
The aim of this study was to analyze the physical activity level, using two tools, and the functional capacity of children and adolescents with asthma and with different levels of disease control, and to compare them to those of individuals without asthma.
MethodsCross-sectional study with children and adolescents with (asthma group, AG) and without asthma (WAG), aged from 7 to 17 years. All participants performed the six-minute walk test (6MWT), the Glittre Activities of Daily Living test (Glittre-ADL), the International Physical Activity Questionnaire (IPAQ), and daily record of steps on a pedometer.
ResultsThe study included 145 individuals with asthma and 173 individuals without asthma. The WAG walked a greater distance in the 6MWT and performed the Glittre-ADL in less time than the AG. Individuals with uncontrolled, partially controlled, and controlled asthma presented the same functional capacity. A difference was observed in the IPAQ classification, with 13.9% of participants from the WAG being sedentary, compared with 26.2% in the AG. The mean quantity of steps measured by the pedometer was higher in the WAG.
ConclusionThere was a difference in the performance of individuals with and without asthma in the physical activity and functional capacity tests. The AG presented worse performance in the physical activity tests and, regardless of the level of asthma control, presented worse functional capacity.
Asthma is a serious public health problem worldwide and is one of the most common chronic diseases in childhood.1 According to the Pesquisa Nacional de Saúde do Escolar (PeNSE),2 Brazil is currently among the countries with the highest prevalence of asthma, with a rate of 23.2% among students. According to authors, this disease may still be growing in the student population.2
Physical activity plays a fundamental role in the child's normal growth and development, being an essential component in promoting health and quality of life.3 It is recommended for individuals with asthma as it assists in controlling the symptoms, as well as increasing exercise tolerance and cardiorespiratory fitness.4
However, in recent years, there has been a significant reduction in physical activity level and increased sedentary behavior in the pediatric age group.5 In addition, children with uncontrolled asthma generally abstain from playing or exercising for fear of triggering shortness of breath.1
Thus, questioning the influence of asthma control level on functional capacity and the lifestyle adopted by these individuals is important. The six-minute walk test (6MWT)6 and the Glittre Activities of Daily Living test (Glittre-ADL)7 are instruments used to assess functional capacity and detect limitations in the performance of activities of daily living (ADL).
Despite the variety of existing instruments for assessing the level of physical activity, there is still no consensus in research literature on whether individuals with asthma are less active than their healthy peers.8–11 Cassim et al.,11 based on a meta-analysis, evaluated and compared the level of physical activity of children and adolescents with and without asthma, and found no differences between groups. However, the authors included only articles that used pedometers and accelerometers as an assessment tool.
Therefore, the aim of this study was to analyze the level of physical activity using two tools, and the functional capacity of children and adolescents with asthma and with different levels of disease control, and to compare them with individuals without asthma.
Materials and methodsThis was a cross-sectional, observational, clinical study, carried out between July 2017 and December 2018, with children and adolescents between 7 and 17 years of age, approved by the Research Ethics Committee of the Faculty of Medical Sciences of the State University of Campinas, ruling No. 2.121.144. An informed consent was signed by the participants’ legal guardians and adolescents aged over 14 years signed an additional assent form.
Asthma group (AG)Included in this group were all children and adolescents from 7 to 17 years old with a diagnosis of asthma, according to the criteria of the Global Initiative for Asthma (GINA),1 who attended the Pediatric Pulmonology Outpatient Clinic of the State University of Campinas, during the study period. Those with cardiac comorbidities, respiratory diseases with anatomical and structural disturbances proven by auxiliary tests, cognitive or motor limitations that could compromise the test’s performance, and individuals who abandoned the follow-up service between the initial contact and the evaluation day, with no possibility of recruitment for further consultation, were excluded.
Participants underwent clinical evaluation with classification of the level of control and severity of asthma, as well as anthropometric and functional evaluation. To this end, the Asthma Control Test (ACT)12 validated for use in Brazil was applied, which addresses five issues relating to signs, symptom frequency, and use of rescue medication in the last four weeks. The overall score obtained classifies the level of asthma control as follows: ≤19 points, uncontrolled asthma (UA); 20–24, partially controlled asthma (PCA); and 25, controlled asthma (CA).13
The classification of asthma severity, on the other hand, was based on the medication that the participants were using on the day of the evaluation. The GINA1 treatment strategy is based on a step-wise approach; step 1 (low dose treatment for mild asthma) to step 5 (high dose treatment for severe asthma).
Spirometry was performed with the CPFS/D model spirometer (Medical Graphics Corporation — St. Paul, MN, United States). The exams followed the American Thoracic Society and the European Respiratory Society (ERS) criteria14 and the measures of the forced vital capacity (FVC), forced expiratory volume in one second (FEV1), ratio of FEV1/FVC, and forced expiratory flow between 25% and 75% of forced vital capacity (FEF25−75%), were obtained.
All patients were diagnosed with asthma and had been on follow-up consultations for at least six months, and all of them had regularly used controlling drugs for at least three months. The assessment of all children and adolescents in the AG was carried out at the Pulmonary Physiology Laboratory of the Pediatric Research Center at Unicamp. In cases of asthma exacerbation symptoms on the day of the evaluation, the patient was seen by a doctor and the study procedures were rescheduled for another date. All participants were instructed to discontinue medication the night before the exams due to spirometry.
Without asthma group (WAG)The composition of the WAG was conducted in partnership with schools of the region, and as there were many classes and students, support from the coordinators of each school was requested, so that they randomly selected the classes that would participate in the study, stratified by school year. All students belonging to the selected classes received an evaluation form that was given to the legal guardians to complete clinical and demographic information.
In order to rule out the possibility of asthma, the form contained the following questions: (1) Have you had wheezing? (2) Have you had wheezing in the last 12 months? (3) Have you had asthma? (4) In the last 12 months, have you had a dry cough at night without infection from a cold or respiratory illness? Based on the International Study of Asthma and Allergies in Childhood (ISAAC)15 questionnaire and also addressed issues related to wheezing hospitalization, treatment in specialized services for chronic lung diseases and the use of medications to manage asthma such as bronchodilators, inhaled corticosteroids and anti-leukotrienes. In case of a positive answer to questions 2 or 3, the participant was immediately excluded. As for the remaining questions, the exclusion criteria adopted to rule out the possibility of asthma took into account all responses, which provided the team the ability to globally assess the individual's eligibility to participate in the study.
All students who presented the signed consent form were included and all procedures performed in this group took place in the public schools of Louveira, Brazil. Those that presented pulmonary or cardiac diseases, those with motor or cognitive limitations, and individuals that did not complete all the tests were excluded from the study.
Functional capacity evaluationThe functional capacity of participants from the AG and WAG was evaluated by the 6MWT, respecting the ATS6 guidelines. The participant was instructed to walk as quickly as possible, without running, for six minutes. At the end of the test, the total distance walked was recorded. The criteria for discontinuation were intense fatigue or dyspnea, peripheral O2 saturation (SpO2)< 85%, or refusal to continue the exam.
After 30min of rest from the 6MWT, the (Glittre-ADL) was also performed. The test was performed following the protocol described by Martins et al.7 for individuals aged up to 14 years, and that of Skumlien et al.16 for individuals aged over 14 years. It consists of a standardized circuit of 10m in which the participant must perform, in the shortest time possible, a sequence of activities such as walking, going up stairs, moving objects with the upper limbs, and then returning to the starting position to restart the course.
Cardiorespiratory parameters were evaluated before, during, and after the tests using the following: a portable oximeter (Oxy Control — Geratherm®) to measure SpO2 and heart rate, a sphygmomanometer (PA2021 P.A. Med®), and a stethoscope (Classic II S.E. — Littmann®) for blood pressure and chest incursion counting for respiratory rate.
Physical activity level evaluationThe International Physical Activity Questionnaire (IPAQ),17 validated for use in Brazil,21 was used to classify the level of participants’ physical activity into the following categories: “very active,” “active,” “irregularly active,” and “sedentary.” The short version of the questionnaire contains seven questions about frequency (in days per week) and duration (in minutes per day) of vigorous physical activity, moderate physical activity, and walking, which were answered by the participants themselves.
The level of physical activity was carried out by direct monitoring, based on the use of a pedometer (ONwalk 50, Geonaute®), which counts number of steps.11 Participants were instructed to use the pedometer all day, for seven consecutive days before the day of evaluation. The annotation of values was made by the participant themselves in standardized form created for this study, and was subsequently compared with the daily step recommendation proposed by Tudor-Locke et al.18
Statistical analysisThe data were processed using SPSS for Windows, v. 16.0 (SPSS Inc. – Chicago, IL, United States).
The association between qualitative variables was evaluated by the chi-squared test, and complemented, where indicated, by the odds ratio (OR) and its 95% confidence interval.
For comparison of the means of two independent groups, Student’s t-test was used when the data displayed normal distribution. Otherwise, the Mann–Whitney test was used. For comparison of the means of three or more groups, analysis variance (ANOVA) was used, as well as the Bonferroni test where indicated.
In order to complement the bivariate analysis, multivariate models were created by multiple linear regression, using the stepwise forward method. The matrix of correlations of the variables involved was always respected. Development of the simplest model was the starting point, escalating to the most complex ones by considering the biggest gain in the adjusted determination coefficient.
For the dependent variables 6MWT distance, Glittre-ADL time, and pedometer, confounding variables were included in the models: group (asthma; without asthma), age, height, weight, body mass index z-score (z-BMI), sex (male; female), and their interactions. It was ensured that the residues had normal distribution, with a mean of zero in all analyses.
In all cases, a significance level of 5% was adopted.
ResultsThis study evaluated 459 children and adolescents, 256 patients with a diagnosis of asthma and 203 students without asthma. In the AG, 111 individuals were excluded, 12 for refusing to participate, 13 due to a follow-up failure in the service, and 86 due to the presence of comorbidities. In the WAG, 30 were excluded, four due to lack of information, 22 due to a positive report of asthma in the data form, two due to cognitive deficit, and two because they did not complete all the tests. Therefore, 318 individuals remained, 145 composing the AG and 173 composing the WAG.
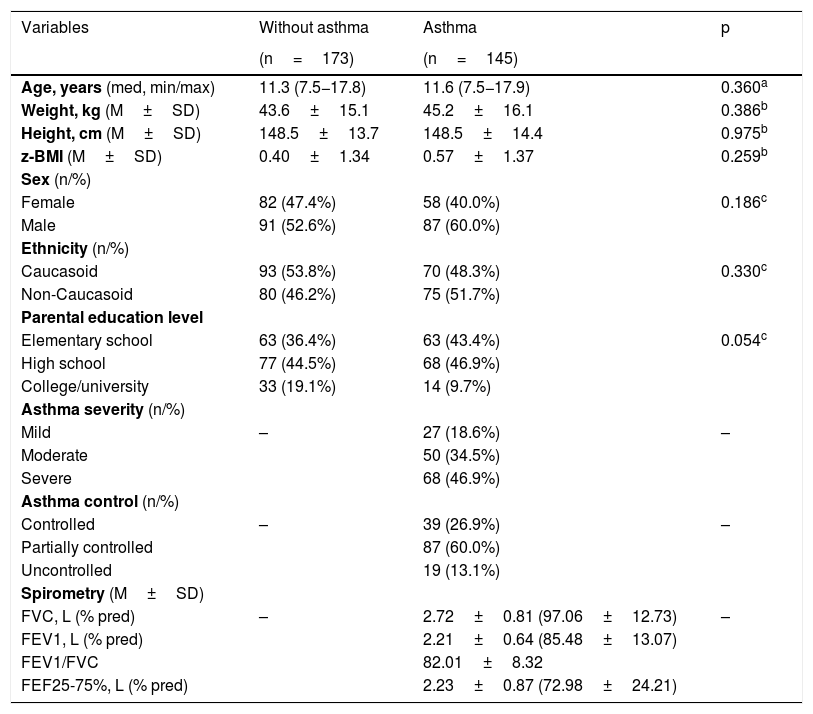
There was no difference between the groups concerning age, height, weight, z-BMI, sex, ethnicity, and level of parental education (Table 1). Regarding the assessment of severity according to the stages of treatment of GINA,1 68 (46.9%) had severe asthma (steps 4 and 5), and as for the assessment of asthma control, 19 (13.1%) were classified as uncontrolled asthma. Spirometry measurements presented by the AG are shown in Table 1.
Characterization of individuals with and without asthma.
| Variables | Without asthma | Asthma | p |
|---|---|---|---|
| (n=173) | (n=145) | ||
| Age, years (med, min/max) | 11.3 (7.5−17.8) | 11.6 (7.5−17.9) | 0.360a |
| Weight, kg (M±SD) | 43.6±15.1 | 45.2±16.1 | 0.386b |
| Height, cm (M±SD) | 148.5±13.7 | 148.5±14.4 | 0.975b |
| z-BMI (M±SD) | 0.40±1.34 | 0.57±1.37 | 0.259b |
| Sex (n/%) | |||
| Female | 82 (47.4%) | 58 (40.0%) | 0.186c |
| Male | 91 (52.6%) | 87 (60.0%) | |
| Ethnicity (n/%) | |||
| Caucasoid | 93 (53.8%) | 70 (48.3%) | 0.330c |
| Non-Caucasoid | 80 (46.2%) | 75 (51.7%) | |
| Parental education level | |||
| Elementary school | 63 (36.4%) | 63 (43.4%) | 0.054c |
| High school | 77 (44.5%) | 68 (46.9%) | |
| College/university | 33 (19.1%) | 14 (9.7%) | |
| Asthma severity (n/%) | |||
| Mild | – | 27 (18.6%) | – |
| Moderate | 50 (34.5%) | ||
| Severe | 68 (46.9%) | ||
| Asthma control (n/%) | |||
| Controlled | – | 39 (26.9%) | – |
| Partially controlled | 87 (60.0%) | ||
| Uncontrolled | 19 (13.1%) | ||
| Spirometry (M±SD) | |||
| FVC, L (% pred) | – | 2.72±0.81 (97.06±12.73) | – |
| FEV1, L (% pred) | 2.21±0.64 (85.48±13.07) | ||
| FEV1/FVC | 82.01±8.32 | ||
| FEF25-75%, L (% pred) | 2.23±0.87 (72.98±24.21) | ||
M±SD, mean±standard deviation; med, min–max; median, minimum–maximum; n/%; sample number/sample percentage.
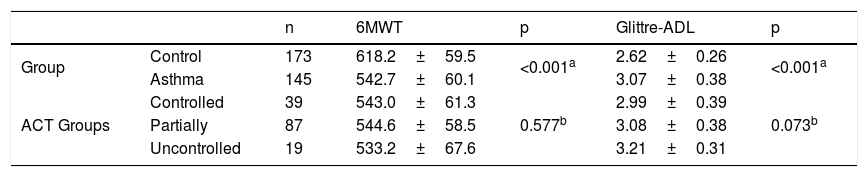
In the 6MWT, the mean distance walked by the WAG was greater than the distance walked by the AG (p<0.001). There was no difference in the distance walked by the AG participants, when compared by the level of asthma control (controlled, partially controlled, and uncontrolled; p=0.577; Table 2).
Distance walked in meters in the six-minute walk test (6MWT) and the required time in minutes for completion of the Glittre Activities of Daily Living test (Glittre-ADL).
| n | 6MWT | p | Glittre-ADL | p | ||
|---|---|---|---|---|---|---|
| Group | Control | 173 | 618.2±59.5 | <0.001a | 2.62±0.26 | <0.001a |
| Asthma | 145 | 542.7±60.1 | 3.07±0.38 | |||
| ACT Groups | Controlled | 39 | 543.0±61.3 | 0.577b | 2.99±0.39 | 0.073b |
| Partially | 87 | 544.6±58.5 | 3.08±0.38 | |||
| Uncontrolled | 19 | 533.2±67.6 | 3.21±0.31 |
Data presented as mean±SD.
ACT, Asthma Control Test.
Comparing the performance of the groups in relation to test Glittre-ADL, it was observed that the WAG needed a shorter mean time to finish the circuit than the AG (p<0.001). Regardless the asthma control level, these individuals showed no difference of performance (p=0.073; Table 2).
Regarding pedometer use, 292 individuals used the device correctly, and a difference was found regarding the mean number of daily steps between the WAG and the AG (p<0.001). The WAG presented a median step count of 7908.0 (3400–21,312) and the median AG step count was 6,426.5 (3326–17,137).
Only 15.1% of children and adolescents in the present study reached the daily step recommendation proposed by Tudor-Locke et al.,18 which is characterized in primary/elementary schoolchildren by 13,000–15,000 steps/day for boys; 11,000–12,000 steps/day for girls, and 10,000–11,700 steps/day for adolescents.
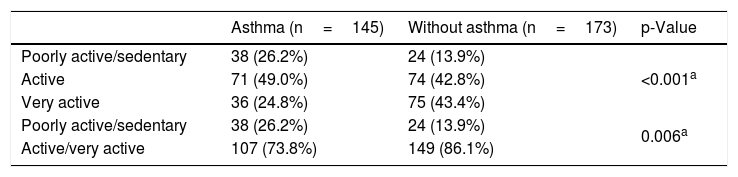
From the IPAQ classification, the prevalence of poorly active and sedentary individuals was 26.2% (38/145) in the AG and 13.9% (24/173) in the WAG (p<0.001; Table 3). When classified into only two groups, poorly active/sedentary and very active/active, it was found that the chance of being poorly active/sedentary in the AG was 2.2 times higher than in the WAG (OR=2.20, 95% CI: 1.25–3.89).
Classification of individuals by the International Physical Activity Questionnaire (IPAQ) questionnaire.
| Asthma (n=145) | Without asthma (n=173) | p-Value | |
|---|---|---|---|
| Poorly active/sedentary | 38 (26.2%) | 24 (13.9%) | <0.001a |
| Active | 71 (49.0%) | 74 (42.8%) | |
| Very active | 36 (24.8%) | 75 (43.4%) | |
| Poorly active/sedentary | 38 (26.2%) | 24 (13.9%) | 0.006a |
| Active/very active | 107 (73.8%) | 149 (86.1%) |
Data presented as absolute and relative frequencies.
Odds ratio=2.20, 95% CI: 1.25–3.89.
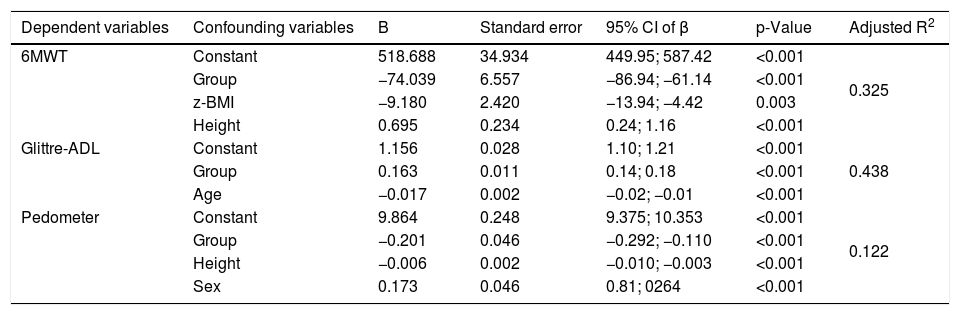
From the models of multiple linear regression analysis, it can be seen that in the case of the 6MWT, if the height and z-BMI are kept constant, the distance walked by the AG is on average 74.039m shorter than that of the WAG (6MWT distance=518.688–74.039*group–9.18*z-BMI+0.695*height). For the Glittre-ADL test, keeping age constant, AG participants had an average time 17.7% higher than that observed in the WAG (LN-Glittre-ADL=1.156+0.163*group–0.017*age). In the case of the pedometer, if the height and sex are kept constant, the average number of steps in the AG was 22.2% lower than that of the WAG (LN-pedometer=9.864−0.201*group–0.006*height+0.173*sex). Table 4 shows the dependent and confounding variables, the 95% CI of β, and the model determination coefficient.
Final multivariable linear regression models.
| Dependent variables | Confounding variables | B | Standard error | 95% CI of β | p-Value | Adjusted R2 |
|---|---|---|---|---|---|---|
| 6MWT | Constant | 518.688 | 34.934 | 449.95; 587.42 | <0.001 | 0.325 |
| Group | −74.039 | 6.557 | −86.94; −61.14 | <0.001 | ||
| z-BMI | −9.180 | 2.420 | −13.94; −4.42 | 0.003 | ||
| Height | 0.695 | 0.234 | 0.24; 1.16 | <0.001 | ||
| Glittre-ADL | Constant | 1.156 | 0.028 | 1.10; 1.21 | <0.001 | 0.438 |
| Group | 0.163 | 0.011 | 0.14; 0.18 | <0.001 | ||
| Age | −0.017 | 0.002 | −0.02; −0.01 | <0.001 | ||
| Pedometer | Constant | 9.864 | 0.248 | 9.375; 10.353 | <0.001 | 0.122 |
| Group | −0.201 | 0.046 | −0.292; −0.110 | <0.001 | ||
| Height | −0.006 | 0.002 | −0.010; −0.003 | <0.001 | ||
| Sex | 0.173 | 0.046 | 0.81; 0264 | <0.001 |
Group (1-asthma and 0-without asthma); sex (1-male and 0-female).
Age, years; CI, confidence interval; height, centimeters; adjusted R2, adjusted determination coefficient; 6MWT, six-minute walk test; Glittre-ADL, Glittre Activities of Daily Living test.
In this study, all tests carried out (6MWT, Glittre-ADL, pedometer, and IPAQ questionnaire) showed a difference between the groups, with the WAG presenting better performance and classification regarding the AG.
This was the first study using a set of tools to evaluate the level of physical activity and the functional capacity in children and adolescents with and without asthma in current research literature. The choice of subjective instruments such as the questionnaire, objective instruments such as daily step count, and two physical tests were important for greater classification accuracy, since all instruments present advantages and disadvantages when used alone.19
Individuals with asthma may be less active than individuals without asthma because of various factors, such as airway obstruction, increase in the sensation of dyspnea, and severity of symptom manifestation.20 In addition, family factors also contribute to inactivity, since parents/guardians usually have restrictive attitudes concerning exercise, judging it dangerous for fear of inducing an asthma exacerbation, or even due to lack of proper information on the disease.20
Concerning the 6MWT, the present findings were similar to those of Andrade et al.,21 who found that children and adolescents with moderate and severe asthma walked shorter distances compared to values predicted for healthy individuals in the same age group, and concluded that these values were directly influenced by physical inactivity in this population.
The Glittre-ADL test also pointed out the difference between the AG and the WAG in the present study. There are still no studies that compare the performance of children and adolescents with and without asthma on this test. The study by Corrêa et al.22 used the Glittre-ADL test to compare the functional capacity of healthy adults and adults with chronic obstructive pulmonary disease, and found that these individuals presented a worse physical performance when compared to healthy adults.
Evaluating the disease control level was important because information about how asthma symptoms affect daily physical activity are still scarce. In the present study, in both the 6MWT and Glittre-ADL, the groups with controlled, partially controlled, and uncontrolled asthma presented the same physical performance. As previously described, several factors may influence the reduction of physical and functional capacity of individuals with asthma, such as aspects related to the severity and manifestation of symptoms and family restrictive attitudes.
As for the pedometer, individuals from the WAG showed higher mean step count than individuals from the AG, as shown in the study by Vangeepuram et al.23 The authors justified this finding by the fact that their parents, especially those who are less educated, had a worse understanding of the disease, causing them to limit the physical activity of these children due to fear of exacerbations.
According to the recommendations of the World Health Organization (WHO),24 low levels of physical activity in children and adolescents are related to greater health risks. The mean daily step count in the present study was a worrying finding, in both the WAG and the AG, considering the values recommended by Tudor-Locke et al.18 for both male and female sexes over 6 years of age. However, according to Oliveira et al.,25 physical activity recommendations for Brazilian children based on step count have not yet been published.
Matsunaga et al.26 assessed the physical activity level of 100 children and adolescents with asthma through the long version of the IPAQ. After application of the questionnaire, 29.0% of the patients were classified as poorly active and sedentary, values close to those found in the present study for the AG (26.2%). However, individuals without asthma were not evaluated to compare the level of physical activity between the groups.
According to the current results, the importance of ensuring adequate preventive care for children and adolescents with asthma can be seen. In agreement with GINA, physical activity is one of the strategies that may be considered to assist in improving symptom control and/or reducing future risk. In this context, documents like the guidance manuals “Promotion of Physical Activity in Children and Adolescents”27 and “Recommendations for the Management of Asthma of the Brazilian Society of Pulmonology and Tisiology”28 represent an important strategy for the dissemination of guidelines on the theme for both health professionals and the general population.
Although this study has as a limitation the number of uncontrolled patients, it was observed that even patients with controlled asthma had worse performance in relation to physical activity and functional capacity when compared to healthy individuals.
In conclusion, all tests performed were able to differentiate the physical activity level and functional capacity among participants of the different groups, indicating that children and adolescents with asthma displayed worse physical performance when compared to individuals without asthma. In addition, individuals with uncontrolled, partially controlled, and controlled asthma presented similar performance in functional capacity tests.
FundingThis work received funding from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior — Brasil (CAPES) [Finance Code 174296] and Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) — Brasil [Process No. 2016/22102-8].
Conflicts of interestThe authors declare no conflicts of interest.
Study conducted at Universidade Estadual de Campinas (Unicamp), Faculdade de Ciências Médicas, Campinas, SP, Brazil.





