
The clinical picture of children with autism spectrum disorder is characterized by deficits of social interaction and communication, as well as by repetitive interests and activities. Sensory abnormalities are a very frequent feature that often go unnoticed due to the communication difficulties of these patients. This narrative review summarizes the main features of sensory abnormalities and the respective implications for the interpretation of several signs and symptoms of autism spectrum disorder, and therefore for its management.
SourcesA search was performed in PubMed (United States National Library of Medicine) about the sensory abnormalities in subjects (particularly children) with autism spectrum disorder.
Summary of the findingsSensory symptoms are common and often disabling in children with autism spectrum disorder, but are not specific for autism, being a feature frequently described also in subjects with intellectual disability. Three main sensory patterns have been described in autism spectrum disorder: hypo-responsiveness, hyper-responsiveness, and sensory seeking; to these, some authors have added a fourth pattern: enhanced perception. Sensory abnormalities may negatively impact the life of these individuals and their families. An impairment not only of unisensory modalities but also of multisensory integration is hypothesized.
ConclusionsAtypical sensory reactivity of subjects with autism spectrum disorder may be the key to understand many of their abnormal behaviors, and thus it is a relevant aspect to be taken into account in their daily management in all the contexts in which they live. A formal evaluation of sensory function should be always performed in these children.
O quadro clínico de crianças com transtorno do espectro do autismo é caracterizado por déficits de interação social e comunicação, bem como por interesses e atividades repetitivos. As alterações sensoriais são uma característica muito frequente que geralmente não é percebida devido às dificuldades de comunicação desses pacientes. Nesta análise narrativa, resumimos as principais características de alterações sensoriais e as respectivas implicações para a interpretação de vários sinais e sintomas do transtorno do espectro do autismo e, portanto, para seu manejo.
FontesRealizamos uma busca no PubMed (Biblioteca Nacional de Medicina dos Estados Unidos) sobre as alterações sensoriais em indivíduos (principalmente crianças) com transtorno do espectro do autismo.
Resumo dos achadosAs alterações sensoriais são comuns e geralmente invalidam as crianças com transtorno do espectro do autismo, porém não são específicas do autismo, sendo uma característica frequentemente descrita também em indivíduos com deficiência intelectual. Três principais padrões sensoriais foram descritos no transtorno do espectro do autismo: hiporreatividade, hiperreatividade e busca sensorial; a eles, alguns autores acrescentaram um quarto padrão: percepção aprimorada. As alterações sensoriais podem afetar negativamente a vida desses indivíduos e de suas famílias. Hipotetizamos uma deficiência não apenas das modalidades não sensoriais, mas também da integração multissensorial.
ConclusõesA reatividade sensorial atípica de indivíduos com transtorno do espectro do autismo pode ser a chave para entender muitos de seus comportamentos anormais e, portanto, é um aspecto relevante para ser considerado em seu manejo diário em todos os contextos nos quais eles vivem. Sempre se deve fazer uma avaliação formal da função sensorial nessas crianças.
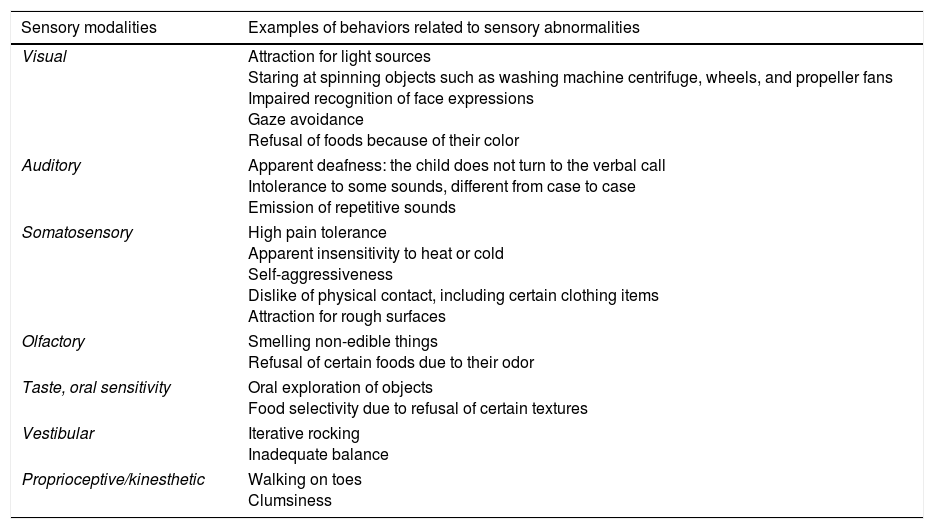
The clinical picture of children with autism spectrum disorder (ASD) is characterized by deficits of social interaction and communication, as well as by repetitive interests and activities, according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).1 Sensory abnormalities are a very frequent feature that often go unnoticed due to the communication difficulties of these patients. According to the DSM-5 criteria, this type of symptomatology is constituted by increased or decreased reactivity to sensory input, or by an unusual interest in sensory aspects of the environment. The following are some of the examples cited by the DSM-5: visual fascination with lights or spinning objects; adverse response to specific sounds or textures; excessive smelling or touching of objects; apparent indifference to pain, heat, or cold.1 Almost any sensory channel may be involved, either in the sense of reduced responsiveness to stimulation or in the sense of excessive responsiveness to stimulation. There may be several types of sensory abnormalities in the same person over the course of life, or even at the same time. Table 1 describes several possible examples of behaviors related to sensory abnormalities in children with ASD. Sensory dysfunction is probably related to an impaired modulation occurring in the central nervous system, which regulates neural messages concerning sensory stimuli.2 Already in Sukhareva's pioneering description of children with autism (1926), sensory reactivity disorders were unequivocally mentioned with foresight.3 Later, hypo-reactivity as well as hyper-reactivity to sensory stimuli were reported in the classical descriptions of Kanner in 19434 and Asperger in 1944.5 In the following decades, the attention to these features has fluctuated, although the clinical experience with ASD individuals has always suggested the importance of these aspects. In 1980, the DSM-III considered sensory hypo-responsiveness or hyper-responsiveness as infantile autism-associated features,6 while the following two editions, DSM-III-R7 and DSM-IV,8 did not include sensory abnormalities as definite diagnostic criteria. Finally, the DSM-5 (2013) included “hyper- or hypo-reactivity to sensory input” as well as “unusual interests in sensory aspects of environment” within the main ASD criterion concerning restricted interests and repetitive behaviors.1
Examples of behaviors related to sensory abnormalities reported in children with autism spectrum disorder, grouped according to the sensory modalities.
| Sensory modalities | Examples of behaviors related to sensory abnormalities |
|---|---|
| Visual | Attraction for light sources Staring at spinning objects such as washing machine centrifuge, wheels, and propeller fans Impaired recognition of face expressions Gaze avoidance Refusal of foods because of their color |
| Auditory | Apparent deafness: the child does not turn to the verbal call Intolerance to some sounds, different from case to case Emission of repetitive sounds |
| Somatosensory | High pain tolerance Apparent insensitivity to heat or cold Self-aggressiveness Dislike of physical contact, including certain clothing items Attraction for rough surfaces |
| Olfactory | Smelling non-edible things Refusal of certain foods due to their odor |
| Taste, oral sensitivity | Oral exploration of objects Food selectivity due to refusal of certain textures |
| Vestibular | Iterative rocking Inadequate balance |
| Proprioceptive/kinesthetic | Walking on toes Clumsiness |
Sensory abnormalities of ASD children may also impair their behavior in family daily activities, including eating, sleeping, and bathtime and bedtime routines; and outside the home, these abnormalities may create problems, for example when taking vacations or participating in community events. Consequently, interventions for autism should include also specific strategies for managing sensory-related behaviors in order to improve daily family activities and participation in community events.9
This narrative review summarizes the main features of abnormal sensory reactivity in ASD patients and their implications for the interpretation of various signs and symptoms of autism, and thus for treatment. The authors considered the most relevant papers (preferably concerning children) among those published on this topic over the period from January 1, 2007 to July 31, 2017 available on PubMed (United States National Library of Medicine), including reviews; the following keywords were used: “autism,” “sensory reactivity,” “sensory abnormalities.”
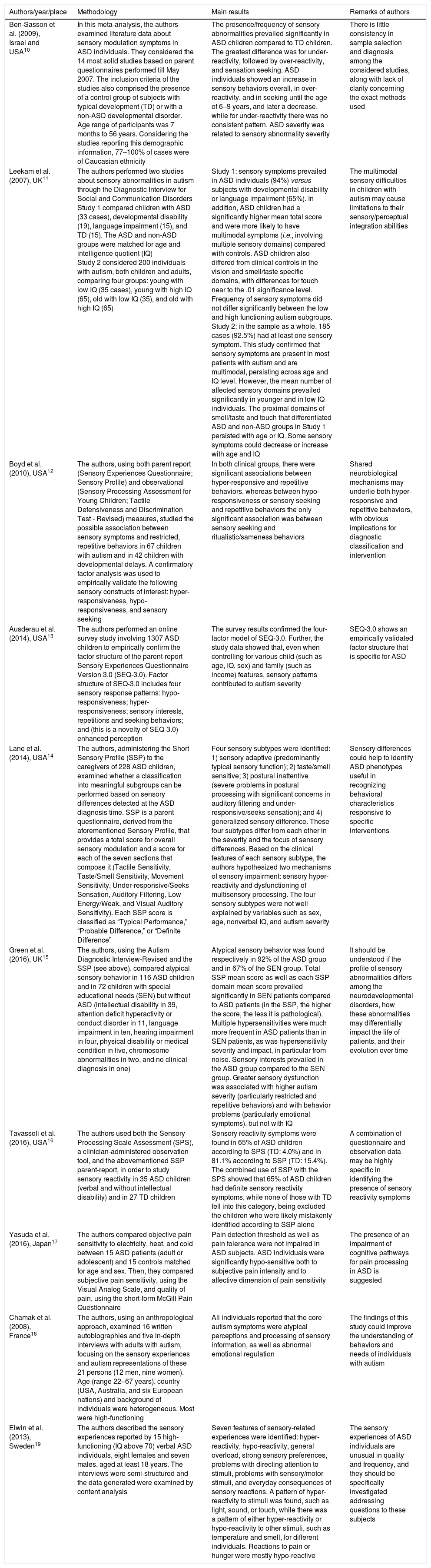
Sensory abnormalities and ASDTable 2 summarizes the most important results of this review.10–19 Three main sensory patterns have been described in patients with ASD: hypo-responsiveness, hyper-responsiveness, and sensory seeking; to these, some authors have added a fourth pattern: enhanced perception.13 Among the findings emerging from Table 2, there is also the importance of associating an objective with a subjective evaluation, as confirmed by the case of pain sensitivity, classically considered reduced in ASD subjects. In this regard, the study by Yasuda et al. offers very interesting findings (Table 2).17
Characteristics of studies that evaluated sensory abnormalities in patients with autism spectrum disorder (ASD).
| Authors/year/place | Methodology | Main results | Remarks of authors |
|---|---|---|---|
| Ben-Sasson et al. (2009), Israel and USA10 | In this meta-analysis, the authors examined literature data about sensory modulation symptoms in ASD individuals. They considered the 14 most solid studies based on parent questionnaires performed till May 2007. The inclusion criteria of the studies also comprised the presence of a control group of subjects with typical development (TD) or with a non-ASD developmental disorder. Age range of participants was 7 months to 56 years. Considering the studies reporting this demographic information, 77–100% of cases were of Caucasian ethnicity | The presence/frequency of sensory abnormalities prevailed significantly in ASD children compared to TD children. The greatest difference was for under-reactivity, followed by over-reactivity, and sensation seeking. ASD individuals showed an increase in sensory behaviors overall, in over-reactivity, and in seeking until the age of 6–9 years, and later a decrease, while for under-reactivity there was no consistent pattern. ASD severity was related to sensory abnormality severity | There is little consistency in sample selection and diagnosis among the considered studies, along with lack of clarity concerning the exact methods used |
| Leekam et al. (2007), UK11 | The authors performed two studies about sensory abnormalities in autism through the Diagnostic Interview for Social and Communication Disorders Study 1 compared children with ASD (33 cases), developmental disability (19), language impairment (15), and TD (15). The ASD and non-ASD groups were matched for age and intelligence quotient (IQ) Study 2 considered 200 individuals with autism, both children and adults, comparing four groups: young with low IQ (35 cases), young with high IQ (65), old with low IQ (35), and old with high IQ (65) | Study 1: sensory symptoms prevailed in ASD individuals (94%) versus subjects with developmental disability or language impairment (65%). In addition, ASD children had a significantly higher mean total score and were more likely to have multimodal symptoms (i.e., involving multiple sensory domains) compared with controls. ASD children also differed from clinical controls in the vision and smell/taste specific domains, with differences for touch near to the .01 significance level. Frequency of sensory symptoms did not differ significantly between the low and high functioning autism subgroups. Study 2: in the sample as a whole, 185 cases (92.5%) had at least one sensory symptom. This study confirmed that sensory symptoms are present in most patients with autism and are multimodal, persisting across age and IQ level. However, the mean number of affected sensory domains prevailed significantly in younger and in low IQ individuals. The proximal domains of smell/taste and touch that differentiated ASD and non-ASD groups in Study 1 persisted with age or IQ. Some sensory symptoms could decrease or increase with age and IQ | The multimodal sensory difficulties in children with autism may cause limitations to their sensory/perceptual integration abilities |
| Boyd et al. (2010), USA12 | The authors, using both parent report (Sensory Experiences Questionnaire; Sensory Profile) and observational (Sensory Processing Assessment for Young Children; Tactile Defensiveness and Discrimination Test - Revised) measures, studied the possible association between sensory symptoms and restricted, repetitive behaviors in 67 children with autism and in 42 children with developmental delays. A confirmatory factor analysis was used to empirically validate the following sensory constructs of interest: hyper-responsiveness, hypo-responsiveness, and sensory seeking | In both clinical groups, there were significant associations between hyper-responsive and repetitive behaviors, whereas between hypo-responsiveness or sensory seeking and repetitive behaviors the only significant association was between sensory seeking and ritualistic/sameness behaviors | Shared neurobiological mechanisms may underlie both hyper-responsive and repetitive behaviors, with obvious implications for diagnostic classification and intervention |
| Ausderau et al. (2014), USA13 | The authors performed an online survey study involving 1307 ASD children to empirically confirm the factor structure of the parent-report Sensory Experiences Questionnaire Version 3.0 (SEQ-3.0). Factor structure of SEQ-3.0 includes four sensory response patterns: hypo-responsiveness; hyper-responsiveness; sensory interests, repetitions and seeking behaviors; and (this is a novelty of SEQ-3.0) enhanced perception | The survey results confirmed the four-factor model of SEQ-3.0. Further, the study data showed that, even when controlling for various child (such as age, IQ, sex) and family (such as income) features, sensory patterns contributed to autism severity | SEQ-3.0 shows an empirically validated factor structure that is specific for ASD |
| Lane et al. (2014), USA14 | The authors, administering the Short Sensory Profile (SSP) to the caregivers of 228 ASD children, examined whether a classification into meaningful subgroups can be performed based on sensory differences detected at the ASD diagnosis time. SSP is a parent questionnaire, derived from the aforementioned Sensory Profile, that provides a total score for overall sensory modulation and a score for each of the seven sections that compose it (Tactile Sensitivity, Taste/Smell Sensitivity, Movement Sensitivity, Under-responsive/Seeks Sensation, Auditory Filtering, Low Energy/Weak, and Visual Auditory Sensitivity). Each SSP score is classified as “Typical Performance,” “Probable Difference,” or “Definite Difference” | Four sensory subtypes were identified: 1) sensory adaptive (predominantly typical sensory function); 2) taste/smell sensitive; 3) postural inattentive (severe problems in postural processing with significant concerns in auditory filtering and under-responsive/seeks sensation); and 4) generalized sensory difference. These four subtypes differ from each other in the severity and the focus of sensory differences. Based on the clinical features of each sensory subtype, the authors hypothesized two mechanisms of sensory impairment: sensory hyper-reactivity and dysfunctioning of multisensory processing. The four sensory subtypes were not well explained by variables such as sex, age, nonverbal IQ, and autism severity | Sensory differences could help to identify ASD phenotypes useful in recognizing behavioral characteristics responsive to specific interventions |
| Green et al. (2016), UK15 | The authors, using the Autism Diagnostic Interview-Revised and the SSP (see above), compared atypical sensory behavior in 116 ASD children and in 72 children with special educational needs (SEN) but without ASD (intellectual disability in 39, attention deficit hyperactivity or conduct disorder in 11, language impairment in ten, hearing impairment in four, physical disability or medical condition in five, chromosome abnormalities in two, and no clinical diagnosis in one) | Atypical sensory behavior was found respectively in 92% of the ASD group and in 67% of the SEN group. Total SSP mean score as well as each SSP domain mean score prevailed significantly in SEN patients compared to ASD patients (in the SSP, the higher the score, the less it is pathological). Multiple hypersensitivities were much more frequent in ASD patients than in SEN patients, as was hypersensitivity severity and impact, in particular from noise. Sensory interests prevailed in the ASD group compared to the SEN group. Greater sensory dysfunction was associated with higher autism severity (particularly restricted and repetitive behaviors) and with behavior problems (particularly emotional symptoms), but not with IQ | It should be understood if the profile of sensory abnormalities differs among the neurodevelopmental disorders, how these abnormalities may differentially impact the life of patients, and their evolution over time |
| Tavassoli et al. (2016), USA16 | The authors used both the Sensory Processing Scale Assessment (SPS), a clinician-administered observation tool, and the abovementioned SSP parent-report, in order to study sensory reactivity in 35 ASD children (verbal and without intellectual disability) and in 27 TD children | Sensory reactivity symptoms were found in 65% of ASD children according to SPS (TD: 4.0%) and in 81.1% according to SSP (TD: 15.4%). The combined use of SSP with the SPS showed that 65% of ASD children had definite sensory reactivity symptoms, while none of those with TD fell into this category, being excluded the children who were likely mistakenly identified according to SSP alone | A combination of questionnaire and observation data may be highly specific in identifying the presence of sensory reactivity symptoms |
| Yasuda et al. (2016), Japan17 | The authors compared objective pain sensitivity to electricity, heat, and cold between 15 ASD patients (adult or adolescent) and 15 controls matched for age and sex. Then, they compared subjective pain sensitivity, using the Visual Analog Scale, and quality of pain, using the short-form McGill Pain Questionnaire | Pain detection threshold as well as pain tolerance were not impaired in ASD subjects. ASD individuals were significantly hypo-sensitive both to subjective pain intensity and to affective dimension of pain sensitivity | The presence of an impairment of cognitive pathways for pain processing in ASD is suggested |
| Chamak et al. (2008), France18 | The authors, using an anthropological approach, examined 16 written autobiographies and five in-depth interviews with adults with autism, focusing on the sensory experiences and autism representations of these 21 persons (12 men, nine women). Age (range 22–67 years), country (USA, Australia, and six European nations) and background of individuals were heterogeneous. Most were high-functioning | All individuals reported that the core autism symptoms were atypical perceptions and processing of sensory information, as well as abnormal emotional regulation | The findings of this study could improve the understanding of behaviors and needs of individuals with autism |
| Elwin et al. (2013), Sweden19 | The authors described the sensory experiences reported by 15 high-functioning (IQ above 70) verbal ASD individuals, eight females and seven males, aged at least 18 years. The interviews were semi-structured and the data generated were examined by content analysis | Seven features of sensory-related experiences were identified: hyper-reactivity, hypo-reactivity, general overload, strong sensory preferences, problems with directing attention to stimuli, problems with sensory/motor stimuli, and everyday consequences of sensory reactions. A pattern of hyper-reactivity to stimuli was found, such as light, sound, or touch, while there was a pattern of either hyper-reactivity or hypo-reactivity to other stimuli, such as temperature and smell, for different individuals. Reactions to pain or hunger were mostly hypo-reactive | The sensory experiences of ASD individuals are unusual in quality and frequency, and they should be specifically investigated addressing questions to these subjects |
As shown in Table 2, over the last years several parent report questionnaires concerning sensory reactivity have been used in ASD individuals, some not specific for autism (e.g., Short Sensory Profile – SSP), others specific for autism (e.g., Sensory Experiences Questionnaire, Version 3.0 – SEQ-3.0). These questionnaires (only sporadically associated with observational tools)12,16,20 can provide valuable findings; however, as they are based on data from an external perspective, they cannot describe the first-person sensorial experience of patients. It would be very important to understand what they really perceive, but unfortunately only some are able to describe it, due to the frequently severe impairment of language and cognitive skills. ASD patients who are able to describe the sensory experiences can provide us with information that is also at least partially applicable to individuals who cannot report such experiences. This aspect was addressed in the studies by Chamak et al.18 and Elwin et al.19 (Table 2).
There are different ways by which sensory abnormalities may negatively impact the life of ASD individuals and their families,9–16,18–20 including an impairment of: social communication and activities; adaptive behavior (e.g., “problem behaviors”: see Discussion); range of interests (restricted, repetitive); everyday routines (e.g., avoiding behaviors due to sensorial distress); and cognition, the last one hypothetically due to the reduced number of signals that ASD individuals can utilize to understand and interact with the environment, as recently suggested by Haigh.21 In addition, eating behavior can be affected by sensory abnormalities, leading to a food selectivity that can in turn cause inadequate nutrition22, as well as sleep, due particularly to a hyperarousal mechanism.23
Sensory abnormalities in ASD: interpretative hypothesesSeveral hypotheses have been formulated to explain the sensory abnormalities in ASD patients, including that of “enhanced perceptual functioning,” perhaps due to the increased functioning of the brain regions involved in primary perceptual functions,24 and the “intense world hypothesis of autism,” where the core brain pathology is increased reactivity and plasticity of local neuronal circuits, leading to increased perception, attention, and memory, making the world aversively intense for the child with ASD.25 But during recent years, there has been an increasing interest in the interpretation models suggesting an impairment not only of unisensory modalities (e.g., auditory alone) but also of multisensory integration, probably related to a brain connectivity impairment, consisting in particular of poor long range connectivity.26 According to this perspective, children and other individuals with ASD have a reduced ability to integrate sensory information across different modalities (auditory, visual, etc.), which would contribute to core autism symptoms, such as social communication impairments.11,14,27,28 In addition, environmental factors may influence these symptoms, as recently suggested by Kirby et al., who studied the contexts surrounding the sensory and repetitive behaviors of 32 ASD children through the behavioral coding of naturalistic video recordings at home. They found that hyper-responsive behaviors were associated with daily living activities and stimuli initiated by the family, while sensory seeking behaviors were associated with free play activities and stimuli initiated by the child. However, the conclusions of this intriguing study should be taken with caution due to the relatively narrow size of the sample considered.29
Sensory abnormalities in ASD: interventionsIn the context of sensory interventions, sensory integration therapies (child-centered) and sensory-based interventions (adult-directed) are distinguished. The former are clinic-based interventions using play activities and sensory-enhanced interactions in order to improve the adaptive responses to sensory experiences. Through gross motor activities activating the vestibular and somatosensory systems, these interventions aim to enhance the capacity to integrate sensory information, leading the child to adopt more organized and adaptive behaviors, including improved joint attention, social skills, motor planning, and perceptual skills. In this context, the therapist chooses a “just-right challenge” (i.e., an activity that is just a little above what the child is now able to do without difficulty) from the child's emerging skills and supports his/her adaptive responses to the challenge. Conversely, sensory-based interventions are classroom-based and use single-sensory strategies (for example therapy balls or weighted vests) in order to influence the state of arousal, most often, with the aim of reducing a high arousal state that can be clinically manifested as restlessness, hyperactivity, and self-stimulating behaviors.30
Which of these two types of intervention is the most effective? The answer comes from Case-Smith et al.,30 who performed a systematic review concerning sensory interventions in children with ASD and sensory processing abnormalities (2000–2012), including five studies about the effects of sensory integration therapies and 14 studies about the effects of sensory-based interventions. Concerning sensory integration therapies, two randomized controlled trials showed positive effects on Goal Attainment Scaling,31,32 decreased mannerisms,31 and improved self-care and social function,32 while other studies showed positive effects on decreasing behaviors related to sensory abnormalities. On the contrary, the studies about sensory-based interventions showed only a few positive effects, suggesting a lack of efficacy.30
DiscussionSensory experiences in ASD individuals are reported as a distress/anxiety as well as a source of fascination/interest.33 On one hand, distress/anxiety can lead to avoidance behaviors against disturbing stimuli or may even trigger reactions with intense agitation and hetero- or self-directed aggression (see the so-called “problem behaviors”). On the other hand, the absorbent stimuli sources can lead to restricted and repetitive behaviors, from which it is very hard to deflect these individuals’ attention. For one reason or another, the impact of sensory abnormalities of children with ASD on their daily lives is considerable and probably underestimated because of their communication difficulties, thus it should always be specifically investigated.
The following question arises spontaneously: should sensory abnormalities be considered core autism features or only comorbidity characteristics? Based on the data available today, this question remains open. In fact, sensory symptoms are common and often invalidating in ASD children, but are not specific for autism, being a feature, as was mentioned above, frequently described also in subjects with intellectual disability without autism. However, the atypical sensory reactivity of these subjects may be the key to understand many of their abnormal behaviors and, therefore, it is a relevant aspect to be taken into account in the daily management of these individuals in all contexts in which they live. For example, according to Leekam et al., the distress due to specific sensory inputs can arouse problem behaviors in low-functioning ASD individuals who are unable to report their discomfort. Understanding what specific sensory inputs cause discomfort in a given individual is the prerequisite for reorganizing the environment in which he/she lives and his/her daily routine in order to reduce as much as possible such discomfort; in this perspective, a desensitization program may be useful. In some cases the use of sensory rooms, where individuals have pleasant sensory experiences of various kinds, can be very useful.11
In conclusion, a formal evaluation of sensory function should be always performed within the neurobehavioral assessment of ASD children and should be repeated periodically during the follow-up, in order to meet the needs of these individuals, to prevent as far as possible the appearance of problem behaviors, and ultimately to alleviate the difficulties of their families. Moreover, further research should be performed, according to Lane et al.,14 in order to better understand the possible neurobiological (genetic, neurophysiological, and neuro-imaging) pathways of sensory abnormalities in ASD patients.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Cecilia Baroncini for linguistic support.
Please cite this article as: Posar A, Visconti P. Sensory abnormalities in children with autism spectrum disorder. J Pediatr (Rio J). 2018;94:342–50.





