

To verify whether the occurrence of acute viral bronchiolitis in the first year of life constitutes a risk factor for asthma at age 6 considering a parental history of asthma.
MethodsCross-sectional study in a cohort of live births. A standardized questionnaire of the International Study of Asthma and Allergies in Childhood was applied to the mothers to identify asthma in children at the age of 6 years. Acute viral bronchiolitis diagnosis was performed by maternal report of a medical diagnosis and/or presence of symptoms of coryza accompanied by cough, tachypnea, and dyspnea when participants were 3, 6, 9, and 12 months. Socioeconomic, environmental data, parental history of asthma, and data related to pregnancy were collected in the first 72h of life of the newborn and in prospective home visits by trained interviewers. The association between acute viral bronchiolitis and asthma was evaluated by logistic regression analysis and potential modifier effect of parental history was verified by introducing an interaction term into the adjusted logistic regression model.
ResultsPrevalence of acute viral bronchiolitis in the first year of life was 68.6% (461). The occurrence of acute viral bronchiolitis was a risk factor for asthma at 6 years of age in children with parental history of asthma OR: 2.66, 95% CI (1.10–6.40), modifier effect p=0.002. Parental history of asthma OR: 2.07, 95% CI (1.29–3.30) and male gender OR: 1.69, 95% CI, (1.06–2.69) were other identified risk factors for asthma.
ConclusionAcute viral bronchiolitis in the first year of life is a risk factor for asthma in children with parental history of asthma.
Verificar se a ocorrência de bronquiolite viral aguda (BVA) no 1° ano de vida constitui fator de risco para asma aos seis anos de idade considerando a história parental de asma.
MétodosEstudo de corte transversal aninhado a uma coorte de nascidos vivos. O questionário padronizado do International Study of Asthma and Allergies in Children (ISAAC) foi aplicado às mães para identificar asma nas crianças na idade de seis anos. O diagnóstico de BVA foi realizado por relato materno de diagnóstico médico e/ou presença de sintomas de coriza acompanhados de tosse, taquipneia e dispneia quando os participantes tinham 3, 6, 9 e 12meses. Dados socioeconômicos, ambientais, história parental de asma e referentes à gestação foram coletados nas primeiras 72 horas de vida do recém-nascido e em visitas domiciliares prospectivas por entrevistadores treinados. Associação entre BVA e asma foi avaliada por análise de regressão logística e potencial efeito modificador da história parental verificada pela introdução do termo de interação no modelo de regressão logística ajustada.
ResultadosA prevalência de BVA no 1° ano de vida foi 68,6% (461). A ocorrência de BVA foi fator de risco para asma aos seis anos de idade em crianças com história parental de asma OR: 2,66 (1,10-6,40), efeito modificador p= 0,002. História parental de asma OR: 2,07 IC95% (1,29-3,30) e sexo masculino OR:1,69 IC95% (1,06-2,69) foram outros fatores de risco identificados para asma.
ConclusãoBVA no 1° ano de vida é fator de risco para asma em crianças com história parental de asma.
Asthma is the most prevalent chronic disease in children, resulting in high demand for care in emergency departments as well as hospitalizations,1,2 with a negative impact on quality of life of children and adults.3
Several studies have shown an association between bronchiolitis, recurrent wheezing, and asthma.4,5 Acute viral bronchiolitis (AVB) is the most common viral disease of the lower airways in infants, characterized by inflammation, edema, and necrosis of small airway epithelial cells, with increased mucus production and bronchospasm, whose diagnosis is mainly clinical.6
The pathogens involved in AVB include respiratory syncytial virus (RSV), rhinovirus, influenza A and B, parainfluenza, metapneumovirus, adenovirus, papillomavirus, and bocavirus.7 RSV is the most common pathogen, responsible for 70% of episodes of bronchiolitis in children younger than 2 years. Changes in the immune response of children with a parental history of asthma affected by AVB caused by RSV and rhinovirus are implicated in this virus/asthma association.8–10 Reinfection is common during the first two years of life.11 In Brazil, RSV is responsible for 31.9–64% of hospitalizations for AVB12,13 and co-infections occur in 40% of cases, with rhinovirus being the most common agent.14
Despite the evidence of the association between AVB and clinical manifestations of asthma, there have been few studies evaluating the action of genetic predisposition in this association. Thus, the role of the AVB as a marker of asthma in children with a parental history of the disease in the development of medium and long-term asthma is not exactly known.
The aim of this study was to investigate the association between AVB in the 1st year of life and asthma in children at 6 years of age, according to a parental history of asthma and other confounding variables in a cohort of live births in the Northeast of Brazil.
MethodsThe cross-sectional study was carried out in a large northeastern city in Brazil with data obtained from a cohort of live births. The cohort was established between April 2004 and March 2005, with the consecutive inclusion of live births from all ten hospitals in the city of Feira de Santana, born to mothers living in the city. The data used in the study were related to those collected in the hospital and during four home visits in the first year of life (3, 6, 9, and 12 months) and at 6 years.
The inclusion criteria were: mothers and their children living in that city; infants born to mothers who had no perinatal complications; newborns who were not admitted to the nursery for a period longer than 24h.
The exclusion criteria were: children born to mothers with health problems that contraindicated breastfeeding and mothers that were legally separated from their children.
Data collection toolChildren who were included in the cohort at birth were followed monthly by previously trained health care workers through monthly household interviews in the first 6 months of life and then were followed every three months up to the end of the first year, and at scheduled ages and at the sixth year of life.
SampleSample size calculation was performed in two stages, namely, sample calculation to estimate the prevalence of asthma in children, and then calculating the sample to identify independent asthma predictors.
The asthma prevalence sample calculation was carried out using the PEPI SAMPLE program (WINPEPI computer programs) using the following parameters: estimated prevalence of asthma in schoolchildren of 20%, confidence interval of 95%, and accuracy of 1.25% around the estimated prevalence of the population. The result showed the need to study 202 children, plus an expected loss of 10%, totaling 223 subjects.
To identify bronchiolitis as an asthma predictor, the sample calculation was carried out using the OpenEpi (Open Source Epidemiologic Statistics for Public Health, version 2.3.1) program, based on the following parameters: prevalence of AVB of 27%, confidence interval of 95%, statistical power of 80%, and relative-risk estimate of 2, considering the prevalence of asthma of 10% in non-exposed and 20% in those exposed to respiratory infections. According to the latter calculation, the minimum sample size consisted of 438 individuals.
Between the two calculations, the one with the highest number of participants was chosen (438 individuals). However, all 684 children aged 6 years who were followed in the cohort were included in the study.
VariablesThe definition of active asthma at 6 years of age was obtained by applying the standardized ISAAC15 study questionnaire to mothers according to an affirmative answer to the question: Has your child had “wheezing” in the last 12 months?
The clinical diagnostic criterion of AVB followed the definition of the American Academy of Pediatrics,16 that is, rhinorrhea accompanied by tachypnea, cough, dyspnea, and intensification of respiratory symptoms such as nasal flaring and intercostal and/or subcostal retractions. Thus, this condition was considered when the child's mother affirmatively answered that her child had a respiratory illness and the physician reported AVB as the diagnosis or reported symptoms of rhinorrhea, accompanied by cough, tachypnea, or dyspnea in the last 15 days, during the interviews at 3, 6, 9, and 12 months of life.
Co-variablesThe other co-variables were gestational age (<37 weeks, ≥37 weeks); parity (primiparous, multiparous); household income (<2 minimum wages, ≥2 minimum wages); maternal level of schooling (<8 years of schooling, ≥8 years of schooling); gender (male, female); birth weight (<2500g, ≥2500g); number of rooms in the household (<5 rooms, ≥5 rooms); number of individuals sleeping in the same room with the child (<4 individuals, ≥4 individuals); maternal smoking during pregnancy (yes, no); presence of dog or cat at home (yes, no); day care attendance up to 2 years (yes, no); truck traffic on the street where the household is located (yes, no); exclusive breastfeeding until the 3rd month (yes, no); exclusive breastfeeding until the 4th month (yes, no). Maternal clinical data were collected shortly after birth in the maternity wards and verified by checking their respective medical records.
Parental history of asthma was considered according to mother's answer to the question: “Does the child's father or mother have/still has asthma?” (Yes, no).
Statistical analysisThe frequency of the sociodemographic characteristics was calculated and the chi-squared test was used to compare proportions, with p-values <0.05 considered significant. Multivariate logistic regression models were used to assess factors associated with asthma at age 6 and AVB at 3, 6, 9, and 12 months, and in the 1st year of life, considering the main confounding variables and those with p-values ≤0.10 in the bivariate analysis.
The modifier effect of parental history of asthma in the association between AVB and asthma was verified by including the interaction term between parental history of asthma and AVB in the multivariate logistic regression analysis. Statistical analyses were performed using the SPSS (SPSS for Windows, version 14.0, Chicago, USA) program.
Ethical aspectsThis study, as well as the free and informed consent form, were approved by the Research Ethics Committee of Universidade Estadual de Feira de Santana.
ResultsA total of 672 of 684 eligible children participated in the study (98.2%), as 12 children were not located due to change in home address. The assessed sample had 30 more participants than the previously estimated sample. The prevalence of active asthma was 13.8%.
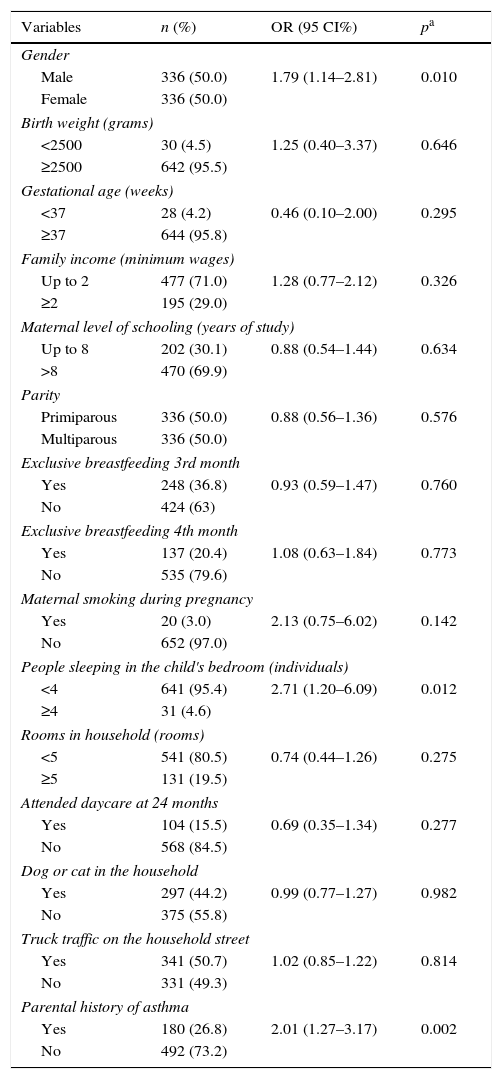
The clinical and demographic characteristics of the sample are shown in Table 1. Most of the children slept in rooms with fewer than four individuals and were children of parents with no history of asthma.
Sample characteristics and association of variables with asthma (n=672).
| Variables | n (%) | OR (95 CI%) | pa |
|---|---|---|---|
| Gender | |||
| Male | 336 (50.0) | 1.79 (1.14–2.81) | 0.010 |
| Female | 336 (50.0) | ||
| Birth weight (grams) | |||
| <2500 | 30 (4.5) | 1.25 (0.40–3.37) | 0.646 |
| ≥2500 | 642 (95.5) | ||
| Gestational age (weeks) | |||
| <37 | 28 (4.2) | 0.46 (0.10–2.00) | 0.295 |
| ≥37 | 644 (95.8) | ||
| Family income (minimum wages) | |||
| Up to 2 | 477 (71.0) | 1.28 (0.77–2.12) | 0.326 |
| ≥2 | 195 (29.0) | ||
| Maternal level of schooling (years of study) | |||
| Up to 8 | 202 (30.1) | 0.88 (0.54–1.44) | 0.634 |
| >8 | 470 (69.9) | ||
| Parity | |||
| Primiparous | 336 (50.0) | 0.88 (0.56–1.36) | 0.576 |
| Multiparous | 336 (50.0) | ||
| Exclusive breastfeeding 3rd month | |||
| Yes | 248 (36.8) | 0.93 (0.59–1.47) | 0.760 |
| No | 424 (63) | ||
| Exclusive breastfeeding 4th month | |||
| Yes | 137 (20.4) | 1.08 (0.63–1.84) | 0.773 |
| No | 535 (79.6) | ||
| Maternal smoking during pregnancy | |||
| Yes | 20 (3.0) | 2.13 (0.75–6.02) | 0.142 |
| No | 652 (97.0) | ||
| People sleeping in the child's bedroom (individuals) | |||
| <4 | 641 (95.4) | 2.71 (1.20–6.09) | 0.012 |
| ≥4 | 31 (4.6) | ||
| Rooms in household (rooms) | |||
| <5 | 541 (80.5) | 0.74 (0.44–1.26) | 0.275 |
| ≥5 | 131 (19.5) | ||
| Attended daycare at 24 months | |||
| Yes | 104 (15.5) | 0.69 (0.35–1.34) | 0.277 |
| No | 568 (84.5) | ||
| Dog or cat in the household | |||
| Yes | 297 (44.2) | 0.99 (0.77–1.27) | 0.982 |
| No | 375 (55.8) | ||
| Truck traffic on the household street | |||
| Yes | 341 (50.7) | 1.02 (0.85–1.22) | 0.814 |
| No | 331 (49.3) | ||
| Parental history of asthma | |||
| Yes | 180 (26.8) | 2.01 (1.27–3.17) | 0.002 |
| No | 492 (73.2) | ||
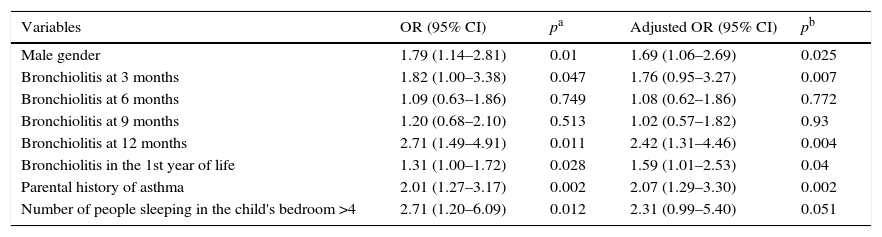
The risk factors for asthma in the logistic regression analysis were male gender, having a parental history of asthma, and AVB at 3 and 12 months, and in the 1st year of life (Table 2).
Factors associated to asthma at the logistic regression analysis (n=672).
| Variables | OR (95% CI) | pa | Adjusted OR (95% CI) | pb |
|---|---|---|---|---|
| Male gender | 1.79 (1.14–2.81) | 0.01 | 1.69 (1.06–2.69) | 0.025 |
| Bronchiolitis at 3 months | 1.82 (1.00–3.38) | 0.047 | 1.76 (0.95–3.27) | 0.007 |
| Bronchiolitis at 6 months | 1.09 (0.63–1.86) | 0.749 | 1.08 (0.62–1.86) | 0.772 |
| Bronchiolitis at 9 months | 1.20 (0.68–2.10) | 0.513 | 1.02 (0.57–1.82) | 0.93 |
| Bronchiolitis at 12 months | 2.71 (1.49–4.91) | 0.011 | 2.42 (1.31–4.46) | 0.004 |
| Bronchiolitis in the 1st year of life | 1.31 (1.00–1.72) | 0.028 | 1.59 (1.01–2.53) | 0.04 |
| Parental history of asthma | 2.01 (1.27–3.17) | 0.002 | 2.07 (1.29–3.30) | 0.002 |
| Number of people sleeping in the child's bedroom >4 | 2.71 (1.20–6.09) | 0.012 | 2.31 (0.99–5.40) | 0.051 |
The number of children exposed to AVB in the 1st year of life was 50.7% (341) and the frequency of AVB was 461 episodes: 75 (11.5%) in the first, 136 (20.3%) in the second, 114 (16.9%) in the third, and 136 (20.3%) in the fourth trimester of life. The frequency of AVB/child in the first year of life was one episode, 234; two episodes, 83; and three or more episodes, 15. The frequency of AVB was not associated with increased risk of asthma at the age of 6 years (Table 3).
Frequency of AVB episodes and association with asthma.
The prevalence of exclusive breastfeeding up to the 3rd month of life among the children was 36.4% (248), and was a protective factor for AVB, OR=0.49, 95% CI (0.28–0.84); p=0.009. Exclusive breastfeeding up to the 4th month did not result in protection against bronchiolitis at 6 months, OR: 0.76, 95% CI (0.42–1.16); 9 months OR: 1.19, 95% CI (0.74–1.93); 12 months, OR: 0.08, 95% CI (0.94–2.29), nor in the children's 1st year of life, OR: 0.60, 95% CI (0.29–1.24).
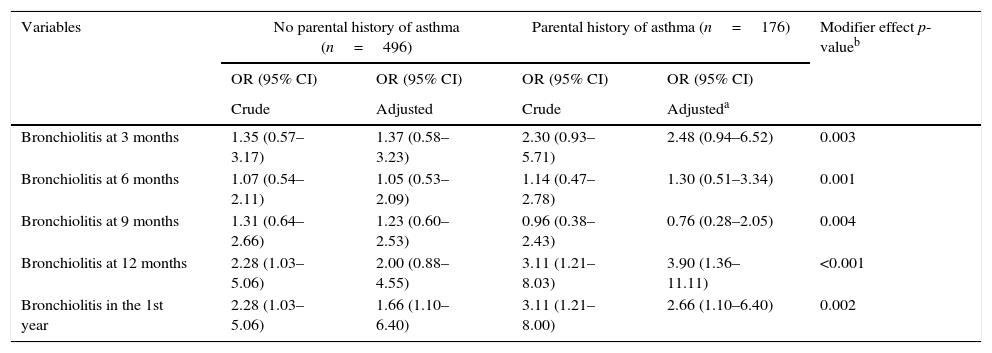
There was an modifier effect of the parental history of asthma for the association between bronchiolitis and asthma at 3, 6, 9, and 12 months, and in the 1st year; AVB at 12 months and in the 1st year of life was a risk factor for asthma in children with parental history of asthma, OR: 3.90 95% CI (1.36–11.1), and OR: 2.66, 95% CI (1.10–6.40), modifier effect p<0.001 and p=0.002, respectively (Table 4).
Association between AVB and asthma according to parental history of asthma.
| Variables | No parental history of asthma (n=496) | Parental history of asthma (n=176) | Modifier effect p-valueb | ||
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Crude | Adjusted | Crude | Adjusteda | ||
| Bronchiolitis at 3 months | 1.35 (0.57–3.17) | 1.37 (0.58–3.23) | 2.30 (0.93–5.71) | 2.48 (0.94–6.52) | 0.003 |
| Bronchiolitis at 6 months | 1.07 (0.54–2.11) | 1.05 (0.53–2.09) | 1.14 (0.47–2.78) | 1.30 (0.51–3.34) | 0.001 |
| Bronchiolitis at 9 months | 1.31 (0.64–2.66) | 1.23 (0.60–2.53) | 0.96 (0.38–2.43) | 0.76 (0.28–2.05) | 0.004 |
| Bronchiolitis at 12 months | 2.28 (1.03–5.06) | 2.00 (0.88–4.55) | 3.11 (1.21–8.03) | 3.90 (1.36–11.11) | <0.001 |
| Bronchiolitis in the 1st year | 2.28 (1.03–5.06) | 1.66 (1.10–6.40) | 3.11 (1.21–8.00) | 2.66 (1.10–6.40) | 0.002 |
The present study shows that AVB in the 1st year of life was a risk factor for asthma in children and significantly increases when associated with a parental history of asthma. Exposure to AVB and other multiple environmental factors is important for the development of the disease, especially in predisposed children.17
Respiratory infections by viruses and AVB are more common in infants, and have been associated with risk of asthma, as they are related to its pathogenesis and the triggering of exacerbations.17,18 Although some infections caused by influenza and parainfluenza viruses can inhibit the development of asthma, despite repeated upper airway respiratory infections in the first two years of the child's life, other infections by RSV and rhinovirus may favor the onset of asthma and atopy.7,19,20
There are several hypotheses to explain the mechanisms involved in the association between viral infection, persistent dyspnea, and asthma: (i) induction of inflammation typical of allergic asthma by T lymphocyte differentiation into Th2; (ii) activation by the respiratory syncytial virus of Th17 cells and IL17 production, a neutrophilic inflammation-inducing cytokine. Th17 cells induce the regulation of other pro-inflammatory cytokines, such as IL6 and TNF-α, chemokines, and metalloproteinases, with a possible role in the pathogenesis of asthma21,22; (iii) increase in IL-4 and decrease in IFN-gamma levels, as demonstrated by the presence of positive allergy tests and specific IgE antibodies in children with AVB; (iv) bronchial hyperactivity mediated by inflammatory cells and sensory C-fiber neuropeptides caused by the increase in bronchial inflammation. Other risk factors for asthma in children may be related to the direct association between bronchiolitis and asthma, such as the presence of smaller-caliber airways in male children, which may lead to dyspnea during virus infections and the development of asthma.
The type of bacterial flora that comprises the nasopharynx microbiome of children in the early years of life has been associated to future risk of asthma. Nasopharyngeal colonization by Streptococcus pneumoniae, Moraxella catarrhalis, and Haemophilus influenzae at the age of 1 month of life is associated with risk of asthma at age 5 years. RSV infection at an early age can change the nasopharyngeal microbiome, and the microflora imbalance can lead to lower respiratory tract infection by pathogenic bacteria and inflammation.21
There have been few studies considering the modifier effect of parental history of asthma in the association between AVB caused by RSV and rhinovirus and asthma development in children. Carroll et al. demonstrated that the presence of rhinovirus was associated with more severe infection in children of mothers with atopic asthma.23 Similarly, Jung et al. demonstrated through genotyping that an modifier effect of TLR4 (rs1927911), CD14 (rs2569190), and IL-13 (rs20541) occurred in the association between asthma and AVB in Korean children; the risk of developing asthma after AVB was significantly higher in children that had one of the three polymorphisms described above.24 It is well known that a parental history of asthma is the most important risk factor for asthma development.25 In the current study, it was an independent risk factor for asthma and played an important modifying effect on the association between AVB and asthma, increasing the risk of asthma in children with bronchiolitis.
A study carried out in the city of Salvador, state of Bahia, Brazil, to verify the association between viral infections and asthma among children aged 4–13 years showed no association between atopic and non-atopic asthma and the herpes simplex, varicella zoster, Epstein–Barr virus, and hepatitis A viruses,26 which are not associated to lower respiratory tract infections. Infections by herpes simplex and Epstein–Barr virus in children caused attenuation of the immediate hypersensitivity skin test verified by immediate aeroallergen hypersensitivity skin prick testing. The result of this study showed that viral infections commonly found in children have been associated with immediate hypersensitivity attenuation, but not the clinical disease.
The current study showed that the rate of exclusive breastfeeding rate in the 4th month of life was 20.4%, which is compatible with the national mean; this fact may have contributed to protect children from AVB and asthma at 3 months of life while in exclusive breastfeeding, due to the presence of immunological, anti-infectious factors, and immunomodulators present in human milk, according to the study by Kull et al.27
The prevalence of asthma in this study was lower when compared with the prevalence found in a previous study performed in the city of Feira de Santana.28 Possible reasons are the high rate of exclusive breastfeeding during the children's first four months of life and the asthma and allergic rhinitis control program actions implemented in the city in 2004, with the free distribution of asthma control drugs.1,2 Further studies planned for the future will add other criteria for disease identification, such as regular use of asthma medications, which can maintain patients asymptomatic.
Male gender and genetics also represented risk factors for asthma in this study. The 2.4-fold higher risk of asthma in male schoolchildren when compared to female ones was also found in the study by Casagrande et al. and can be justified by the smaller airway caliber of boys when compared to girls in this age group, which disappears in adolescence.29,30 Studies have shown that having parents with asthma is the main risk factor for having the disease.25
Some limitations inherent to cross-sectional studies, such as recall bias, have been minimized in the present study, as it was carried out in a prospective cohort of children. The diagnosis of asthma, using the ISAAC study questionnaire, was standardized and validated in Brazil, used to measure the overall prevalence of asthma and allergic disease symptoms in schoolchildren with questions limited to symptoms in the last year, thus reducing the recall bias. The diagnosis of AVB based on data provided by mothers on the medical diagnosis and the presence of respiratory tract symptoms can be faulty and may have overestimated the diagnosis of AVB. Febrile tachypnea and rhinorrhea are common in viral infections. The respiratory symptoms were not accompanied by fever in a significant percentage of the sample. Not performing serological tests for virus identification was also a limitation of the current study.
AVB in the 1st year of life was a risk factor for asthma in children in Northeast Brazil. Parental history of asthma further increases the risk of asthma in children exposed to bronchiolitis. The use of prevention and control measures for respiratory infections caused by RSV and rhinoviruses, such as vaccination for VSR, preventing contamination by washing hands, and avoiding crowded places, should be expanded and intensified by public health agencies, especially for children with a parental history of asthma, aiming to obtain a decrease in morbidity and mortality for bronchiolitis and asthma prevalence.
Conflicts of interestThe authors declare no conflicts of interest.
Paulo Camargos received grants from CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico, Grant #303396/2012-1) and FAPEMIG (Fundação de Amparo à Pesquisa do Estado de Minas Gerais, Grant #PPM0065-14)
Please cite this article as: Brandão HV, Vieira GO, Vieira TO, Cruz ÁA, Guimarães AC, Teles C, et al. Acute viral bronchiolitis and risk of asthma in schoolchildren: analysis of a Brazilian newborn cohort. J Pediatr (Rio J). 2017;93:223–9.
Study conducted at Escola Bahiana de Medicina e Saúde Pública, Salvador, BA, Brazil.





