
Determine the prevalence of medication use in children and adolescents in 20 municipalities of Vale do Jequitinhonha, Minas Gerais-Brazil, showing the main groups and variables that may have influenced use.
MethodsDescriptive population-based survey sample of 555 interviews, selected by simple random cluster sampling of 137 census tracts. Inclusion criteria were age ≤ 14 years, mandatory interview with the legal guardians, and regardless of having received medications. Regarding the usage pattern, participants were divided into two groups: consumption and non-consumption of drugs. A descriptive analysis of the variables and tests of association were performed.
ResultsThe prevalence of drug consumption was 56.57%, and 42.43% showed no consumption. The use of medicinal plants was 72.9% for drug users and 74.3% for non-users. The health conditions for consumption were cough, common cold, flu, nasal congestion or bronchospasm (49.7%), fever (5.4%), headache (5.4%), diarrhea, indigestion, and abdominal colic (6.7%). In cases of self-medication, 30.57% of the drugs were given by the mother, and 69.42% were prescription drugs. Self-medication was prevalent using paracetamol (30.2%), dipyrone (20.8%), and cold medicine (18.8%). There was increased use of analgesics/antipyretics, followed by respiratory medications, systemic antibiotics, histamine H1 antagonists, and vitamins/antianemics.
ConclusionsThe prevalence of drugs use in children was high, indicating the need for formulating educational programs aiming at the awareness of caregivers regarding rational use.
Determinar a prevalência do consumo de medicamento em crianças e adolescentes de 20 municípios do Vale do Jequitinhonha, Minas Gerais-Brasil, mostrando os principais grupos e variáveis que possam ter influenciado o uso.
MétodosEstudo descritivo tipo inquérito populacional domiciliar, amostra constituída por 555 entrevistas selecionadas de maneira aleatória simples por meio de amostragem por conglomerado de 137 setores censitários. Os critérios de inclusão foram idade ≤14 anos, entrevista obrigatória com os responsáveis legais, independente de terem consumido medicamento. Quanto ao padrão de uso os participantes foram divididos em dois grupos consomem e não consomem medicamentos. Realizada análise descritiva das variáveis e aplicados testes de associação.
ResultadosA prevalência de consumo de medicamentos foi 56,57% e o não consumo 42,43%. O uso de plantas medicinais foi de 72,9% para o consumo de medicamento e 74,3% para o não consumo. As situações de saúde para o consumo foram tosse, resfriado comum, gripe, congestão nasal ou broncospasmo (49,7%); febre (5,4%); cefaléia (5,4%); diarréia, “má digestão” e cólica abdominal (6,7%). Na automedicação, 30,57% dos medicamentos foram indicados pela mãe, e 69,42% de prescrições médicas. Destaca-se na automedicação o uso de paracetamol (30,2%), dipirona (20,8%) e antigripais (18,8%). E um maior uso de analgésicos/antipiréticos, seguido do aparelho respiratório, antibióticos sistêmicos, antagonistas H1da histamina e vitaminas/antianêmicos.
ConclusõesA prevalência do consumo de medicamentos na população infantil foi alta, indicando a necessidade de formulação de programas educativos visando principalmente à conscientização dos cuidadores sobre o uso racional.
The main users of health services in developing countries are children, and their pattern of illness is reflected in medication use.1 This use, in turn, can be excessive due to self-medication, a widespread practice in Brazil, induced by the media and performed without indication and medical prescription. In Brazil, approximately 80 million people practice self-medication, and the risk of this practice is correlated with the level of education and information about drugs, as well as the accessibility of medications in the health system.2
In this sense, some authors recommend special attention to the medications used by children, considering the reservations regarding their efficacy and safety caused by lack of clinical trials due to ethical, legal, and economic reasons, and limited knowledge about the effects of the medication on the body.3,4 In the case of children, the practice of medication use is based primarily on extrapolation and adaptations of the use in adults, on the information obtained from rare observational studies, and on expert consensuses.5
Although scarce in developing countries, population-based studies are required to evaluate the use of medications in children.6,7 A study conducted in Brazil demonstrated a prevalence of 56%, which indicates a high consumption by children, indicating a significant use of medications with indication and age restrictions, especially in children younger than 2 years.8 Considering these facts, it is advisable to establish a specific list of essential medications according to the needs of children, aiming to promote their rational use.9
In order to contribute to this area, a population-based epidemiological study was conducted in children aged 0-14 years living in urban areas of Vale do Jequitinhonha, located in the northern region of the state of Minas Gerais, Brazil. The objective was to identify the prevalence and pattern of medication use, with or without prescription, demonstrating the main groups and types of drugs used, as well as variables that may have influenced this use.
MethodsThis descriptive, exploratory, cross-sectional, population-based household-survey study was carried out from April 10 to July 20, 2013. Inclusion criteria were age ≤ 14 years old, mandatory interview with the legal guardians, regardless of having received medications. All guardians who were not present at the time of the interview or who refused to participate were excluded from the study, as well as when the selected household was a commercial property, or did not have residents aged ≤ 14 years.
After estimating a population proportion of 41.4% of self-medication in children,10 the number calculated for sample selection was estimated as 672 household interviews for the urban areas of each city (acceptable error of 5.0% for an infinite sample). To calculate this value, data from the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística - IBGE)11 census were used, showing a total of approximately 88,936 individuals aged ≤ 14 years in 20 municipalities of the Intermunicipal Healthcare Consortium of Alto Jequitinhonha, Diamantina, Minas Gerais, Brazil.
Regarding the Human Development Index (HDI) of the municipalities studied,18 five had an HDI between 0.558 and 0.582; 14, between 0.616-0.682, and one, 0.716, reflecting indicators of education, housing, health, work, income, and vulnerability.
Simple random cluster sampling was used to select households, using as reference unit 137 urban census sectors for a sample of 672 households defined by IBGE (2010).11 However, a greater number of sectors was chosen, estimating that the required minimum number of individuals would not be met, especially in central sectors (commercial properties) and in old neighborhoods with elderly residents. An IBGE map (2010) was printed for each selected sector,11 allowing the interviewer to find it in the field and walk around it, following a pre-established system for household selection.
Data were collected by four interviewers trained in a pilot study to validate the collection, using a structured open- and closed-question questionnaire. In households with more than one child, only one questionnaire was applied, after the individual was selected by drawing lots using a table of random numbers.
The dependent variable was medication use, and the participants were divided into two study groups: uses medication and does not use medication. Self-medication was defined as medication use due to lay advice, and medical prescription was defined as medication use motivated by medical consultation and prescription for the disease that originated use. The medications used were divided into groups and subgroups according to the latest version of the Anatomical Therapeutic Chemical (ATC) Classification of the World Health Organization (WHO).12 Two groups of variables, socioeconomic indicators and use of health care (public or private) services, were considered. The socioeconomic indicators considered in the study were the head of the family's occupation (employed or unemployed/retired); family income in minimum wages at the time of the interview; and the criteria of the Brazilian Association of Business and Research (Associação Brasileira de Empresas e Pesquisas - ABEP), considering a measure of potential and consumption habits.13
For data analysis, a descriptive analysis of the dependent variable and the explanatory variables was initially conducted, and association tests (chi-squared and Fisher's exact) were subsequently applied. Analyses were processed using the statistical software Epi-Info, release 7.0 (CDC/WHO, Atlanta, GE, USAs); and R, release 2.12.2 (CDC/WHO - Atlanta, United States).14
The study protocol was approved by the Research Ethics Committee of Universidade Federal dos Vales do Jequitinhonha e Mucuri (UFVJM; Opinion 044/11); the participant population was informed of the study purpose and signed the informed consent.
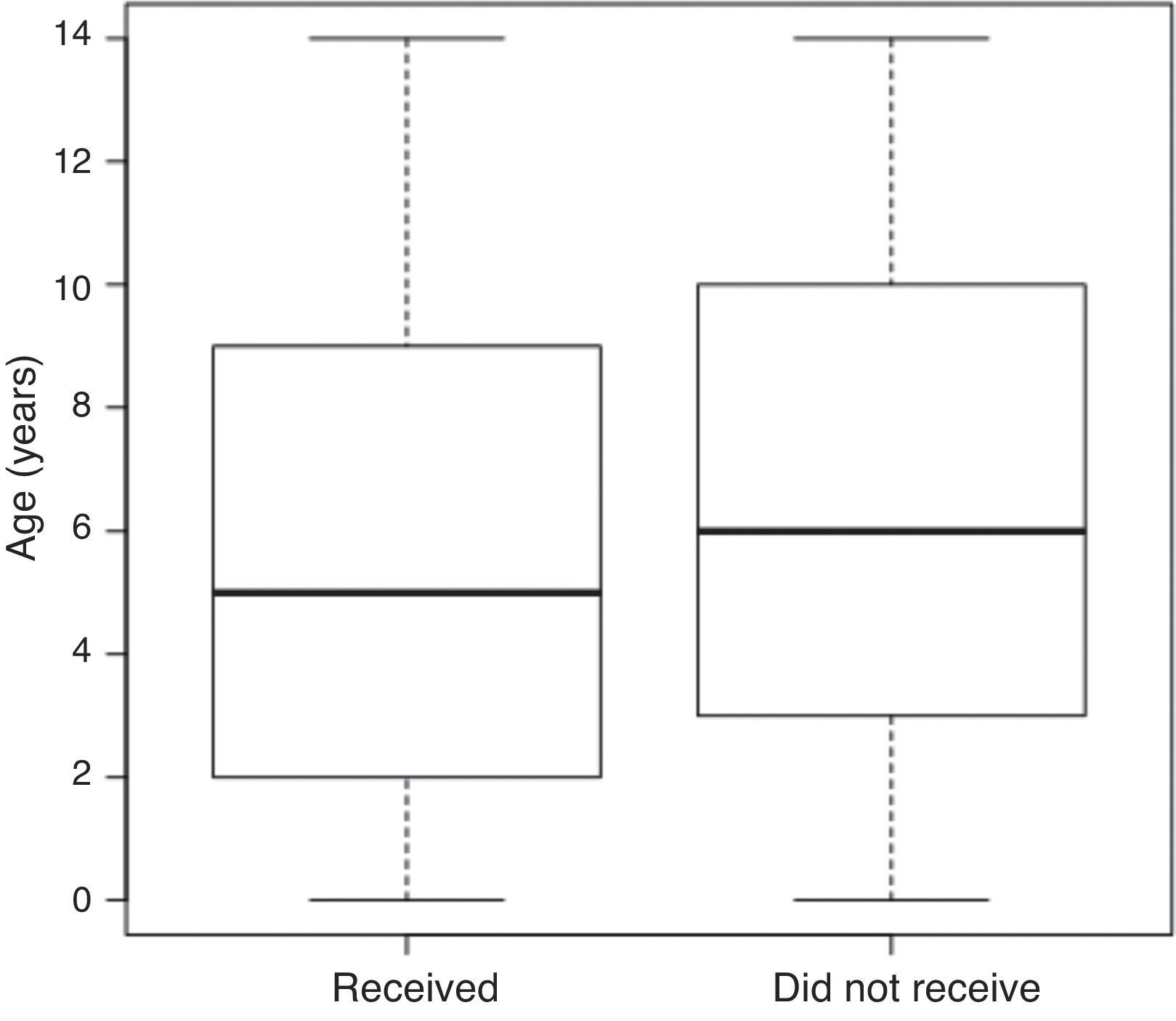
ResultsThe study included 672 individuals, of whom 117 (17.41%) were losses and refusals, resulting in 555 interviews. The validated interviews followed a similar pattern of distribution during the four-month study in 20 municipalities (138.5±34.6 interviews/week). The mean age of the individuals who used medications was 2-7 years (38.9%), and 7-14 years (43.9%) in those using medications according to medical prescription and self-medication (Fig. 1).
, Brazil, 2014. The data are shown without box-and-whisker plots; in each rectangle (box plot), the lower, intermediate, and upper horizontal lines represent the 1st quartile (25th percentile), median (50th percentile), and 3rd quartile (75th percentile), respectively. The lower and upper limits of the vertical lines represent the lowest and highest value, respectively. p=0.88 (Mann-Whitney U-test).")
Graphical representation of groups of children and adolescents who received medications on the 15 days prior to the household interview, according to age - Vale do Jequitinhonha Municipalities (MG), Brazil, 2014.
The data are shown without box-and-whisker plots; in each rectangle (box plot), the lower, intermediate, and upper horizontal lines represent the 1st quartile (25th percentile), median (50th percentile), and 3rd quartile (75th percentile), respectively. The lower and upper limits of the vertical lines represent the lowest and highest value, respectively. p=0.88 (Mann-Whitney U-test).
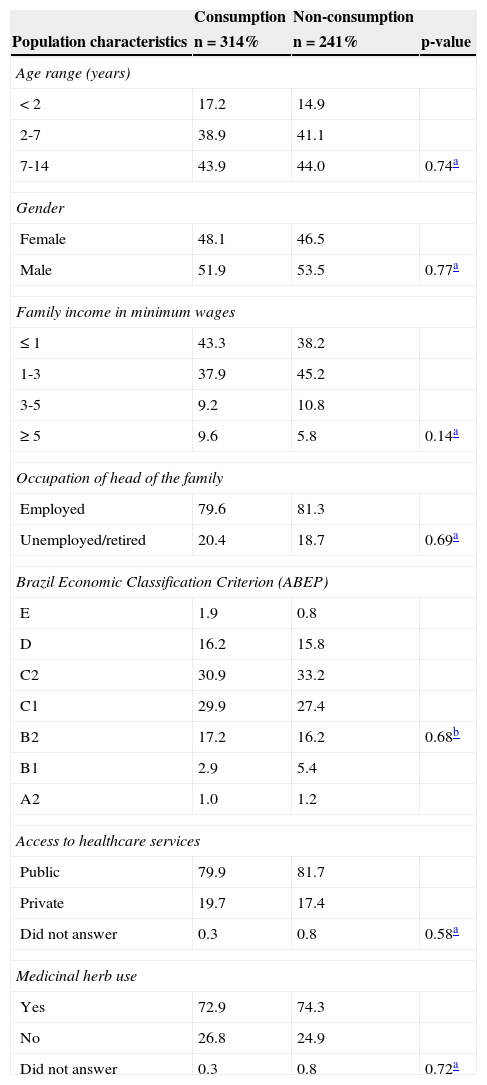
Considering the use of medications in the previous 15 days, the prevalence of use was 56.57%, with no statistically significant difference when comparing the 20 cities (chi-squared, p=0.5). Regarding the use of medicinal herbs and plants among children who used and did not use medications, it was 72.9% and 74.3%, respectively (Table 1).
Distribution of sociodemographic variables as well as of consumption and non-consumption of medications on the 15 days prior to the household interview – Vale do Jequitinhonha municipalities (MG), Brazil, 2014.
| Consumption | Non-consumption | ||
|---|---|---|---|
| Population characteristics | n=314% | n=241% | p-value |
| Age range (years) | |||
| <2 | 17.2 | 14.9 | |
| 2-7 | 38.9 | 41.1 | |
| 7-14 | 43.9 | 44.0 | 0.74a |
| Gender | |||
| Female | 48.1 | 46.5 | |
| Male | 51.9 | 53.5 | 0.77a |
| Family income in minimum wages | |||
| ≤ 1 | 43.3 | 38.2 | |
| 1-3 | 37.9 | 45.2 | |
| 3-5 | 9.2 | 10.8 | |
| ≥ 5 | 9.6 | 5.8 | 0.14a |
| Occupation of head of the family | |||
| Employed | 79.6 | 81.3 | |
| Unemployed/retired | 20.4 | 18.7 | 0.69a |
| Brazil Economic Classification Criterion (ABEP) | |||
| E | 1.9 | 0.8 | |
| D | 16.2 | 15.8 | |
| C2 | 30.9 | 33.2 | |
| C1 | 29.9 | 27.4 | |
| B2 | 17.2 | 16.2 | 0.68b |
| B1 | 2.9 | 5.4 | |
| A2 | 1.0 | 1.2 | |
| Access to healthcare services | |||
| Public | 79.9 | 81.7 | |
| Private | 19.7 | 17.4 | |
| Did not answer | 0.3 | 0.8 | 0.58a |
| Medicinal herb use | |||
| Yes | 72.9 | 74.3 | |
| No | 26.8 | 24.9 | |
| Did not answer | 0.3 | 0.8 | 0.72a |
ABEP, Associação Brasileira de Empresas de Pesquisas.
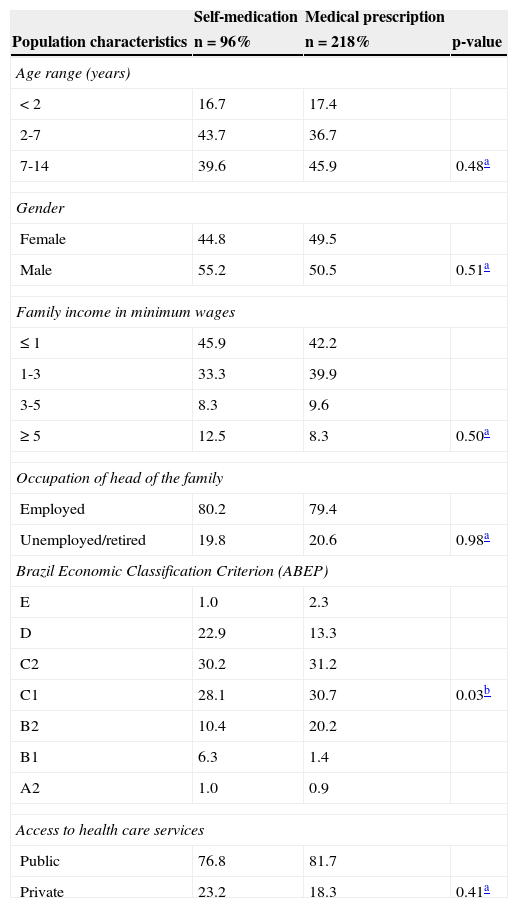
Most participants lived in brick houses (97.5%) and had sanitation facilities (92.9%), public water supply (99.5%), and public garbage collection service (99%). It was observed that the use of self-medication was not statistically significant (p<0.05) regarding age ranges, gender, family income, and access to healthcare services (Table 2).
Distribution of sociodemographic variables and of health care access, considering medication use through self-medication and prescription on the 15 days prior to the household interview - Vale do Jequitinhonha municipalities (MG), Brazil, 2014.
| Self-medication | Medical prescription | ||
|---|---|---|---|
| Population characteristics | n=96% | n=218% | p-value |
| Age range (years) | |||
| <2 | 16.7 | 17.4 | |
| 2-7 | 43.7 | 36.7 | |
| 7-14 | 39.6 | 45.9 | 0.48a |
| Gender | |||
| Female | 44.8 | 49.5 | |
| Male | 55.2 | 50.5 | 0.51a |
| Family income in minimum wages | |||
| ≤ 1 | 45.9 | 42.2 | |
| 1-3 | 33.3 | 39.9 | |
| 3-5 | 8.3 | 9.6 | |
| ≥ 5 | 12.5 | 8.3 | 0.50a |
| Occupation of head of the family | |||
| Employed | 80.2 | 79.4 | |
| Unemployed/retired | 19.8 | 20.6 | 0.98a |
| Brazil Economic Classification Criterion (ABEP) | |||
| E | 1.0 | 2.3 | |
| D | 22.9 | 13.3 | |
| C2 | 30.2 | 31.2 | |
| C1 | 28.1 | 30.7 | 0.03b |
| B2 | 10.4 | 20.2 | |
| B1 | 6.3 | 1.4 | |
| A2 | 1.0 | 0.9 | |
| Access to health care services | |||
| Public | 76.8 | 81.7 | |
| Private | 23.2 | 18.3 | 0.41a |
ABEP, Associação Brasileira de Empresas de Pesquisas.
The main health conditions that motivated medication use were cough, common cold, flu, nasal congestion, or bronchospasm (49.7%); fever (5.4%); headache (5.4%); and diarrhea, indigestion, and colic (6.7%). In self-medication, 30.57% of the medications were given by the mother, and 69.42% resulted from medical prescriptions.
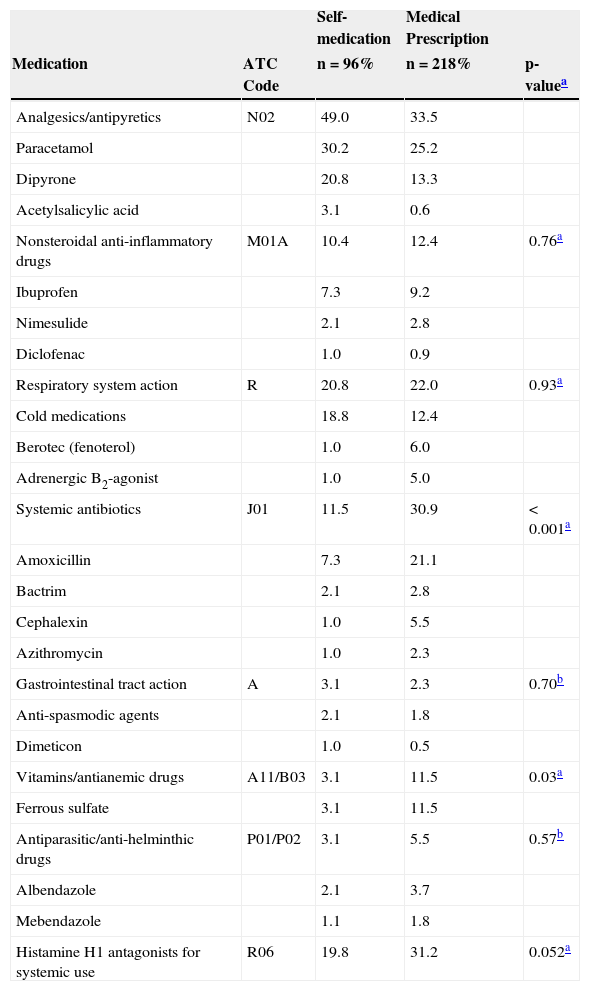
According to Table 3, the number of medications used was proportionally higher in the population that received prescription medications. Increased frequency of use was observed for analgesics/antipyretics, followed by respiratory system medications, systemic antibiotics, histamine H1 antagonists, and finally vitamins/antianemic drugs. The consumption of analgesics/antipyretics was higher among self-medication users, while the others were higher in cases of medical prescription. As for the drug's active agent, the authors highlight the high frequency of use of paracetamol (30.2%), dipyrone (20.8%), and cold medicine (18.8%) in self-medicated individuals; in those receiving drugs according to the medical prescription, prevalent drugs included histamine H1 antagonist (31.3%), amoxicillin (21.1%), ferrous sulfate (11.5%), and ibuprofen (9.2%) (Tables 1-3; Fig. 1).
Main medications found in home pharmacies, according to groups and subgroups of the Anatomical Therapeutic Chemical (ATC/WHO) classification and the patterns of use on the 15 days prior to the household interview - Vale do Jequitinhonha municipalities (MG), Brazil, 2014.
| Self-medication | Medical Prescription | |||
|---|---|---|---|---|
| Medication | ATC Code | n=96% | n=218% | p-valuea |
| Analgesics/antipyretics | N02 | 49.0 | 33.5 | |
| Paracetamol | 30.2 | 25.2 | ||
| Dipyrone | 20.8 | 13.3 | ||
| Acetylsalicylic acid | 3.1 | 0.6 | ||
| Nonsteroidal anti-inflammatory drugs | M01A | 10.4 | 12.4 | 0.76a |
| Ibuprofen | 7.3 | 9.2 | ||
| Nimesulide | 2.1 | 2.8 | ||
| Diclofenac | 1.0 | 0.9 | ||
| Respiratory system action | R | 20.8 | 22.0 | 0.93a |
| Cold medications | 18.8 | 12.4 | ||
| Berotec (fenoterol) | 1.0 | 6.0 | ||
| Adrenergic B2-agonist | 1.0 | 5.0 | ||
| Systemic antibiotics | J01 | 11.5 | 30.9 | <0.001a |
| Amoxicillin | 7.3 | 21.1 | ||
| Bactrim | 2.1 | 2.8 | ||
| Cephalexin | 1.0 | 5.5 | ||
| Azithromycin | 1.0 | 2.3 | ||
| Gastrointestinal tract action | A | 3.1 | 2.3 | 0.70b |
| Anti-spasmodic agents | 2.1 | 1.8 | ||
| Dimeticon | 1.0 | 0.5 | ||
| Vitamins/antianemic drugs | A11/B03 | 3.1 | 11.5 | 0.03a |
| Ferrous sulfate | 3.1 | 11.5 | ||
| Antiparasitic/anti-helminthic drugs | P01/P02 | 3.1 | 5.5 | 0.57b |
| Albendazole | 2.1 | 3.7 | ||
| Mebendazole | 1.1 | 1.8 | ||
| Histamine H1 antagonists for systemic use | R06 | 19.8 | 31.2 | 0.052a |
The prevalence of drug use in children up to 14 years of age estimated in this study was 56.57%, based on the mother's recall period of 15 days, similar to other Brazilian studies in which it ranged from 48% to 56%.6,8 Due to the heterogeneity of the methods used in other studies, it is difficult to compare the data, as the age group investigated and the recall period vary significantly, as well as the origin of the medication use.
While some studies have investigated the use of medications by medical prescription,3 others assessed their use in self-medication.7,15 Some characteristics of this study sample must be taken into account when comparing it with literature data, as the socioeconomic conditions are known determinants of medication consumption.16,17 Therefore, when interpreting these data, it must be considered that the studied population lives in a large geographical area in northern Minas Gerais, and is slightly economically heterogeneous, not including the more privileged strata of society regarding income, education, and access to healthcare services.
In the present study, variables related to sociodemographic of children and their parents/guardians were not associated with medication use and are probably associated with low family income, considered as a determinant of medication use:17 individuals with income ≤ three minimum wages consume 1.3 times more medication than those with income ≥ three minimum wages. Furthermore, the sample was restricted to the urban area of 20 municipalities with low HDI, whose household income was supplemented by the federal government income transfer program, and who are users of the public healthcare service network.18
As reported by the mothers, 69.42% of the medications used had been prescribed by physicians and 30.57% were given by the mothers at their own discretion. As previously demonstrated,19 there was a predominance of non-prescription medications administered to children by the mothers. This attitude has been attributed to social roles traditionally assigned to mothers, among them, to provide family health.
The ten most often administered medications comprised 77.16% of the total, with a predominance of analgesics/antipyretics, decongestants, iodine syrups, expectorants, and mucolytics. The commercialization of medications in Sweden is under strict control; however, in a study carried out in children, the ten most popular drugs constituted 70% of the total.20
Analgesics/antipyretics are often used in children, probably because fever is a common manifestation, as well as the trivialization of use of this class of medications due to unrestricted commercialization. Although medications such as paracetamol and dipyrone are analgesics and antipyretics of relatively safe use in children, considering appropriate doses, chronic and abusive use must be prevented.21
Paracetamol and ibuprofen are on the list of children's medications of the WHO.22 The safety of dipyrone, a low-cost analgesic/antipyretic and part of the list of medications subsidized by the federal government's Popular Pharmacy program, has been questioned in several parts of the world. Results of the Latinstudy, a multicenter case-control study conducted in seven locations in Brazil, two in Argentina, and one in Mexico, indicate a low incidence of aplastic anemia (1.6 cases per one million inhabitants/ year) and lack of association with dipyrone.23
Among medications acting on the respiratory tract, the most often used were antihistamines, cough medicines and expectorants, and nasal preparations. Several systematic reviews have shown that there is insufficient evidence that these medications show greater benefit than placebo in the treatment of symptoms caused by upper airway respiratory infections, such as nasal congestion and rhinorrhea associated with the common cold24 and acute cough.25
Although some of the medications used to treat the respiratory tract, such as dexchlorpheniramine and the association of phenylephrine-brompheniramine are contraindicated for children younger than two years, it was observed that approximately 17.18% of children using these medications were in this age group. 8,26,27 In addition to the intrinsic adverse effects of each active substance, there are other factors that can make them potentially dangerous for this age group, including the incorrect dose interpretation or dose interval, use of inappropriate dispensing measures, or the simultaneous administration of several medications, in order to achieve greater symptom relief.8,22
The authors also emphasize the significant use of nimesulide and diclofenac in children younger than 1 year, an age group for which the medication is contraindicated. The efficacy and safety of this drug for use in pediatric patients has yet to be established.8,27
In this study, the high percentage of medicinal herb and plant use (74.9%) is noteworthy, corresponding to 37.7% teas and 37% infusions. Even if the evidence of safety or effectiveness of complementary therapies is limited when compared to conventional therapies, such products are generally considered safe and/or natural by the parents, who administer them to their children with or without the doctor's awareness.28 The results of this study show the importance of a study to understand the psychological and sociocultural aspects that explain the reasons why parents feel encouraged to use these resources to ease the discomfort of their children.
Antibiotics are the second most often used medication subgroup in the investigated sample. In several studies,1,4 antibiotics appear in the list of the most common drugs used by children, especially those receiving prescribed medications.8 It is known that the main respiratory infections are responsible for a large proportion of outpatient antimicrobial prescriptions, demonstrating the intended use of antibiotics.29 Among the most studied antibiotics, amoxicillin was the most often used by children, and similar to results were found by other researchers.8 Amoxicillin is mentioned in international guidelines as first choice of treatment for the most common childhood infections, such as acute otitis media, sore throats, and sinusitis.1
All medications used for the treatment of children must be submitted to the licensing process to ensure the quality, safety, and efficacy in this age group. The four most commonly used medications in the sample (paracetamol, amoxicillin, ibuprofen, and dipyrone) have good documentation for pediatric use, although their indication is not recommended for some age ranges.8,26,27
Moreover, drugs used for the treatment of respiratory tract diseases show little evidence of efficacy, as mentioned previously. One of the most important factors to be considered in assessing the available evidence in pediatrics is how to deal with the ethical issues of child protection when performing controlled clinical trials. By definition, these always involve some degree of risk, which in pediatrics should be assumed by parents, based on potential benefits that will not be immediately available to their own children.
Despite the benefits that the pharmaceutical industry provides in drug development for adults, it is important to emphasize that economic motivation is not prominent for pediatric use.
The reduced drug market for the pediatric age range when compared to other ranges, such as adults and the elderly, in addition to the difficulties inherent to performing clinical trials in children, makes the development of these drugs unattractive to the pharmaceutical industry.30 However, as proposed by Coelho et al., the use of a specific list of essential drugs may be part of a comprehensive policy to stimulate the development and manufacturing of medicines for children in Brazil.9
Some limitations of the present study should be considered. The household survey is subject to biases from interviewers and interviewees, which are not always possible to control. The period in which data collection was conducted, April to July of 2013, coincided with the winter season in the region, when there is increased incidence of viral diseases and respiratory infections, which may have contributed to the higher consumption of certain drug classes, such as analgesics, antipyretics, antibiotics, antitussives, expectorants, mucolytics, and antiasthmatic drugs.26
In the present study, data collection standardization followed some procedures aimed at minimizing recall bias, including the 15-day recall period, to evaluate the use of medicines in children and request that the drug package and/or drug prescription be presented.
The prevalence found in this study corroborates the results of the literature, which indicate a high consumption of medication by children. It is also important to understand that medication use appears to be associated to low-income, as it is subsidized by the government.
Moreover, children aged 0 to 14 years, in general, are in a phase in life when health problems that require the use of medications should consider indication and age restrictions. The use of medications, in addition to being an indicator of health problems, also reflects social inequalities and deficiencies, quality of the healthcare system, regulations related to medications in the country, medical education, cultural habits, and the pharmaceutical market composition, among others factors.
The epidemiological reality of medication use should be considered by healthcare professionals and managers to create educational programs. In this sense, the nursing work process starts with drug prescription in primary care, and may involve studies of pharmacoepidemiology and pharmacovigilance in order to understand the consumption profile, resulting in knowledge that will allow interventions aimed at promoting rational use of medications.
FundingFundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMG-Process n. CDS-APQ-02522-11).
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank the interviewers (Alex, Lays, and Guilherme), the interviewed families, and Prof. Dr. Delba.
Please cite this article as: Cruz MJ, Dourado LF, Bodevan EC, Andrade RA, Santos DF. Medication use among children 0-14 years old: population baseline study. J Pediatr (Rio J). 2014;90:608–15.





