
To carry out a systematic review on the relationship of bullying with type 1 diabetes in children and adolescents.
MethodsSystematic review, according to the PRISMA methodology, in which the databases PubMed, Web of Science, Scopus, Thomson Reuters, Eighteenth Century Collections Online, Begell House Digital Library, LILACS, and SciELO were searched using the terms “bullied”, “aggression”, “peer victimization”, “victimization”, “school violence”, “diabetes mellitus”, “type 1 diabetes mellitus”, “autoimmune diabetes”, “children” and “adolescents.” The authors included original studies, involving bullying associated with type 1 diabetes, with children and adolescents, without language restriction and publication period, with texts available in full.
ResultsOf the 32 articles found, four studies met the selection criteria. Of these studies 85.7% identified occurrence of victimization in diabetics or found a higher frequency in diabetic children and adolescents when compared with young people with other chronic conditions or with healthy peers. Association between bullying and worse glycemic control was observed in two studies, and all the studies mention the fact that type 1 diabetes is a limiting factor for socialization related to diabetes, with less social support and difficulties for the management of the disease in public environments, such as school. The type of bullying suffered varied, including physical, verbal, social, psychological, and sexual.
ConclusionMost of the studies showed an association between bullying and type 1 diabetes when compared to individuals with no such condition. Knowledge of this association has become essential for the follow-up of these patients and the implementation of preventive programs.
Realizar uma revisão sistemática sobre a relação do bullying com o diabetes tipo 1 em crianças e adolescentes.
MétodosRevisão sistemática, conforme a metodologia PRISMA, onde foram pesquisadas as bases de dados Pubmed, Web of Science, Scopus, Thomson Reuters, Eighteenth Century Collections Online, Begell House Digital Library, Lilacs e SciELO, usando os termos “bullying”, “bullied”, “aggression”, “peer victimization”, “victimization”, “school violence”, “diabetes mellitus”, “type 1 diabetes”, “type 1 diabetes mellitus”, “autoimmune diabetes”, “children” and “adolescents”. Foram incluídos estudos originais, envolvendo bullying associado ao diabetes tipo 1, com população de crianças e adolescentes, sem restrição de idioma e período de publicação, com textos disponíveis na íntegra.
ResultadosDos 32 artigos encontrados, quatro atenderam aos critérios de seleção. Desses estudos, 85,7% identificaram ocorrência de vitimização em diabéticos ou constataram maior frequência em crianças e adolescentes diabéticos quando comparados com jovens com outras condições crônicas ou sadios. Associação entre bullying e pior controle glicêmico foi observada em dois estudos e todos os estudos mencionam o fato de ser portador do diabetes tipo 1, um fator limitante para socialização relacionado ao diabetes, com menor apoio social e dificuldades para o manejo da doença em ambientes públicos, como a escola. O tipo de bullying sofrido variou entre físico, verbal, social, psicológico e sexual.
ConclusãoA maioria dos estudos evidenciou associação entre vitimização por bullying e diabetes tipo 1, quando comparada com indivíduos com ausência dessa condição. O conhecimento dessa associação torna-se fundamental para acompanhamento desses pacientes e implantação de programas preventivos.
Bullying is defined as a repetitive physical or psychosocial force usually exercised by a stronger person against a weaker person that can lead to an unbalanced power dynamic between the aggressor and victim.1 Bullying and physical strife are reported to be frequent behavioral disorders occurring early in adolescence.2,3 Bullying is recognized as a major concern as it is associated with poor school performance and mental health problems.4
In 2008, the World Health Organization (WHO) published a report on the behavior of approximately 200,000 children and adolescents of both sexes aged 11, 13, and 15 years in 41 countries and regions in Europe and North America.5 In Brazil, several studies have been published investigating bullying in Brazilian schools, including an epidemiological study involving 60,973 schoolchildren from 1452 public and private schools in 26 capitals, including the Federal District, where it was shown that 32.6% of the boys and 29.1% of the girls encountered bullying in the 30 days prior to the survey.6
Research suggests that children and adolescents with chronic diseases have more difficulty psychologically adjusting, and are more likely to have emotional and behavioral problems.7 T1D is one of the most common chronic diseases to affect the child/adolescent population, affecting approximately 2/3 of all cases of diabetes in this demographic.8 It is the most common endocrinopathy in childhood and adolescence, and may jeopardize growth, development, and psychosocial adjustment.9 Delamater10 considers that psychosocial factors are the most important influences that affect the care and treatment of the disease. Thus, new therapeutic approaches for all types of diabetes require not only greater involvement by patients, but also people who provide them with social support.11
Common signs of stress in these patients include changes in sleep patterns, changes in appetite, anxious thoughts, and irritability.12 General emotional stress can affect the blood glucose levels and glycemic control, and interfere with the ability to self-manage diabetes. Moreover, it has been found to be associated with poor quality of life.13,14 Stressful experiences influence diabetes control not only because of the devastating effect on poor blood glucose control but also because of the association between high blood glucose levels and the development of diabetes-related complications.13,15 For example, in prospective studies involving individuals with T1D, patients who reported negative stress showed deteriorating glycemic control over time.16
In addition to the physiological influence that stress has on glycemia, stress interferes with the ability to self-manage diabetes, such as monitoring glucose frequently, following a meal plan, and correctly preparing or remembering to take insulin or oral medication at the right time.13 Exposure to bullying predisposes individuals to long-term physical and psychological effects. In addition to its short-term effects such as various somatic symptoms, anxiety, depression, and social problems, exposure to bullying in childhood and adolescents can lead to poor self-esteem, poor peer relationships, and higher rates of depression in adulthood.17
In children and adolescents with T1D specifically, research shows that stress stems from the need to manage a complex medical condition that requires daily completion of multiple self-care behaviors; the impact of diabetes on social interactions with family members, peers, and teachers; and the interference of symptoms such as hypoglycemia with daily activities.18
Therefore, children with T1D may be at greater risk than their healthy peers for intimidation due to their associated disease management routines (e.g., home glucose monitoring, multiple insulin injections, dietary restrictions) that may be stigmatizing, making them potential targets of bullies.19 In many cases, children report being victims due to the needs/particularities caused by the disease pathology.20
When considering the particularities of adolescence, the age group with the highest incidence of T1D, the psychosocial aspects deserve to be highlighted, because this is a phase of sudden changes in the physiological, psychological, and social aspects. Therefore, attention to psychosocial aspects should also be incorporated into the treatment of these individuals in search of adherence to treatment and better metabolic control.21
Based on this information, it is important to investigate bullying and its effects on the management of T1D in children, in order to demonstrate its occurrence, to avoid/ameliorate the damages caused by bullying, and to improve the condition of children and adolescents who are victims of bullying. The repercussions of bullying on the lives of diabetic children, combined with the lack of studies that have investigated the issue, justifies the present review. The objective of this study was to conduct a systematic review of the influence of bullying on T1D mellitus in children and adolescents.
MethodsA systematic review of the literature on bullying associated with T1D mellitus in children and adolescents was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology.22 The search sources were PubMed, Web of Science, Scopus, Thomson Reuters, Eighteenth Century Collections Online, Begell House Digital Library, LILACS, and SciELO.
The descriptors used in the search strategy were bullied, aggression, peer victimization, victimization, school violence, diabetes mellitus, T1D mellitus, autoimmune diabetes, children, and adolescents. The search used the Boolean operators “AND” and “OR” resulting in the search detail as follows: “bullying” OR “bullied” OR “aggression” OR “peer victimization” OR “victimization” OR “school violence” OR “stigma” AND “diabetes mellitus” OR “T1D mellitus” OR “autoimmune diabetes” AND “children” AND “adolescents.”
The following inclusion criteria were used: original epidemiological studies (cohort study, cross-sectional study, case–control study, and clinical trial) and non-epidemiological (qualitative) studies involving bullying associated with T1D mellitus, with a target population of children and adolescents (aged between 3 and 17 years). The outcome of interest was an evaluation of the occurrence of bullying in individuals with T1D, and any associations with disease management (capillary glycemia, insulin therapy, diet therapy) and control. Studies that compared victimization among diabetics, healthy individuals, and those with other chronic diseases were also included. Studies that used specific scales and/or questionnaires to investigate the occurrence of bullying, without restriction of language and period of publication, with texts available in full were included.
Excluded from the analysis were double indexed articles, literature reviews, case reports that evaluated the occurrence of bullying in patients with chronic diseases without specifying T1D, and studies that identified bullying through scales for evaluation of anxiety, stress, suffering, or depression.
After consulting the databases and applying the search strategies, all resulting abstracts were read. In cases where the summary reading was not sufficient to establish whether the article should be incorporated, the article was read in its entirety to determine its eligibility. When the summary was sufficient, the article was selected, and full versions were obtained for confirmation of eligibility and inclusion in the study. Two independent researchers carried out the selection, along with a judge who has expertise in systematic reviews, in cases of disagreement of article inclusion.
Analyses of the studies were descriptive and performed in two stages. The first stage included a description of the methodological characteristics: authorship, country/year of publication, interview location, study design, sample, and population characteristics. The second stage comprised a measure of the occurrence of the study outcomes and the factors associated with these outcomes,22 i.e., the main results with a description of the occurrence of bullying, the type of bullying, type of aggressors, and influence on T1D management in the target population. Because this was a systematic review of the literature and the material evaluated is freely available in databases, there was no need for an evaluation by the Research Ethics Committee.
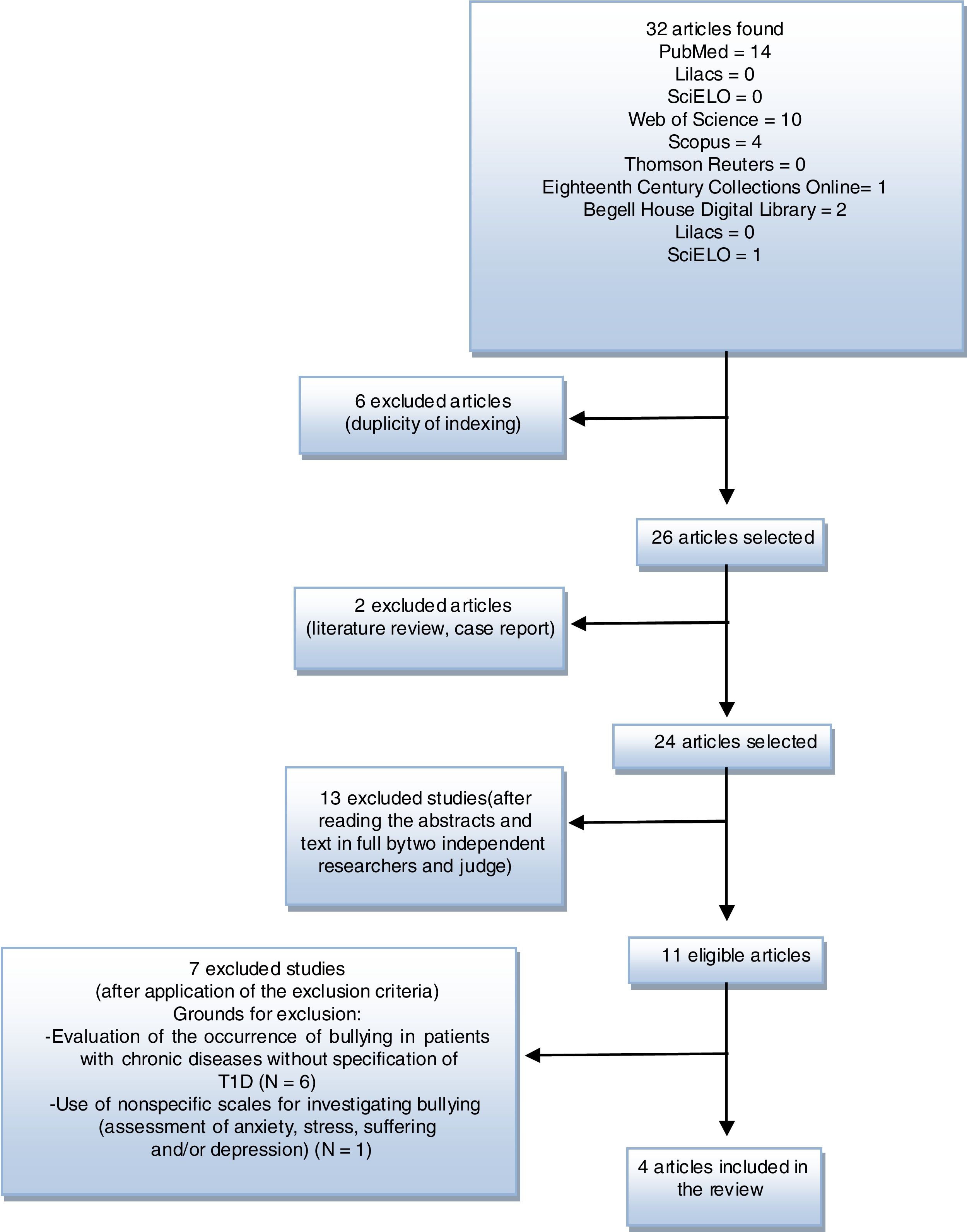
ResultsBy July 2017, 32 articles were found; after the elimination of eight studies, because they were literature reviews, case reports, and/or double indexed, 26 articles were selected. Of these, 13 were excluded after an analysis of titles and abstracts. Of the 11 eligible articles, seven were excluded for the following reasons: evaluation of the occurrence of bullying in patients with chronic diseases without specification of T1D and use of nonspecific scales for investigating bullying (evaluation of anxiety, stress, suffering, and/or depression).
In the end, four studies were included in the present systematic review, with one containing adult individuals (outside the defined age group). However, this was still included by conducting a retrospective investigation of bullying by referencing the childhood/adolescence of the participants. Fig. 1 presents a synthesis of the article selection process.

All studies were conducted in the United States and England, published between 1999 and 2008, and conducted at general health and/or specific pediatric endocrinology services. The studies presented a quantitative methodological approach.
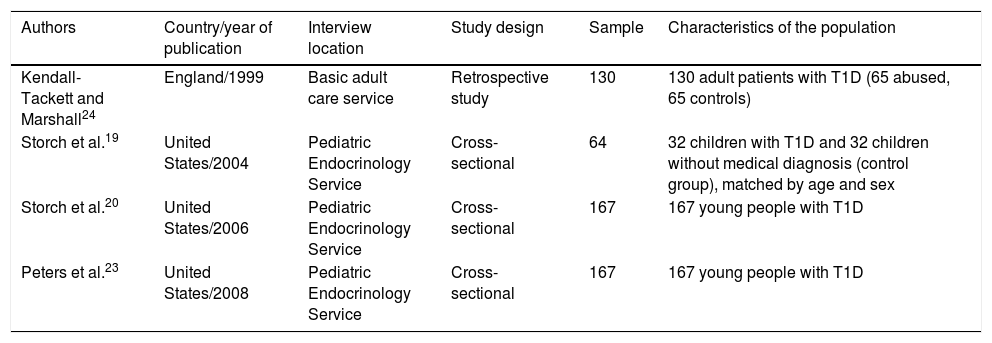
Methodologically, three studies presented cross-sectional designs and one study was a longitudinal cohort. The sample sizes ranged from 64 to 167 children and adolescents, with three studies identified as having over 100 participants. Among the characteristics of the study populations, bullying was investigated only in individuals with T1D, in comparison with other chronic diseases and in contrast to healthy children (Table 1).
Methodological characteristics of the studies included in the review.
| Authors | Country/year of publication | Interview location | Study design | Sample | Characteristics of the population |
|---|---|---|---|---|---|
| Kendall-Tackett and Marshall24 | England/1999 | Basic adult care service | Retrospective study | 130 | 130 adult patients with T1D (65 abused, 65 controls) |
| Storch et al.19 | United States/2004 | Pediatric Endocrinology Service | Cross-sectional | 64 | 32 children with T1D and 32 children without medical diagnosis (control group), matched by age and sex |
| Storch et al.20 | United States/2006 | Pediatric Endocrinology Service | Cross-sectional | 167 | 167 young people with T1D |
| Peters et al.23 | United States/2008 | Pediatric Endocrinology Service | Cross-sectional | 167 | 167 young people with T1D |
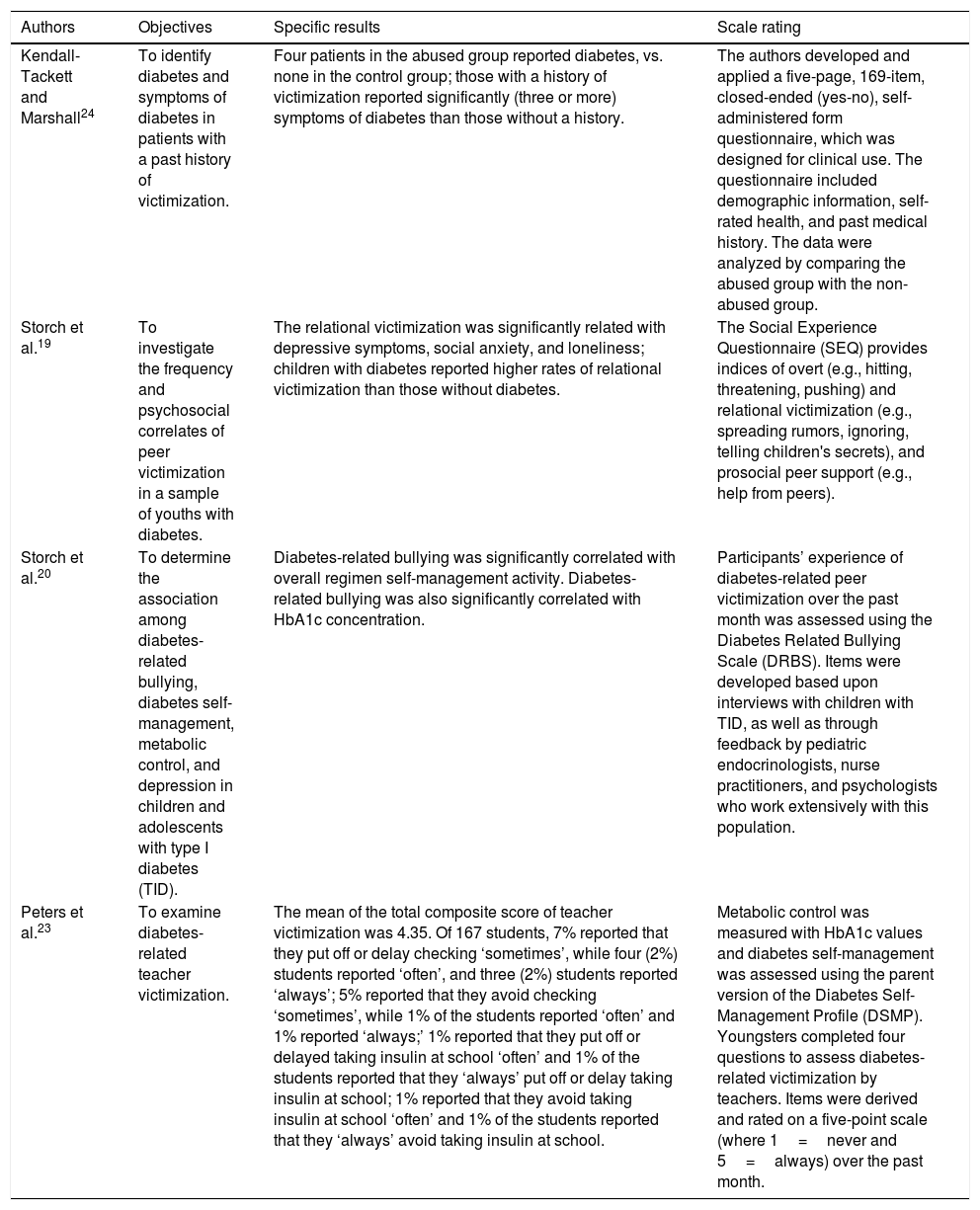
All included studies carried out research using questionnaires to assess the occurrence of bullying; one used an audio interview. The variables studied included the frequency/occurrence of bullying episodes, the type of bullying and aggressor, the reaction of the school and teachers to the bullying, social interactions and the support of friends/classmates (peers), as well as the influence of victimization on glycemic control. The description the objectives, measures of specific results, and evaluation of the scale of the studies included in the review can be observed in Table 2.
Description the objectives, measures of specific results, and evaluation of the scale of the studies included in the review.
| Authors | Objectives | Specific results | Scale rating |
|---|---|---|---|
| Kendall-Tackett and Marshall24 | To identify diabetes and symptoms of diabetes in patients with a past history of victimization. | Four patients in the abused group reported diabetes, vs. none in the control group; those with a history of victimization reported significantly (three or more) symptoms of diabetes than those without a history. | The authors developed and applied a five-page, 169-item, closed-ended (yes-no), self-administered form questionnaire, which was designed for clinical use. The questionnaire included demographic information, self-rated health, and past medical history. The data were analyzed by comparing the abused group with the non-abused group. |
| Storch et al.19 | To investigate the frequency and psychosocial correlates of peer victimization in a sample of youths with diabetes. | The relational victimization was significantly related with depressive symptoms, social anxiety, and loneliness; children with diabetes reported higher rates of relational victimization than those without diabetes. | The Social Experience Questionnaire (SEQ) provides indices of overt (e.g., hitting, threatening, pushing) and relational victimization (e.g., spreading rumors, ignoring, telling children's secrets), and prosocial peer support (e.g., help from peers). |
| Storch et al.20 | To determine the association among diabetes-related bullying, diabetes self-management, metabolic control, and depression in children and adolescents with type I diabetes (TID). | Diabetes-related bullying was significantly correlated with overall regimen self-management activity. Diabetes-related bullying was also significantly correlated with HbA1c concentration. | Participants’ experience of diabetes-related peer victimization over the past month was assessed using the Diabetes Related Bullying Scale (DRBS). Items were developed based upon interviews with children with TID, as well as through feedback by pediatric endocrinologists, nurse practitioners, and psychologists who work extensively with this population. |
| Peters et al.23 | To examine diabetes-related teacher victimization. | The mean of the total composite score of teacher victimization was 4.35. Of 167 students, 7% reported that they put off or delay checking ‘sometimes’, while four (2%) students reported ‘often’, and three (2%) students reported ‘always’; 5% reported that they avoid checking ‘sometimes’, while 1% of the students reported ‘often’ and 1% reported ‘always;’ 1% reported that they put off or delayed taking insulin at school ‘often’ and 1% of the students reported that they ‘always’ put off or delay taking insulin at school; 1% reported that they avoid taking insulin at school ‘often’ and 1% of the students reported that they ‘always’ avoid taking insulin at school. | Metabolic control was measured with HbA1c values and diabetes self-management was assessed using the parent version of the Diabetes Self-Management Profile (DSMP). Youngsters completed four questions to assess diabetes-related victimization by teachers. Items were derived and rated on a five-point scale (where 1=never and 5=always) over the past month. |
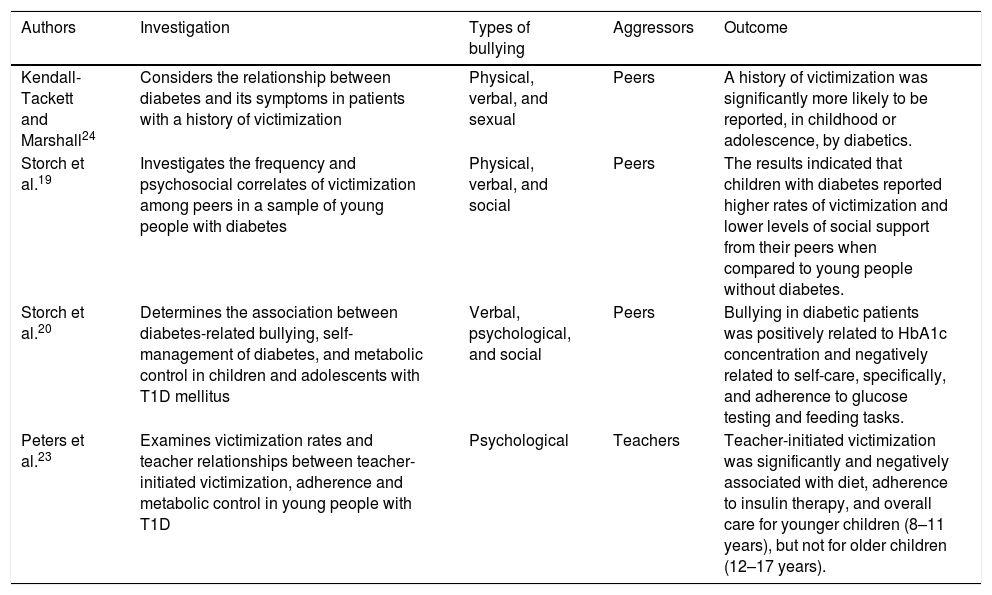
Of the selected studies, all identified the occurrence of victimization in diabetics, or found a higher frequency in diabetic children and adolescents compared to young people with healthy conditions. An association between bullying, and worse glycemic control was observed in two studies. All studies found T1D to be a limiting factor for successful socialization, with less social support and increased difficulties in the management of the disease in public settings such as schools. The type of bullying suffered was diverse and included physical, verbal, social, psychological, and sexual. The outcome was constructed by grouping the main results of the studies, with relevance given to associations between the studied variables (Table 3).
Characteristics of the investigation, type of bullying, aggressors, and outcome observed in the reviewed studies.
| Authors | Investigation | Types of bullying | Aggressors | Outcome |
|---|---|---|---|---|
| Kendall-Tackett and Marshall24 | Considers the relationship between diabetes and its symptoms in patients with a history of victimization | Physical, verbal, and sexual | Peers | A history of victimization was significantly more likely to be reported, in childhood or adolescence, by diabetics. |
| Storch et al.19 | Investigates the frequency and psychosocial correlates of victimization among peers in a sample of young people with diabetes | Physical, verbal, and social | Peers | The results indicated that children with diabetes reported higher rates of victimization and lower levels of social support from their peers when compared to young people without diabetes. |
| Storch et al.20 | Determines the association between diabetes-related bullying, self-management of diabetes, and metabolic control in children and adolescents with T1D mellitus | Verbal, psychological, and social | Peers | Bullying in diabetic patients was positively related to HbA1c concentration and negatively related to self-care, specifically, and adherence to glucose testing and feeding tasks. |
| Peters et al.23 | Examines victimization rates and teacher relationships between teacher-initiated victimization, adherence and metabolic control in young people with T1D | Psychological | Teachers | Teacher-initiated victimization was significantly and negatively associated with diet, adherence to insulin therapy, and overall care for younger children (8–11 years), but not for older children (12–17 years). |
All studies showed a relationship between bullying and T1D mellitus, and when diabetics were compared with children and adolescents with or without a chronic condition, they presented greater victimization.19,20,23,24
Delamater10 considers that psychosocial factors are the most important influences that affect the care and treatment of the disease. Storch et al.19 consider that children with T1D may be at greater risk than their healthy counterparts to be intimidated because of the obvious life behavior associated with disease management (e.g., glucose monitoring, multiple insulin injections), which may be stigmatizing and may also make these patients potential victims of bullying.19 In many cases, children report being bullied because of the needs/particularities of the disease.20
Difficulties may also arise because of negative attitudes toward disease by peers and teachers that perpetuate the belief that children with T1D are “different.” When these adolescents are seen as different, as abnormal compared to the standard, their peers may refuse to include them in the group, pushing them away or even assaulting them, thus making them victims of bullying.25
There are some hypotheses that try to explain why children with chronic diseases such as T1D are likely victims of bullying. Some authors suggest external causes of victimization, arguing that students with chronic diseases are more likely to be intimidated due to differences in appearance or behavior (mannerisms, speech patterns).26,27 When these adolescents are seen as different, non-standard, or abnormal, their peers can make them the target of nicknames/jokes, thus making them victims of bullying. These reasons are related to the high report of victimization by means of nicknames and cursing.
In regards to the type of social bullying, adolescents reported victimization through exclusion as the type of aggression routinely experienced. Because of their T1D status, young people may be less involved in social activities, thus placing them at greater risk of intimidation.28,29 Insults regarding physical characteristics were also reported by participants, and the literature suggests a relationship with T1D.
Added to this are reports of children and adolescents who associate physical differences as motivation for the practice of psychological violence between peers.30 When these adolescents are viewed as different, their peers may want to assault them.25 This shows an associated relationship with the percentage of responses affirming the occurrence of physical bullying, as evinced by the behavior is expressed by hitting, such as kicking, pushing, pinching, snapping, elbowing, and punching; taking, stealing, or damaging belongings; attack with objects; spitting; and physical threats. Verbal aggression, in turn, is manifested basically through insults; nicknames/name-calling; humiliation, intimidation and provocation; verbal offenses; threats; whispering about the victim; criticism; and revelry.6
Sexual bullying has been addressed in these studies; however, the occurrence of youth harassment may be a risk factor for occurrence of the sexual type, which may have been underreported. In this sense, a study indicates that patients with a history of victimization were significantly more likely to be diabetic or to have symptoms of diabetes than their non-abused peers.24
In relation to psychological/social bullying, typical aggressions were ignoring, isolating, excluding, and rejecting the peer in studies, or in jokes, or treating them with indifference and contempt; discriminating against them in regards to physical characteristics arising from the disease; threatening; defaming, slandering, and starting rumors; chasing; weakening self-esteem, the latter common among teachers.6
Besides that, children with T1D may be at greater risk for intimidation and bullying than their healthy counterparts because of behaviors associated with disease management (e.g., self-monitoring of blood glucose, multiple insulin injections, dietary restrictions) that may be stigmatizing.19
Among the attempts to explain why children with chronic diseases such as T1D are more often victims of bullying than their peers, some authors suggest external causes of victimization, arguing that students with chronic diseases are more likely to be intimidated due to differences in appearance or behavior (mannerisms, speech patterns).26,27
Children and adolescents with chronic conditions showed more limited social integration and peer support.31 They were more likely to have fewer friends and lower levels of support. Chronic diseases, such as T1D, which lead to less involvement of young people in social activities, place them at greater risk of being bullied and excluded.28,29
Boys with T1D had lower levels of support/peer support than girls with T1D and healthy boys and girls.31 These findings are consistent with previous research.32 It may be that students with chronic diseases have greater difficulty in developing psychosocial relationships due to fears of rejection by peers. These teenagers may choose to remain isolatedfrom their peer group.33
In regards to psychological bullying, difficulties may also arise due to the negative attitudes of teachers that help to perpetuate the belief that children with T1D are “different”.20 Young people victimized by their teachers may avoid engaging in self-management behaviors related to diabetes.34 According to one study, the absence of such management behaviors might put them at medical risk since without proper regulation, their blood glucose levels can reach dangerously high or low levels.23
Bullying is a sever problem that can lead to many serious situations such as suicide, homicide, and learning difficulties on the part of the victim.6 Among the influences of bullying in the health-disease process of children and adolescents with T1D, depression stands out. However, the prevalence of bullying in the health-disease process of young diabetics presented in the studies might have been masked, since its onset may be due to other psychological aspects, where, perhaps, children and adolescents with T1D are more likely to report bullying due to underlying depression or other anxieties than their non-diabetic peers. This demonstrated the importance of the study of this phenomenon associated with the investigation of depression and other psychological and emotional adaptations intrinsic to living with the disease.
The present study26 indicates that bullying-related depression can contribute to a lower adherence to treatment, impairing self-care and, consequently, contributing to the appearance of complications in the long term.
Depression is a common comorbidity among patients with diabetes,35 especially in developing countries such as Brazil. A recent survey indicated that, globally, individuals with diabetes had greater odds of experiencing an episode of depressive symptoms than those without diabetes.35 Diabetes patients with depression are at increased risk for poor glycemic control and development of cardiovascular complications and have higher mortality rates.36–38 One of the behavioral mechanisms that may link depression with poor outcomes in diabetes is suboptimal diabetes self-care behaviors.
It is worth mentioning that T1D patients are less able to cope with these situations, because they present feelings of inferiority, insecurity and alienation. At this stage of vulnerability, if the treatment requirements exclude the patient from social life or make they feel different from the group, conflicts may increase and compliance is unlikely.39 However, this impact will depend on the perception the patient and their family, the way they deal with self-care and the management of the disease, and the family functioning as a whole.
A difficulty indicated by the children and adolescents of the studies as a factor that interferes with the management of the disease, is T1D-related bullying. In one study, metabolic control was inversely proportional to the occurrence of bullying, and the authors suggested that poor management of diabetes contributed to patients being bullied.20 Stress associated with peer relationships can also directly affect blood glucose levels, or may interfere with self-care behavior, which in turn affects metabolic control.31
A recent study conducted among Dutch patients showed that, in particular, depressed mood, sleeping difficulties, appetite problems, and suicidal ideation were significantly related to higher glycosylated hemoglobin (HbA1c) in patients with T1D.40 Another variable with negative influence in the management of the disease and maintenance of glycemic levels was school infrastructure, which may not be able to assist these patients in some self-care actions. The lack of private places for insulin administration often leads to the need to apply it in inappropriate places, for example in the bathroom, which may inhibit self-care behaviors.41,42
One study showed that medications and supplies used to control or treat diseases such as T1D are usually stored in a separate room and require permission to use them. This system was perceived and demonstrated to be a problem.41 Other studies have shown negative associations between T1D with bullying and self-care behavior.41,43,44 This suggests not only problems of bullying in this population, but also to possible losses to glycemic control.
There were some limitations in the course of the study. Among them, the scarcity of studies on the subject matter is highlighted, which hindered the theoretical basis and comparison with other realities; nonetheless, the analyzed articles were generally of good methodological quality according to the criteria used.
Different instruments were used to assess bullying and social support. The questionnaire created by Olweus45 has been used in a series of investigations on bullying and has been adapted and translated by several authors. The relative merits of self-reported versus other types of assessments, such as a peer's and/or a teacher's perception, have been discussed in the evaluation in bullying.45–47
The scales used in the studies measured victimization, types of bullying, and types of aggressors. They also measured the perception of the different modes of support including emotional, care, and information, and showing the physical and verbal types of abuse as types of bullying that occur in high frequencies in boys and girls.48 However, due to heterogeneity of instruments and research methods, a single score would not be appropriate to asses all methodological approaches used in the articles, hindering comparisons.
The studies were carried out only in developed countries, thus indicating a need for studies in developing countries. No study estimated the incidence of bullying among young people with diabetes, as cross-sectional studies predominated. Therefore, it is necessary to carry out longitudinal studies in order to identify a cause and effect relationship between bullying and insufficient disease management.
Despite these limitations, this systematic review provides current data on bullying and its relation to T1D in children and adolescents and offers ideas for projects that can promote health and prevent aggression to those with T1D. It also reveals a lack of studies on bullying and its influence on the health-disease process of young diabetics in Brazil, suggesting the need for the development of more studies in other countries with standardized methods that would allow for better comparisons. These findings are important for public health, considering the repercussion of bullying in the learning environment and in the management of chronic diseases such as T1D.
ConclusionMost of the studies included in the present review demonstrated the occurrence of bullying in patients with T1D and greater victimization of these individuals in comparison with children and adolescents with other chronic diseases or with healthy peers. The physical and/or verbal forms of aggression were the most frequent threats/actions. Possible explanations for the occurrence of bullying in patients with T1D start with self-care, where activities are performed at various times as part of the daily routine of these young people, which are uncommon and can make them seem different from their peers, leading to victimization. Therefore, knowledge of this relationship is fundamental for the follow-up of these patients and the implementation of preventive programs.
FundingThis study was partially funded by a grant of the Bahia State Research Support Foundation (FAPESB).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Andrade CJ, Alves CA. Relationship between bullying and type 1 diabetes mellitus in children and adolescents: a systematic review. J Pediatr (Rio J). 2019;95:509–18.





