


To examine longitudinal (seven years) relationships among cardiorespiratory fitness (VO2peak), body fatness, and motor competence.
MethodData were collected as part of the Copenhagen School Child Intervention Study (CoSCIS). Body fatness was assessed by the sum of four skinfolds. VO2peak was measured directly in a continuous running protocol. Motor competence was assessed using the Körperkoordinationtest für Kinder. This study used multilevel linear mixed models to evaluate the reciprocal longitudinal association between body fatness, VO2peak, and motor competence. All regressions were stratified by sex and adjusted by intervention and pubertal status. All variable coefficients were standardized.
ResultsA reciprocal relationship was observed between children's motor competence with body fatness and VO2peak at the seven-year follow-up (6–13 years of age). Children with higher motor competence at baseline had a lower risk of having higher body fatness (βboys=−0.45, 95% CI: −0.52 to −0.38; βgirls=−0.35, 95% CI: −0.42 to −0.28) and higher VO2peak (βboys=0.34, 95% CI: 0.27–0.40; βgirls=0.27, 95% CI: 0.20–0.33) during childhood. Alternatively, higher body fatness or lower levels of VO2peak at baseline were associated with lower motor competence during childhood.
ConclusionsThese data suggest motor competence, body fatness, and VO2peak demonstrate reciprocal relationships across childhood (6–13 years of age). Interventions addressing motor competence, cardiorespiratory fitness, and body fatness in early childhood are recommended, as intervention effects are likely to be enhanced because of the mutual reciprocal associations between these three variables.
Examinar as relações longitudinais (sete anos) entre a aptidão cardiorrespiratória (VO2 pico), gordura corporal e coordenação motora.
MétodoOs dados foram coletados como parte do Copenhagen School Child Intervention Study (CoSCIS). A gordura corporal foi avaliada pela soma de quatro dobras cutâneas. O VO2 pico foi medido diretamente em um protocolo de corrida contínua. A coordenação motora foi avaliada com o teste de coordenação corporal para crianças (Körperkoordination für Kinder – KTK). Usamos modelos lineares mistos multiníveis para avaliar a associação longitudinal recíproca entre a gordura corporal, o VO2 pico e a coordenação motora. Todas as regressões foram estratificadas por sexo e ajustadas para intervenção e estado puberal. Todos os coeficientes das variáveis foram padronizados.
ResultadosObservamos uma relação recíproca entre a coordenação motora e a gordura corporal. As crianças com maior coordenação motora no início do estudo apresentaram menor risco de ter maior nível de gordura corporal (βmeninos=-0,45, IC de 95%: -0,52: -0,38; βmeninas=-0,35, IC de 95%: -0,42: -0,28) e maior VO2 pico (βmeninos=0,34, IC de 95%: 0,27: 0,40; βmeninas=0,27, IC de 95%: 0,20: 0,33). Por outro lado, maior nível de gordura corporal ou menores níveis de VO2 pico no início do estudo foram associados a menor coordenação motora durante a infância.
ConclusõesEsses dados sugerem que a coordenação motora, gordura corporal e VO2 pico demonstram relações recíprocas durante a infância (6-13 anos). São recomendadas intervenções que abordem a coordenação motora, a aptidão cardiorrespiratória e a gordura corporal na primeira infância, pois os efeitos da intervenção são provavelmente maiores devido às associações recíprocas mútuas entre essas três variáveis.
Motor competence (MC) is indispensable for many functional and purposeful tasks in daily life, sports, and recreational activities. Alongside strength and power, MC is reflective of the cooperative function of the central and peripheral nervous systems and the musculoskeletal system.1 Recent research has demonstrated strong evidence of associations between MC and cardiorespiratory fitness,2,3 body weight status,2,3 and physical activity,3,4 suggesting that MC may have an important impact on children's health.3,5
Association between MC and body weight status is observed even in early childhood (5 years)6,7 and continues through early adulthood.8 Specifically, Lopes et al.9 and D’Hondt et al.7 analyzed cross-sectional associations between gross MC and weight status in children ages 6–14 and 5–12 years old, respectively, and noted that children with higher MC scores already demonstrated lower BMI at 5–6 years old. In addition, the inverse strength of associations between MC and BMI became larger with increasing age. Fransen et al.10 also observed the same phenomenon with two-year longitudinal data. Importantly, associations between MC and BMI were not mediated by physical activity in this study.10 Data from the previously mentioned studies and others provide indirect support for a heuristic model that proposes MC and body weight status will demonstrate reciprocal relationships across childhood, with increasing strengths of association across childhood.5,11
The model also proposes that MC and aspects of health-related physical fitness (i.e., cardiorespiratory endurance, muscular strength/endurance) will demonstrate the same reciprocal relationships across childhood. Recent review articles generally support these views.2,3,5 Cardiorespiratory fitness is consistently correlated with MC in children and adolescents, with recent a systematic review noting that 12 out of 12 studies demonstrated positive associations between MC and cardiorespiratory fitness.2 The development of gross MC promotes independent upright posture and locomotion in early childhood, which is suggested to influence the early improvement of cardiorespiratory fitness in children11via the repetitive nature of movement exploration (e.g., crawling, walking). Hands12 and Cairney and Veldhuizen13 observed that motorically delayed children had lower cardiorespiratory fitness performance compared to peers with higher gross motor coordination, with the difference remaining after two to five years of follow-up.
While the aforementioned cross-sectional and longitudinal data provide strong evidence for consistent inverse associations between MC and weight status and positive associations between MC and cardiorespiratory fitness, a causal pathway between these variables is still not clear. Recently, Robinson et al.5 compiled the literature that investigated the potential impact of MC on health-related factors. In summary, the authors noted that cardiorespiratory fitness (positively) and fatness (negatively) were longitudinally associated with MC during childhood. However, the possible reciprocal association between MC and fitness and fatness has not been fully addressed.
It is important to test whether relationships between MC, cardiorespiratory fitness, and fatness are reciprocal to provide knowledge to more successful interventions aiming to increase MC and fitness levels and decrease fatness during childhood and adolescence. This evidence can also support policy makers designing policies for this population. To provide a more comprehensive understanding of the long-term relationships between the health-related components of MC, cardiorespiratory fitness, and fatness, the authors analyzed the longitudinal associations (seven-year span from childhood into beginning adolescence) among fitness (VO2peak), fatness (sum of four skinfolds), and MC levels, and the potential reciprocal nature of these associations. More specifically, the strengths of the relationships among these variables were evaluated over time.
Material and methodsThis study was based on longitudinal analysis of data from the Copenhagen School Child Intervention Study (CoSCIS), which began in 2001. Children attending preschool class in two communities in the area of Copenhagen (46 preschool classes in 18 schools) were recruited to participate in the study. CoSCIS is a controlled longitudinal intervention study that took place in 18 public schools (ten interventions and eight controls) in two suburbs of Copenhagen. The local Authority of Ballerup had decided to upgrade the physical activity opportunities for their youngest schoolchildren and contacted the research group to quantify and measure the effect of such an intervention. The intervention was hereafter planned in cooperation between the local authority and the researchers. All children from 46 preschool classes (age 6–7 years) in the schools in the two local authorities were invited to participate in the study.14 The study was approved by the ethical committee, University of Copenhagen (reference KA00011gm). Written informed consent was obtained from the parents/guardians of 706 children (69% of the population), and 696 actually participated in the study at baseline. The intervention lasted three years and no key variables examined in this study were affected by the intervention.14 Children were followed up again in 2008 at 13 years.
Because the complete methodology has been previously published,14 the methodology here presents only those variables of interest. Bicipital, tricipital, subscapular, and suprailiac skinfolds were measured on the self-reported nondominant side of the body by the same two skilled researchers with a Harpender skinfold caliper (Harpender, West Sussex, United Kingdom), and fatness was computed as the sum of the four skinfolds (S4SF). Cardiorespiratory fitness (VO2peak) was assessed using a continuous running protocol on a treadmill until exhaustion. VO2peak was measured directly on an AMIS 2001 Cardiopulmonary Function Test System (Innovision, Odense, Denmark) at 6 and 9 years-of-age, and using a COSMED K4b2 portable metabolic system (COSMED, Rome, Italy) at 13 years-of-age. Both systems provide valid measures of VO2 when validated against the Douglas bag method.15–17 From 9 to 13 years of age, the pubertal status was reported using the Tanner scale,18 with pictures of breasts for girls and genital development for boys.
MC was assessed using the Körperkoordinationstest für Kinder (KTK), which is a standardized normative German test battery.19 The KTK has high test-retest reliability (0.90 to 0.97).19 It consists of four independent tests: (1) walking backwards on balance beams of decreasing width: 6.0, 4.5, and 3.0cm (KTKBEAM), (2) moving sideways on wooden boards for 20s (KTKBOARD), (3) one-legged hopping over a foam obstacle with increasing height in consecutive steps of 5cm (KTKHOP), and (4) two-legged jumping from side to side for 15s (KTKJUMP). The KTK battery has been used in numerous studies to evaluate MC performance levels in normally developing children and adolescents up to 15 years-of-age.20,21 The raw performance score on each item was summed and standardized in Z-scores (KTK Z-score) to evaluate the longitudinal association between the S4SF, VO2peak, and MC.
In all analyses, STATA version 13.0 was used (StataCorp, College Station, TX, USA). We performed multilevel linear regressions to evaluate the reciprocal longitudinal association between VO2peak, S4SF, and MC, and how this possible reciprocal longitudinal association would develop over time. Therefore, it was analyzed whether VO2peak and S4SF (exposure variables) influence MC (outcome) development, and also whether MC (exposure variable) impacts the development of VO2peak and S4SF (outcomes). Note that independent multilevel linear regressions were performed to evaluate the relationships between MC and VO2peak, and between MC and S4SF. Therefore, VO2peak and S4SF were not in the same regression models. Standardized β coefficients are presented for each testing time (results in figures) and the overall longitudinal relationship over seven years of follow-up (results in text), both provided by the same multilevel models. Standardized β coefficients are presented to help readers to compare the strength between coefficients. This approach has been used previously.22 Children with missing information in one of the three measuring points were included in the analyses. The hierarchical data structure was taken into account with students nested in school classes, and school classes nested in schools (random effects). The regressions were adjusted for group (intervention; control), and pubertal status (prepubertal, initial puberty, and puberty). All the analyses were stratified by sex (boys and girls).
In all multilevel regression models, the variance related to the clusters (school and classes within school) and the intraclass correlation coefficient (ICC) were calculated for each model to interpret the variation between school classes, classes, and individuals.23,24 In all regression models, the majority of the variation (ICC) was based on the individual level (the conjugated ICCs from school and classes were always below 5%). All regression models were tested for linearity between dependent and independent variables; normality of the regression equation residuals; and the variance equality of the equation residuals.
ResultsThe majority of the boys at 9 years of age were in the initial stages of genitalia development (95.4% in stage 1 and 4.6% in stage 2). At 13 years of age, most of the boys characterized themselves in stage 3 in genitalia development (45.7%), followed by stage 4 (40.3%), stages 2 and 5 (6.3% each), and stage 1 (1.4%). At 9 years of age, 54.7% of the girls recognized themselves as being in stage 1 regarding their breast development, while 40.4% reported being in stage 2 and 4.9% reported being in stage 3. At 13 years of age, most of the girls characterized themselves as being in stage 4 (55.3%), 23.3% reported being in stage 3, 15.2% reported being in stage 5, 5.7% reported being in stage 2, and 0.5% reported being in stage 1.
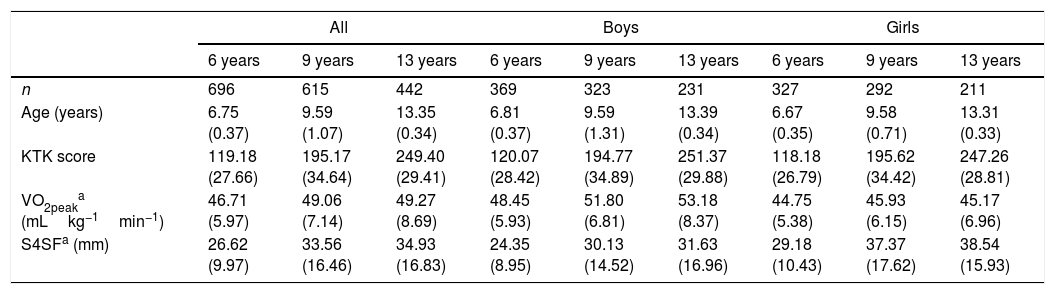
Table 1 presents the physical and motor characteristics of the participants in each age period of monitoring. Differences were observed in VO2peak and S4SF between boys and girls in all age ranges.
Mean (SD) physical and motor characteristics of participants by age and sex.
| All | Boys | Girls | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 6 years | 9 years | 13 years | 6 years | 9 years | 13 years | 6 years | 9 years | 13 years | |
| n | 696 | 615 | 442 | 369 | 323 | 231 | 327 | 292 | 211 |
| Age (years) | 6.75 (0.37) | 9.59 (1.07) | 13.35 (0.34) | 6.81 (0.37) | 9.59 (1.31) | 13.39 (0.34) | 6.67 (0.35) | 9.58 (0.71) | 13.31 (0.33) |
| KTK score | 119.18 (27.66) | 195.17 (34.64) | 249.40 (29.41) | 120.07 (28.42) | 194.77 (34.89) | 251.37 (29.88) | 118.18 (26.79) | 195.62 (34.42) | 247.26 (28.81) |
| VO2peaka (mLkg−1min−1) | 46.71 (5.97) | 49.06 (7.14) | 49.27 (8.69) | 48.45 (5.93) | 51.80 (6.81) | 53.18 (8.37) | 44.75 (5.38) | 45.93 (6.15) | 45.17 (6.96) |
| S4SFa (mm) | 26.62 (9.97) | 33.56 (16.46) | 34.93 (16.83) | 24.35 (8.95) | 30.13 (14.52) | 31.63 (16.96) | 29.18 (10.43) | 37.37 (17.62) | 38.54 (15.93) |
KTK, Körperkoordinationtest für Kinder; S4SF, sum the four skinfolds.
Results indicated MC and S4SF demonstrated a reciprocal influence on each other across time for both boys and girls. For both boys and girls, S4SF had a stronger association in the development of MC (βboys=−0.45 Z-scores, 95% CI: −0.52 to −0.38; βgirls=−0.35 Z-scores, 95% CI: −0.42 to −0.28), as opposed to MC influencing the development of S4SF (βboys=−0.31 Z-scores, 95% CI: −0.36 to −0.26; βgirls=−0.26 Z-scores, 95% CI: −0.31 to −0.20). The strength of the longitudinal association between MC and S4SF was also evaluated over time. For boys, the strength of the association between MC and S4SF increased across follow-up time points, independent of the direction analyzed. While for girls, an increase in the strength of the association was observed from 6 to 9 years-of-age, and maintenance of the strength of the association from 9 to 13 years-of-age, independent of the direction analyzed (Fig. 1).
 Gray line: S4SF (exposure) and MC (outcome); (b) black line: MC (exposure) and S4SF (outcome). Adjusted for: group (intervention; control), and pubertal status (prepubertal, initial puberty and puberty). S4SF, sum the four skinfolds; MC, motor competence.")
Parameter estimates of the slope for the association between S4SF and MC at 6, 9, and 13 years of age. (a) Gray line: S4SF (exposure) and MC (outcome); (b) black line: MC (exposure) and S4SF (outcome). Adjusted for: group (intervention; control), and pubertal status (prepubertal, initial puberty and puberty).
S4SF, sum the four skinfolds; MC, motor competence.
Independent of sex, MC and VO2peak also demonstrated reciprocal relationships across time. Although for boys, MC demonstrated a stronger influence on VO2peak (βboys=0.34 Z-scores, 95% CI: 0.27–0.40), as opposed to the influence of VO2peak on the development of MC (βboys=0.24 Z-scores, 95% CI: 0.18–0.30). While for girls, results did not demonstrate a marked differential effect of one variable on the development of the other variable across time (VO2peak→MC; βgirls=0.25 Z-scores, 95% CI: 0.18–0.32) (MC→VO2peak; βgirls=0.27 Z-scores, 95% CI: 0.20–0.33). Evaluating the pattern of associations between MC and VO2peak across the time points in boys, independent of the direction analyzed, it was possible to observe an increase in the strength of the association from 6 to 9 years-of-age and a subsequent maintenance at 13 years-of-age. While for girls, the strength of the association that MC had on the development of VO2peak was relatively stable during the follow-up period (0.24≤β≥0.30). On the other hand, the impact of VO2peak on MC increased from 6 to 9 years-of-age and stabilized from nine to 13 years-of-age (Fig. 2).
 Gray line: VO2peak (exposure) and MC (outcome); (b) black line: MC (exposure) and VO2peak (outcome). Adjusted for: group (intervention; control), and pubertal status (prepubertal, initial puberty, and puberty). MC, motor competence.")
Parameter estimates of the slope for the association between VO2peak and MC at 6, 9, and 13 years of age. (a) Gray line: VO2peak (exposure) and MC (outcome); (b) black line: MC (exposure) and VO2peak (outcome). Adjusted for: group (intervention; control), and pubertal status (prepubertal, initial puberty, and puberty). MC, motor competence.
Overall, this study observed a reciprocal relationship between children's MC with S4SF and VO2peak across the seven-year follow-up (6–13 years of age). Children with lower MC performance at baseline had higher risk of having higher S4SF and lower VO2peak during childhood. Alternatively, higher S4SF or lower levels of VO2peak at baseline were associated with lower MC development across time. Except for the stable longitudinal relationship between MC and VO2peak for girls, the strength of the association between MC and S4SF and VO2peak increased from 6 to 9 years of age and then was fairly stable from 9 to 13 years of age in both boys and girls, independent of the direction analyzed (MC→S4SF, S4SF→MC; MC→VO2peak, VO2peak→MC).
To the best of our knowledge, this is the first long-term follow-up study (seven years) to evaluate the potential reciprocal relationship between MC and S4SF that also evaluated the strength of the association over time. Robinson et al.5 also noted the lack of literature addressing these important developmental findings and thus, these data add to the existing literature in this area. As most previous studies addressing these variables used BMI as their assessment of obesity status, the use of skinfolds in the present study provided a more valid measure of body fat across childhood and into adolescence, when BMI becomes a less valid measure of obesity.25 The current data expand on previous four-year longitudinal data published by Lopes et al.,21 who also observed that children with higher MC at baseline demonstrated lower body fatness across time, as measured by the sum of skinfolds. Overall, the mutual relationship between MC and body fat across childhood suggests the need to consistently address them, via intervention on both factors to potentialize the effects of the intervention.
The present study partially supports the heuristic model proposed by Stodden et al.,11 which hypothesizes that MC and body weight status will demonstrate reciprocal relationships across childhood with increasing strengths of associations across childhood. It is logical that heavier children face problems to be active and develop their MC, as compared to their normal weight peers. Alternatively, children who demonstrate lower MC demonstrate less success and enjoyment in many developmentally appropriate activities (e.g., sports and games); thus, they are less likely to continue to participate in activities that inherently demand various forms of MC.11 This further hinders MC development and physical activity participation, and promotes negative developmental trajectories of MC, weight status, and fitness.26 In fact, it was possible to observe reciprocal associations between S4SF and MC that became stronger across age (boys: increase during the whole period of monitoring) or remained stable (girls: increase until 9 years of age with subsequent stabilization), which could mean that successful intervention with a focus on both unhealthy weight gain (i.e., nutrition and physical activity) and low MC in early childhood might have greater sustained impact across childhood.26
Of course, children's cardiovascular endurance is not independent from either obesity or MC. The demonstrated reciprocal relationship between MC and cardiovascular endurance partially demonstrates this affect. Few studies have analyzed the association between MC and fitness level longitudinally,2,12,27 but to the best of our knowledge, none have analyzed if MC and VO2peak mutually influence the development of each other during childhood. In particular, the majority of studies have only looked at the influence of MC on physical fitness.5 It has been shown that lower MC negatively influences cardiorespiratory fitness development.10,12,28 In a six-year follow-up study (10 year-old children at baseline), Barnett et al.27 observed that MC at baseline predicted the fitness level in Australian children. Complementarily, perceived sports competence mediated this relationship. It was interesting to note that the present data indicated MC has a larger suggested impact on VO2peak development than the reverse causality from 6 to 9 years-of-age. However, from ages of 9 to 13 or for girls, the regression models did not demonstrate stronger relationships in either direction. According to these results, the capability to successfully participate in many different activities that inherently require adequate levels of MC probably generates more opportunities to be physically active, thus leading to higher cardiorespiratory fitness and decreased body fatness.11 Subsequently, higher cardiorespiratory fitness would allow for longer participation, and a higher chance to develop better MC.11
In particular, the different pattern of the relationships between MC, S4SF, and VO2peak for boys and girls might be partially explained by their pubertal status. Because MC, S4SF, and VO2peak did not differ for boys and girls due to the effects of the initial intervention that was conducted from the ages of 6 to 9 years14 and because girls reach higher pubertal status sooner than boys, it is possible that the physical development was being influenced by their maturational status. In addition, the fact that girls decrease their participation in physical activities sooner than boys might also influence the pattern of the relationships between MC, S4SF, and VO2peak.29
This study had some limitations that have to be considered in the interpretation of the results. This longitudinal study was part of an intervention project and some results could be influenced by the intervention; however, this study presented a follow-up of four years after the intervention ended and the analyses were adjusted for group (intervention, control). In addition, the intervention did not influence MC development, VO2peak, or S4SF.14 Longitudinal studies provide valuable inferences about causal mechanisms; however, evidence for causality would be further strengthened with experimental evidence. It would be valuable to assess pubertal status by a more precise measure. Some of the differences in the associations between boys and girls might be explained by differences in pubertal status. Another limitation is the fact that the nutrition/diet and physical activity level of the participants were not accounted for in the study, which may have influenced the association between variables.
The development of MC, S4SF, and VO2peak trajectories across childhood and into adolescence (6–13 years of age) seems to be the result of reciprocal mechanisms. It seems logical that interventions should address MC, cardiorespiratory fitness, and other factors associated with body fatness in early childhood, as early intervention effects are likely to be enhanced because of the reciprocal and potentially synergistic associations between these three variables across time. As noted, by the increasing strength of associations across both time points or in at least one longitudinal time point, promoting MC, fitness, and a healthy weight status in early childhood can promote positive developmental trajectories of these variables across childhood and into adolescence.
FundingThis work was supported by a CAPES Scholarship, number: 1361/13-9, The Danish Heart Foundation, and TrygFonden.
Conflicts of interestThe authors declare no conflicts of interest.
The authors are thankful to all participating children and their families, school principals, and teachers, and the politicians and employees of the local authorities of Ballerup and Tårnby.
Please cite this article as: Lima RA, Bugge A, Ersbøll AK, Stodden DF, Andersen LB. The longitudinal relationship between motor competence and measures of fatness and fitness from childhood into adolescence. J Pediatr (Rio J). 2019;95:482–8.




