inclusion criteria for parents/caregivers were aged over 18 years, able to understand and answer the questionnaire alone, knowledge of the children's clinical condition, living in the same home as the patient, and sign the Informed Consent Form. Inclusion criteria for children were age between 5 and 15 years old, diagnosis of PFC according to the Rome IV Criteria[13] and toilet trained. Exclusion criteria were chronic health problems (neurological, genetic, psychiatric, surgical, growth, and development disorders). The Ethics Committee (CAAE 90158218.0.0000.5411) approved this study.
Data collectionThe sociodemographic and anthropometric data were collected on a standardized clinical form developed according to the Rome IV criteria for pediatric Functional Gastrointestinal Disorders. Stool characteristics were obtained with Bristol Stool Consistency Scale translated and adapted for the Brazilian Portuguese.14 Experienced pediatric nurses obtained anthropometric measurements at the first visit, according to the World Health Organization (WHO) guidelines.15 BMI (kg/m2) and z score were evaluated according to the WHO growth standards adjusted for sex and age.16,17
PedsQLTM 4.0 Generic Cores Scales Parent Proxy-Report (PedsQL 4.0)18,19 have age-appropriate questionnaires for the young child (5–7y), child (8–12y), and adolescent (13–18y). The instrument encompasses 23 items in four domains: Physical Functioning (8 items), Emotional Functioning (5 items), Social Functioning (5 items), and School Functioning (5 items). This instrument was adapted cross-culturally and validated for use in Brazilian Portuguese exhibiting good psychometric properties.20 PedsQL 4.0 was used for validation of PedFCQuest-PR, and permission was obtained from the Mapi Research Trust.
ProceduresBoth questionnaires, PedFCQuest-PR (Supplementary Material A) and PedsQL 4.0, were self-administered simultaneously in a printed form during the first visit, in a private room, and before medical treatment. If the parent/caregiver did not understand the meaning of any question, the researcher read the question slowly, without using synonyms or giving explanations. After receiving the questionnaire already answered, the researcher checked that there is no more than one answer per question. In both questionnaires, the items were reverse-scored and linearly transformed to a 0 to 100 scale. The sum of the values attributed to each item was calculated as a total score, and the lowest values indicated HRQoL impairment.
Statistical analysis and psychometric properties of the PedFCQuest-PRInstrument validationThis step proposes to evaluate the psychometric properties of the instrument.21 The scales were considered to be absent of floor or ceiling effects if <15% of the sample scored either the lowest possible score (floor effect) or the highest possible score (ceiling effect). Reliability analysis was measured using Cronbach's alpha coefficient. It provides an estimate of reliability based on all possible correlations between two sets of items. The higher the internal consistency, the most significant congruence occurs between the items. However, if the value were very high, it would mean that there is redundancy between the items. The reference value acceptable (excellent reliability) must be equal to or greater than 0.70 and at a maximum of 0.90.12
Validity describes how much a measure represents the attribute to be calculated and how much it captures the concept that will be the target. Construct Validity was assessed by correlating the same domains of both questionnaires. It was hypothesized that more severe scores in the PedFCQuest-PR would be associated with greater impairment of PedsQL 4.0 scores. Researchers consider that mean values of correlation greater than 0.30 are adequate and, therefore, measure the same construct. Convergent and divergent Validity is based on the patterns of correlations among the measures. Convergent validity was expected to be moderate (0.30 < r < 0.50) or large (r > 0.50), and divergent validity to be relatively weak (r < 0.30).
Content validity involves a critical examination of the basic structure of the instrument, considering the applicability to the intended research question. It is mostly a qualitative study. Therefore, it is not statistically determined. Furthermore, Criterion validity estimates the extent to which a measure agrees with an external criterion, as another established instrument that is widely accepted or considered "gold standard" for the construct being evaluated.
Descriptive statisticsThe analysis was performed with GraphPad Prism version 8.4.0 for Windows (GraphPad Software, USA). The normality of data was tested with the Kolmogorov-Smirnov test. Continuous variables were analyzed with the Mann-Whitney test and the categorical data with Fisher's exact test. The Validity of the PedFCQuest-PR was analyzed using Spearman's correlation coefficient. Value of r (positive or negative) can be interpreted as a magnitude correlation between variables, and r values are designated as small (0.10), medium (0.30), and large (> 0.50). The statistical tests were two-tailed, and the level of significance was set at p < 0.05.
ResultsQuestionnaire validationSupplementary Fig. 1 presents the flow diagram of 142 parents/caregivers of children with FC involved in the study. Forty-five participate in the Questionnaire development, and 87 in the Questionnaire validation. The PedFCQuest-PR and PedsQL 4.0 were self-administered, highly suitable with low refusal or difficulty in answering (only 04 parents/caregivers). There were no missing item responses.
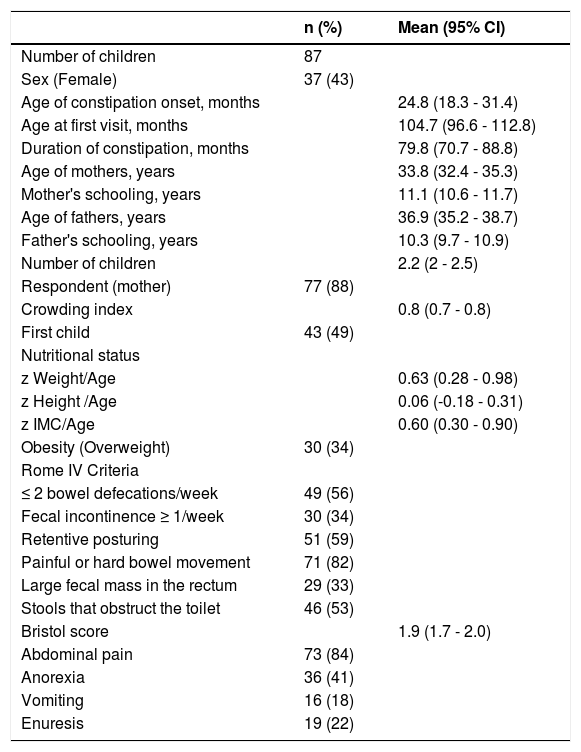
Table 1 presents the baseline characteristics of the participants on questionnaire validation. The results demonstrate small families, mothers as respondents, and schoolchildren with prolonged duration of symptoms. Comparison analysis of total score of PedFCQuest-PR for the presence/absence of different Rome IV criteria demonstrated a significantly lower score for the children with ≤ 2 bowel defecations/week (p < 0.0001), fecal incontinence ≥1/week (p < 0.0001), retentive posturing (p < 0.01), large fecal mass in the rectum (p < 0.04), and large-diameter stools which can obstruct the toilet (p < 0.006). In a similar analysis using the PedsQL 4.0 total score, only the children with fecal incontinence ≥1/week showed a significantly lower score (p < 0.001). There was no statistical difference in comparison the total score of both questionnaires for sex, children age (< 8 vs > 8.3 years), duration of constipation (< 71 vs > 71 months), blood in the stool, and the presence of enuresis. There was a statistical difference in the presence of abdominal pain in both PedFCQuest-PR (p = 0.02) and PedsQL 4.0 (p = 0.03). No baseline characteristics of children and responders differed between the Questionnaire development (n = 45), and Questionnaire Validation (n = 87).
Baseline characteristics of children of the Final study.
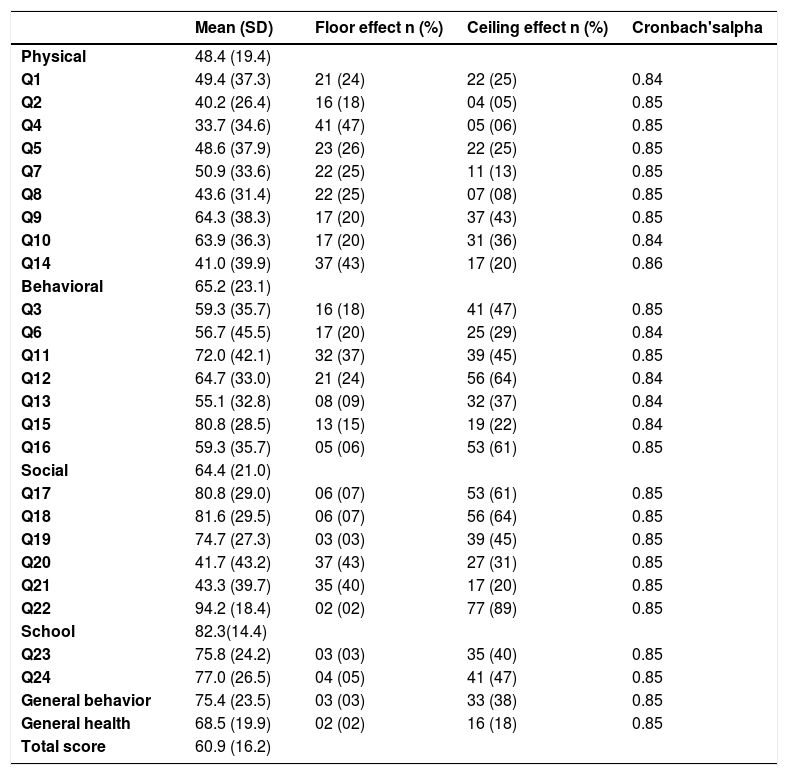
Table 2 presents PedFCQuest-PR results of ceiling effects in all domains. The Physical domain presents items with the lowest score values. The Cronbach's alpha was very adequate for all Items.
PedFCQuest-PR: Domains, Items, Floor, Ceilings effects, and Cronbach's alpha
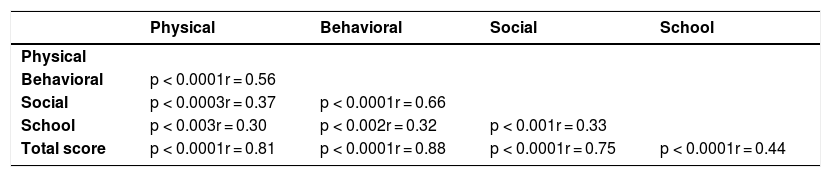
The reliability analysis was analyzed using Cronbach's alpha coefficients (Table 2) for the different items of PedFCQuest-PR, which were between 0.84 and 0.86, with a median of 0.85. Table 3 presents a statistically significant positive correlation coefficient between the total score and different domains and inter domains of PedFCQuest-PR. All correlations were positive, statistically significant and with medium (r > 0.30) and large (r > 0.50) values. In particular, Physical, Social, Behavior and Total scores are large. Table 4 presents the correlation between similar domains of PedFCQuest-PR and PedsQL 4.0. All results are positive, convergent and demonstrate a statistically significant medium value (r > 0.30), except for Physical domain (r = 0.25). On items correlation analysis between both questionnaires, all similar items correlations were statistically significant with moderate intensity (r > 0.30; p < 0.001). On different items, there were no statistically significant differences.
Content validity was evaluated, exposing the questionnaire to a group of pediatric specialists,22 and during the application of preliminary questionnaires (Steps 7 and 8), in order to construct the final questionnaire (PedFCQuest-PR). There was a minimum of suggestions for correction, suppression or addition of the items, as well as changes in domains. Criterion validity is rarely used due to the lack of a widely accepted criterion measure. This study is the first questionnaire in Brazilian Portuguese to evaluate the HRQoL of children with PFC. Consequently, there is no "gold standard" that can be used for comparison.
DiscussionIn this study, a specific instrument in the Brazilian Portuguese language was developed and validated for the evaluation of HRQoL in children and adolescents with PFC, from the perspective of the parents/caregivers. PedFCQuest-PR was verified to determine the applicability of the instrument to the target group. The comparison analysis of the Total score of PedFCQuest-PR with the presence/absence of Rome IV criteria establishes an association of PedFCQuest-PR and Rome IV criteria. Therefore, incorporate HRQoL and Rome IV criteria could be very applicable.
Developing new instruments is a time-consuming process, involving an extensive literature exploration, elaboration of the questionnaire, interviews with professionals and patients. Indeed, a questionnaire must address some principles to confirm the development of a good questionnaire.23
Fitzpatrick et al.24 identified eight issues that must be addressed when choosing an HRQoL instrument for either a clinical trial or routine clinical practice. Therefore, these issues were considered in the development and validation of PedFCQuest-PR as detailed below.
- 1.
Suitability: Is the content of the instrument appropriate for the questions that the study intends to address? The current study involves careful consideration of the objectives of the study, with particular reference to HRQoL research questions.
- 2.
Acceptability: Is the instrument acceptable to patients? Pragmatically the best measure of acceptability of PedFCQuest-PR is the result of obtaining complete data from the mothers. According to the methodology, the same researcher always checked the PedFCQuest-PR before releasing the patient. The acceptability can be assessed in response rate and the percentage of the sample that complete the questionnaire.
- 3.
Feasibility: Is the instrument easy to administer and process? The impact of administration, collection and processing of instrument information on the research team was minimal and with no additional effort.
- 4.
Validity: Does the instrument measure what it intends to measure? A group of experts in clinical Pediatrics analyzed the Content validity, and the adjustments were minimal. The Criterion validity consists of the relationship between the scores of a given instrument and some external criterion. There is not a questionnaire to assess HRQoL in children with PFC in the Brazilian Portuguese language as a “gold standard”. Accordingly, PedsQL 4.0 was chosen as an external criterion, which has already been used by previous studies in children with functional constipation.25–28
The correlations within the PedFCQuest-PR questionnaire showed that the Total score versus different domains was very strong/moderate, which suggests that there is considerable convergence in the association between these scores. The next step involved comparing the correlations between domains and items of PedFCQuest-PR and PedsQL 4.0, assessing the extent to which they converge or diverge. The correlations of the same domains between both instruments demonstrate positive, but moderate to weak. However, the comparison occurs between domains of specific versus generic instruments. Researchers consider that values of correlation, higher than 0.30 measure the same construct, and are considered adequate.29
- 5.
Reliability: Does the instrument produce reproducible and internally consistent results? In PedFCQuest-PR validation, the internal consistencies with Cronbach's alpha for the total scale were 0.85, and for all items between 0.84 and 0.86. Thus, the authors can conclude that all items were consistent, and they measured the same concept, with no redundancy between the items.
- 6.
Responsiveness: Does the instrument detect changes over time? In the current step of PedFCQuest-PR validation, only a cross-sectional study was done.
- 7.
Accuracy: How accurate are the instrument scores? In the PedFCQuest-PR questionnaire, the answer options, organized on a four-point Likert scale format, were interspersed with standardization for even and odd questions, being reversed alternately to avoid the addiction of response by the respondent. Each item was given equal importance in the score, being transformed into percentages of values between 0 and 100. As an alternative, for the ceiling effect observed, the Likert scale would be extended for five options instead of four.
- 8.
Interpretability: How understandable are the instrument's scores? The PedFCQuest-PR questionnaire was not designed to create a hypothetical subdivision of values in the total score. Another study must analyze a healthy population in order to calculate cutoff values for the questionnaire.
This study has some limitations. First, the sample consists of children who attended a tertiary outpatient clinic. Thus, participants might have had a more prolonged and more severe disease course than children evaluated in communities. Second, the study has no healthy control group, which could be useful in developing a cutoff value. Third, the data presented is from the parent's perspective. However, studies demonstrate that there were no differences between children's form and parent-form questionnaires.30 Fourth, a generic questionnaire was used for comparison with the specific questionnaire. However, there is no specific questionnaire for comparisons validated for the Brazilian Portuguese language. The strengths of this study are the inclusion of children with PFC following Rome IV criteria. Second, this is the first specific instrument to assess the HRQoL of children with functional constipation in the Brazilian Portuguese language.
In conclusion, the PedFCQuest-PR provides evidence and indicates that it is a reliable instrument with a high degree of internal consistency and validity of the instrument. The four domains showed an excellent correlation index with the Total Score, and the domains offer different information about the concerns of families about PFC. Therefore, it can be useful for clinicians, psychologists and researchers, and could be used as a support to health services that want to implement an HRQoL program. Future research is required for the PedFCQuest-PR questionnaire development, such as community assessment, different social and economic classes, multicenter study, and outcomes measurement.
Ethics approvalThe medical, institutional review board approved this study (CAAE 90158218.0.0000.5411).
Consent to participate and for publicationWritten parental informed consent and child assent (when age-appropriate) were obtained for all participants.





