
Computed tomography should be performed after careful consideration due to radiation hazard, which is why interest in low dose CT has increased recently in acute appendicitis. Previous studies have been performed in adult and adolescents populations, but no studies have reported on the efficacy of using low-dose CT in children younger than 10 years.
MethodsPatients (n=475) younger than 10 years who were examined for acute appendicitis were recruited. Subjects were divided into three groups according to the examinations performed: low-dose CT, ultrasonography, and standard-dose CT. Subjects were categorized according to age and body mass index (BMI).
ResultsLow-dose CT was a contributive tool in diagnosing appendicitis, and it was an adequate method, when compared with ultrasonography and standard-dose CT in terms of sensitivity (95.5% vs. 95.0% and 94.5%, p=0.794), specificity (94.9% vs. 80.0% and 98.8%, p=0.024), positive-predictive value (96.4% vs. 92.7% and 97.2%, p=0.019), and negative-predictive value (93.7% vs. 85.7% and 91.3%, p=0.890). Low-dose CT accurately diagnosed patients with a perforated appendix. Acute appendicitis was effectively diagnosed using low-dose CT in both early and middle childhood. BMI did not influence the accuracy of detecting acute appendicitis on low-dose CT.
ConclusionLow-dose CT is effective and accurate for diagnosing acute appendicitis in childhood, as well as in adolescents and young adults. Additionally, low-dose CT was relatively accurate, irrespective of age or BMI, for detecting acute appendicitis. Therefore, low-dose CT is recommended for assessing children with suspected acute appendicitis.
A tomografia computadorizada deve ser realizada após cautelosa consideração devido ao perigo de radiação, motivo pelo qual o interesse na TC de baixa dosagem tem aumentado recentemente em casos de apendicite aguda. Estudos anteriores foram realizados em populações adultas ou adolescentes, porém nenhum estudo relatou a eficácia do uso da TC de baixa dosagem em crianças com menos de 10 anos de idade.
MétodosRecrutamos pacientes (n=475) com menos de 10 anos de idade examinados com relação a apendicite aguda. Os indivíduos foram divididos em três grupos de acordo com os exames realizados: TC de baixa dosagem, ultrassonografia e TC de dosagem padrão. Os indivíduos foram categorizados de acordo com a idade e o índice de massa corporal.
ResultadosA TC de baixa dosagem foi uma ferramenta de grande contribuição no diagnóstico de apendicite e um método adequado em comparação à ultrassonografia e à TC de dosagem padrão em termos de sensibilidade (95,5% em comparação a 95,0% e 94,5%, p=0,794), especificidade (94,9% em comparação a 80,0% e 98,8%, p=0,024), valor preditivo positivo (96,4% em comparação a 92,7% e 97,2%, p=0,019) e valor preditivo negativo (93,7% em comparação a 85,7% e 91,3%, p=0,890). A TC de baixa dosagem diagnosticou de forma precisa pacientes com um apêndice perfurado. A apendicite aguda foi diagnosticada de maneira efetiva utilizando a TC de baixa dosagem tanto na primeira quanto na segunda infância. O IMC não influenciou a precisão da detecção de apendicite aguda na TC de baixa dosagem.
ConclusãoA TC de baixa dosagem é eficaz e precisa no diagnóstico de apendicite aguda na infância, bem como em adolescentes e jovens adultos. Além disso, a TC de baixa dosagem foi relativamente precisa, independentemente de idade ou IMC, na detecção de apendicite aguda. Assim, a TC de baixa dosagem é recomendada na avaliação de crianças com suspeita de apendicite aguda.
Acute appendicitis is the most common abdominal disease requiring surgery in the pediatric population. The incidence of appendicitis is relatively high in pediatric patients, and appendicitis in these patients tends to be associated with higher rates of perforation.1–3 To prevent severe complications, such as perforation, panperitonitis, or intra-abdominal abscess, early diagnosis and prompt treatment, such as appendectomy, are important. In the past, the rate of negative or unnecessary appendectomies was higher. With recent advances in imaging techniques, such as ultrasonography (USG) or computed tomography (CT), the diagnostic accuracy of acute appendicitis has improved, and negative appendectomy rates have been reduced.4
Among these diagnostic modalities, USG has been considered a tool to aid in the diagnosis of acute appendicitis over the last 30 years, and has been particularly useful for diagnosing appendicitis in children, because it uses no ionizing radiation and is non-invasive.4 However, its diagnostic accuracy varies, depending on the operator; moreover, making a diagnosis based on USG findings is difficult in obese patients.4,5 Conversely, CT has a high sensitivity and specificity; thus, it is a comparatively accurate diagnostic method, and consequently, the number of CT examinations has increased considerably.4–6 Nevertheless, CT must be performed carefully, because of the associated radiation exposure, and the consequent risk of cancer.6–8 Saito et al. reported various methods that are currently used to diagnose pediatric appendicitis at different hospitals, but no clear conclusion could be drawn regarding the effect of age or body mass index (BMI).6 With magnetic resonance imaging (MRI), there is no exposure to ionizing. The scanner is safe during pregnancy and the result of the examination is reliable and accurate. Nevertheless, MRI is not used widely due to its high costs.4
For these reasons, there is an increasing interest in low-dose CT. Some studies on this subject have been reported, which have focused on diverse diseases, including cardiac or pulmonary diseases, in addition to abdominal diseases, and in various age groups.9,10 Additionally, many reports have evaluated diagnoses made using low-dose CT in adults and adolescents, and these findings have been applied in clinical practice.11–15 However, no studies have reported the efficacy of using dose CT in the diagnosis of acute appendicitis in children younger than 10 years, including those in early childhood, as previous studies have focused mainly on young adults or adolescents.
Therefore, in the present study, the authors assessed the usefulness and accuracy of low-dose CT for diagnosing acute appendicitis in children, and compared the use of low-dose CT in this context with abdominal USG and standard-dose abdominal CT.
MethodsPatients and data extractionChildren under 10 years of age who were hospitalized at Chung-Ang University Hospital from March 2005 to December 2014 with clinical suspicion of acute appendicitis were recruited for the study.16 Among those recruited, patients who did not undergo radiological evaluation and those in which the purpose of radiological evaluation was unclear were excluded; thus, 616 patients were identified. Of these, further patients were excluded due to prior appendectomy. The exclusion criteria also comprised patients with a gastrointestinal anomaly that caused structural misperception during radiological interpretation; patients diagnosed by CT imaging, but for whom the accurate radiation dose was not recorded; and those with other gastrointestinal abnormalities, such as intussusceptions or malignancy. A total of 484 patients were assessed, and the clinical manifestations, laboratory findings, imaging findings, operation records, and pathological findings were retrospectively analyzed. Of these, nine children underwent CT after USG (standard-dose CT: five patients; low-dose CT: four patients) and were also excluded. In the remaining 475 patients, a single test was performed, and those patients were included in the study. The definite diagnosis of appendicitis was based on operation records, findings, and pathology records.
Subjects were categorized into two groups according to age classifications developed by the Eunice Kennedy Shriver National Institute of Child Health and Human Development: early childhood (2–5 years) and middle childhood (6–10 years).17
BMI was calculated from the patient's medical chart, and subjects were categorized into three groups according to age-specific BMI: underweight (<5th percentile), normal weight (5th–85th percentile), and overweight (>85th percentile).
This study was conducted after the approval from the Institutional Review Board (IRB) of the Chung-Ang University Hospital (IRB No. 10-014-02-03), and the need for an informed consent was waived due to the retrospective nature of the study.
Diagnostic imaging methodsFor all study subjects, low-dose and standard-dose CT and abdominal USG were performed and read by expert abdominal radiologists when they presented with acute symptoms. Other expert abdominal radiologists retrospectively reviewed the radiologic images.
At this institution, CT examinations for acute abdominal pain were performed using intravenous contrast media. No oral or rectal contrast material was used. The CT radiation dose was adjusted according to the child's age and weight.16 Exams were performed on either a Philips Brilliance iCT 256-slice or Brilliance 64-slice CT scanner (Philips Healthcare, Cleveland, OH, USA) with statistical iterative reconstruction algorithms (iDose).4 The CT protocol used was the size-based scan technique (weight-based, 80–120 kVp), with automated Z-axis dose modulation based on the scout image (DoseRight, Philips Healthcare, Cleveland, OH, USA). Images were reformatted at 3-mm slice thickness in the axial plane and 3-mm slice thickness in the coronal plane for clinical review.
The primary criteria for diagnosis of appendicitis by CT were visualization of an appendix >6mm in diameter, a non-opacified appendiceal lumen, and significant wall enhancement. Secondary criteria on CT included visualization of periappendiceal fat stranding, appendicolith, bowel wall thickening, free fluid, extraluminal air, and the presence of phlegmon or abscess, with the final four criteria constituting evidence of perforation.18–20 A scan was considered to be negative if a normal appendix was observed or if no secondary signs were seen, even if the appendix could not be visualized. The presence of any alternative diagnosis for patient pain was recorded, excluding mesenteric adenitis, as it is a diagnosis of exclusion.
Statistical analysisStatistical analysis was performed using SPSS 18.0 statistical software (SPSS Inc., IL, USA). ANOVA test, Student's t-test, Pearson's χ2 test, and analysis of variance were used to analyze differences between groups. The level of statistical significance was set at p<0.05.
ResultsOf the 484 children evaluated by radiological methods, nine underwent CT after USG in order to achieve an accurate diagnosis of appendicitis. The diagnosis was followed by appendectomy. In the remaining 475 patients included in the study, a single test was performed. Of these, 297 children were finally diagnosed with acute appendicitis (Table 1).
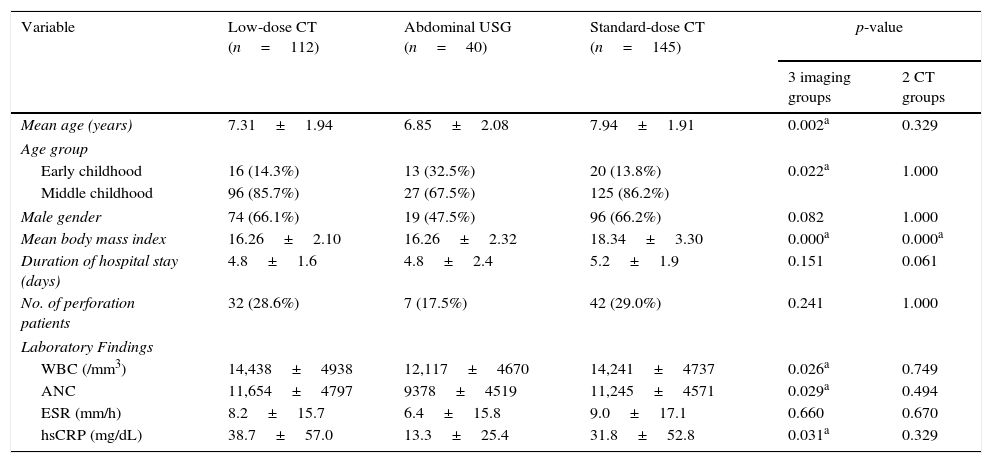
Clinical manifestations and laboratory findings according to radiologic methods in children with acute appendicitis.
| Variable | Low-dose CT (n=112) | Abdominal USG (n=40) | Standard-dose CT (n=145) | p-value | |
|---|---|---|---|---|---|
| 3 imaging groups | 2 CT groups | ||||
| Mean age (years) | 7.31±1.94 | 6.85±2.08 | 7.94±1.91 | 0.002a | 0.329 |
| Age group | |||||
| Early childhood | 16 (14.3%) | 13 (32.5%) | 20 (13.8%) | 0.022a | 1.000 |
| Middle childhood | 96 (85.7%) | 27 (67.5%) | 125 (86.2%) | ||
| Male gender | 74 (66.1%) | 19 (47.5%) | 96 (66.2%) | 0.082 | 1.000 |
| Mean body mass index | 16.26±2.10 | 16.26±2.32 | 18.34±3.30 | 0.000a | 0.000a |
| Duration of hospital stay (days) | 4.8±1.6 | 4.8±2.4 | 5.2±1.9 | 0.151 | 0.061 |
| No. of perforation patients | 32 (28.6%) | 7 (17.5%) | 42 (29.0%) | 0.241 | 1.000 |
| Laboratory Findings | |||||
| WBC (/mm3) | 14,438±4938 | 12,117±4670 | 14,241±4737 | 0.026a | 0.749 |
| ANC | 11,654±4797 | 9378±4519 | 11,245±4571 | 0.029a | 0.494 |
| ESR (mm/h) | 8.2±15.7 | 6.4±15.8 | 9.0±17.1 | 0.660 | 0.670 |
| hsCRP (mg/dL) | 38.7±57.0 | 13.3±25.4 | 31.8±52.8 | 0.031a | 0.329 |
CT, computed tomography; USG, ultrasonography; WBC, white blood cell; ANC, absolute neutrophil count; ESR, erythrocyte sedimentation rate; hsCRP, highly sensitive C-reactive protein.
The mean age and age group were slightly higher in patients who underwent standard-dose CT than in those who underwent low-dose CT or USG (p=0.002 vs. p=0.022). However, there were no significant differences in the two CT groups (p=0.329 vs. p=1.000). In addition, the mean BMI was slightly higher in the standard-dose CT group (p=0.000). In laboratory findings, there were significant differences in white blood cell count, absolute neutrophil count, and highly sensitive C-reactive protein levels between the three groups (p=0.026, p=0.029, and p=0.031, respectively). Moreover, these values were also not significantly different between the two CT groups (p=0.749, p=0.494, and p=0.329, respectively). Other clinical manifestations and laboratory findings are presented in Table 1.
Comparison of the radiation dose parameters between the CT groupsRegarding the two groups that underwent CT, in the low-dose CT group, as compared with the standard-dose CT group, the radiation dose was reduced by about 64.2% (2.06±0.52 vs. 5.76±3.23, p=0.000). However, there was no significant difference between the two groups regarding the tube voltage and tube current (93.58±15.36 vs. 95.91±17.20; 92.56±35.00 vs. 92.85±42.17, p=0.147 and p=0.940, respectively).
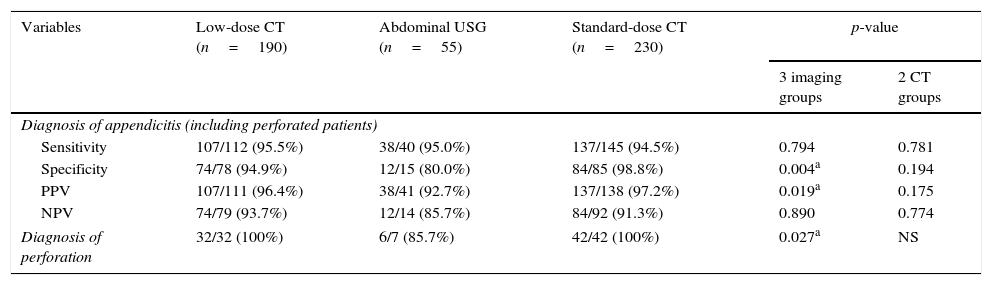
Comparison of the diagnosis of appendicitis based on imaging studiesThe usefulness of making a diagnosis of acute appendicitis based on imaging studies was compared in Table 2. There was no significant difference in the sensitivity between the three approaches (95.5% vs. 95.0% vs. 94.5%, respectively, p=0.794) and we even included the perforated appendix patients. There were significant differences in specificity and positive-predictive value (PPV) between the three groups (94.9% vs. 80.0% vs. 98.8%, respectively, p=0.004; and 96.4% vs. 92.7% vs. 97.2%, respectively, p=0.019). However, when the low-dose CT and the standard-dose CT groups were compared, there were no significant differences (p=0.194 and p=0.175, respectively) and both CT imaging modalities were superior when compared with USG. Moreover, there was no significant difference in the negative-predictive value (NPV) between the three groups (93.7% vs. 85.7% vs. 91.3%, respectively, p=0.890). In making a diagnosis of a perforated appendix, both low-dose CT and standard-dose CT were effective and relatively accurate. Thus, both CT modalities were more superior diagnostic tools when compared with USG (100.0% vs. 85.7% vs. 100.0%, respectively, p=0.027).
Comparison of availability between low dose computed tomography and abdominal ultrasonography or standard dose computed tomography in children with acute appendicitis.
| Variables | Low-dose CT (n=190) | Abdominal USG (n=55) | Standard-dose CT (n=230) | p-value | |
|---|---|---|---|---|---|
| 3 imaging groups | 2 CT groups | ||||
| Diagnosis of appendicitis (including perforated patients) | |||||
| Sensitivity | 107/112 (95.5%) | 38/40 (95.0%) | 137/145 (94.5%) | 0.794 | 0.781 |
| Specificity | 74/78 (94.9%) | 12/15 (80.0%) | 84/85 (98.8%) | 0.004a | 0.194 |
| PPV | 107/111 (96.4%) | 38/41 (92.7%) | 137/138 (97.2%) | 0.019a | 0.175 |
| NPV | 74/79 (93.7%) | 12/14 (85.7%) | 84/92 (91.3%) | 0.890 | 0.774 |
| Diagnosis of perforation | 32/32 (100%) | 6/7 (85.7%) | 42/42 (100%) | 0.027a | NS |
CT, computed tomography; USG, ultrasonography; PPV, positive predictive value; NPV, negative predictive value; NS, no significant difference.
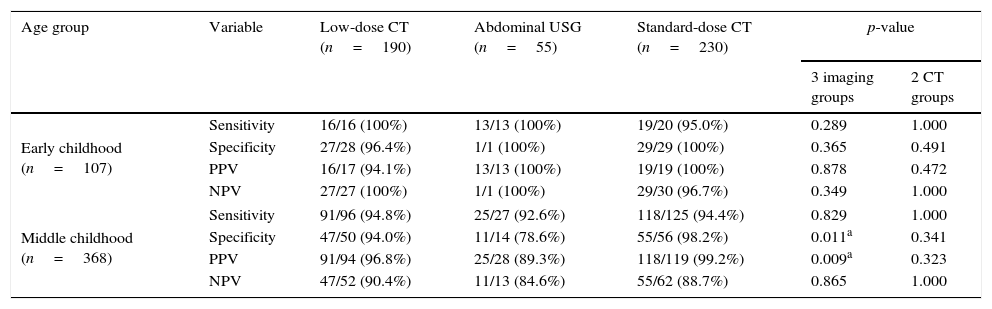
In early childhood, acute appendicitis was accurately diagnosed in all three groups: the low-dose CT group, the standard-dose CT group, and the USG group. In addition, there was no significant difference between the three groups (Table 3). When comparing low-dose with standard-dose CT, there was no significant differences in the sensitivity, specificity, PPV, and NPV between the two groups (100% vs. 95.0%, p=1.000; 96.4% vs. 100.0%, p=0.491; 94.1% vs. 100.0%, p=0.472; and 100% vs. 96.7%, p=1.000, respectively). Moreover, in middle childhood patients, there was no significant difference in the sensitivity between the three groups (94.8% vs. 92.6% vs. 94.4%, respectively, p=0.829). There was a significant difference in the specificity between the three groups (94.0% vs. 78.6% vs. 98.2%, respectively, p=0.011). However, there was no significant difference (p=0.341) between the low-dose CT and the standard-dose CT. Both groups showed a higher value than that of the USG group. PPV was significantly different between the USG and the two CT groups (96.8% vs. 89.3% vs. 99.2%, respectively, p=0.009). However, no significant difference in PPV was observed between the two CT groups (p=0.323). Furthermore, NPV was not significantly different between the three groups (90.4% vs. 84.6% vs. 88.7%, respectively, p=0.865).
Comparison of radiologic methods for diagnosis according to age group in children with acute appendicitis.
| Age group | Variable | Low-dose CT (n=190) | Abdominal USG (n=55) | Standard-dose CT (n=230) | p-value | |
|---|---|---|---|---|---|---|
| 3 imaging groups | 2 CT groups | |||||
| Early childhood (n=107) | Sensitivity | 16/16 (100%) | 13/13 (100%) | 19/20 (95.0%) | 0.289 | 1.000 |
| Specificity | 27/28 (96.4%) | 1/1 (100%) | 29/29 (100%) | 0.365 | 0.491 | |
| PPV | 16/17 (94.1%) | 13/13 (100%) | 19/19 (100%) | 0.878 | 0.472 | |
| NPV | 27/27 (100%) | 1/1 (100%) | 29/30 (96.7%) | 0.349 | 1.000 | |
| Middle childhood (n=368) | Sensitivity | 91/96 (94.8%) | 25/27 (92.6%) | 118/125 (94.4%) | 0.829 | 1.000 |
| Specificity | 47/50 (94.0%) | 11/14 (78.6%) | 55/56 (98.2%) | 0.011a | 0.341 | |
| PPV | 91/94 (96.8%) | 25/28 (89.3%) | 118/119 (99.2%) | 0.009a | 0.323 | |
| NPV | 47/52 (90.4%) | 11/13 (84.6%) | 55/62 (88.7%) | 0.865 | 1.000 | |
CT, computed tomography; USG, ultrasonography; PPV, positive predictive value; NPV, negative predictive value.
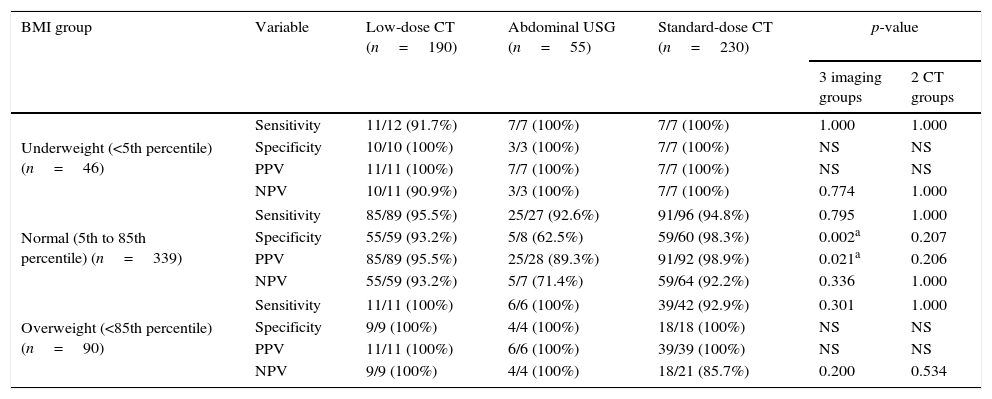
Table 4 shows the comparison of radiological methods for diagnosis according to age-specific BMI. In patients who were classified as underweight by less than five percentile points, diagnosis was not obtained in only one patient. Accurate diagnoses were made in all three groups. Furthermore, in patients with normal BMI, the sensitivity and NPV showed no significant differences between groups (95.5% vs. 92.6% vs. 94.8%, p=0.795 and 93.2% vs. 71.4% vs. 92.2%, p=0.336, respectively). In addition, the specificity and PPV showed no significant differences between the two types of CT doses, and were higher in the CT groups than in the USG group (93.2% vs. 98.3%, respectively, p=0.207; and 95.5% vs. 98.9%, respectively; p=0.206). Furthermore, in overweight patients, diagnosis was not obtained in only three patients. However, there was no significant difference in the diagnosis based on the three radiological methods.
Comparison of radiologic methods for diagnosis according to BMI in children with acute appendicitis.
| BMI group | Variable | Low-dose CT (n=190) | Abdominal USG (n=55) | Standard-dose CT (n=230) | p-value | |
|---|---|---|---|---|---|---|
| 3 imaging groups | 2 CT groups | |||||
| Underweight (<5th percentile) (n=46) | Sensitivity | 11/12 (91.7%) | 7/7 (100%) | 7/7 (100%) | 1.000 | 1.000 |
| Specificity | 10/10 (100%) | 3/3 (100%) | 7/7 (100%) | NS | NS | |
| PPV | 11/11 (100%) | 7/7 (100%) | 7/7 (100%) | NS | NS | |
| NPV | 10/11 (90.9%) | 3/3 (100%) | 7/7 (100%) | 0.774 | 1.000 | |
| Normal (5th to 85th percentile) (n=339) | Sensitivity | 85/89 (95.5%) | 25/27 (92.6%) | 91/96 (94.8%) | 0.795 | 1.000 |
| Specificity | 55/59 (93.2%) | 5/8 (62.5%) | 59/60 (98.3%) | 0.002a | 0.207 | |
| PPV | 85/89 (95.5%) | 25/28 (89.3%) | 91/92 (98.9%) | 0.021a | 0.206 | |
| NPV | 55/59 (93.2%) | 5/7 (71.4%) | 59/64 (92.2%) | 0.336 | 1.000 | |
| Overweight (<85th percentile) (n=90) | Sensitivity | 11/11 (100%) | 6/6 (100%) | 39/42 (92.9%) | 0.301 | 1.000 |
| Specificity | 9/9 (100%) | 4/4 (100%) | 18/18 (100%) | NS | NS | |
| PPV | 11/11 (100%) | 6/6 (100%) | 39/39 (100%) | NS | NS | |
| NPV | 9/9 (100%) | 4/4 (100%) | 18/21 (85.7%) | 0.200 | 0.534 | |
BMI, body mass index; CT, computed tomography; USG, ultrasonography; PPV, positive predictive value; NPV, negative predictive value; NS, no significant difference.
In pediatric patients, it is highly possible that acute appendicitis may present with atypical clinical features. A complication, such as perforated appendix, may manifest as the initial symptom of appendicitis. Therefore, it is crucial to make an early diagnosis of acute appendicitis, particularly in these young patients. To minimize the delay in diagnosis and false-positive and/or false-negative diagnoses, decision on and interpretation of radiological evaluation are essential.21–25
However, with the increased interest in the occurrence of cancer due to radiation exposure, there have been concerns about CT scanning.7,26,27 Many studies have indicated the usefulness of low-dose CT in the diagnosis of acute appendicitis. However, no study has reported on the efficacy of using low-dose CT to do so in children, including in infants and young children. In the present study, the authors have examined the usefulness and accuracy of different radiological examinations, depending on the age group and age-specific BMI. Unlike previous studies, it was attempted to confirm that low-dose CT is also effective in the early childhood group.
The present results confirmed that low-dose CT is effective in making a diagnosis of acute appendicitis, including the diagnosis of perforated appendix patients, when compared with USG or standard-dose CT. Following a comparison based on the age group, it was also confirmed to be effective in both early childhood and middle childhood groups. In addition, in a comparison based on the age-specific BMI, low-dose CT was confirmed to be effective in making a diagnosis of acute appendicitis not only in underweight patients, but also in overweight patients. Low-dose CT was effective in making a diagnosis in all patients, particularly in those whose BMI was above the 95th percentile. In all cases, low-dose CT was shown to be more effective than or similarly effective as standard-dose CT or USG in terms of sensitivity, specificity, PPV, and NPV. These findings were similar to those of previous pediatric studies on other diseases. Moreover, it agrees with previous studies based on an adult population on the usefulness of low-dose CT in making a diagnosis of acute appendicitis.11,12
However, due to the retrospective nature of the study, CT was not performed using a certain pre-determined dose; rather, the dose was determined by age and weight. For these reasons, there was no consistency in the tube voltage or current. In particular, the range was relatively wider in the case of standard-dose CT. In addition, the mean age was slightly lower in the low-dose CT group than in the standard-dose CT group. Nonetheless, there was no age-related significant difference between the two CT groups. Furthermore, there was also no significant difference in the number of patients in each group. In addition, the radiation dose was actually lower by approximately 64.2% in the low-dose CT group.
In the current study, of the 614 patients (including those who were excluded due to an undefined radiation dose) in whom USG or CT was performed due to the suspicion of appendicitis, 388 actually had appendicitis and the remaining 226 did not. During the diagnostic procedure, patients presenting with other diseases, based on test results, such as intussusception or malignancy, were initially excluded. In addition, the study also excluded those in which the purpose of radiological evaluation was unclear; therefore, the number of patients in the negative group might be greater, and the actual NPV may also be higher than that found in this study.
However, the present results do not support the imprudent use of low-dose CT for diagnosing acute appendicitis. According to the National Academy of Science report about health risks from exposure to low levels of ionizing radiation, BEIR VII, there would be a linear increase in the risk of developing cancer even at a low dose, without a specific threshold.28 This should also be accompanied by the definition of a rationale that is appropriate for the age and radiation dose used in each center. In recent years, abdominal USG has been used as the first-line of measure for making a diagnosis of acute appendicitis not only in adults, but also in children. In equivocal cases, a CT is performed. This staging protocol has been studied and reported, and should be applied in a clinical setting.18,29 In these cases, low-dose CT may become an alternative modality to standard-dose CT. Furthermore, in the present study, regarding the cases in which a CT was performed after USG, there were four patients in the low-dose CT group and five patients in the standard-dose CT group. An accurate diagnosis was made at a probability of 100% in all 15 patients, including in the six patients who were excluded from the current analysis, due to a lack of accurate dose data.
There are several limitations to the present study. The number of patients diagnosed by USG was smaller than the number of patients diagnosed with appendicitis by of low-dose CT; therefore, it was not possible to make a direct comparison between these two options. However, numerous previous studies have investigated diagnosis via USG, which has been found to be greatly dependent on the expertise or subjective judgment of the observer. Moreover, there was no notable difference in the degree of diagnostic accuracy by USG between this and previous studies.30,31 Therefore, the present results indicate that low-dose CT is not inferior to USG in the diagnosis of appendicitis.
In conclusion, low-dose CT is effective and relatively accurate for diagnosing acute appendicitis of patients in childhood, as well as in adolescence and young adulthood. Moreover, low-dose CT was highly accurate, regardless of age or BMI, for detecting acute appendicitis. Therefore, low-dose CT may be a superior diagnostic tool when compared with USG, and may be an alternative modality to standard-CT for assessing pediatric patients suspected of having acute appendicitis.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Yi DY, Lee KH, Park SB, Kim JT, Lee NM, Kim H, et al. Accuracy of low dose CT in the diagnosis of appendicitis in childhood and comparison with USG and standard dose CT. J Pediatr (Rio J). 2017;93:625–31.





