
To create and validate an instrument for child development monitoring.
MethodsMethodological study, based on the World Bank’s proposition to monitor child development indicators in low- and middle-income countries. The stages of the study included the following: development of an inventory of items for child development evaluation, based on open access instruments; content validation by a group of experts on the topic, using consensus techniques; selection of questions to describe children and their families; pre-test of the instrument during the vaccination campaign in 2016 in three municipalities, and conducting cognitive interviews.
ResultsA total of 431 items were sent for the evaluation of the specialists; 77 were initially excluded and the others were evaluated in-person by the group, with 162 items covering the motor, cognitive, language, and socio-emotional domains, distributed in ten age ranges. Questions about health, nutrition, early learning, protection and safety, and responsive care were also included. The instrument was applied by volunteer undergraduate students to 367 mothers of children under 5 years, showing good adherence of the caregivers. The time of application of the questionnaire was, on average, 20minutes. The cognitive interviews allowed the final adjustment of 19 items of the instrument for better understanding by the caregivers.
ConclusionsThe instrument created and validated by experts fills a gap, as it allows a comprehensive evaluation of the development of children under 5 years at the population level, using a fast and inexpensive tool, and can be useful for monitoring indicators of development in Brazilian children in vaccination campaigns.
Elaborar e validar um instrumento para o monitoramento de indicadores do desenvolvimento infantil.
MétodosEstudo metodológico baseado na proposta do Banco Mundial para medir indicadores do desenvolvimento infantil em países de baixa e média renda. As etapas do estudo contemplaram: elaboração de um inventário de itens para avaliação do desenvolvimento infantil, com base em instrumentos de livre acesso; validação de conteúdo por um grupo de especialistas no tema, com técnicas de consenso; seleção de questões para descrever as crianças e suas famílias; pré-teste do instrumento durante a campanha de vacinação de 2016 em três municípios e realização de entrevistas cognitivas.
ResultadosForam enviados 431 itens foram enviados para avaliação dos especialistas, 77 foram excluídos e os demais apreciados presencialmente pelo grupo. No fim foram selecionados 162 itens que abrangeram os domínios motor, cognitivo, de linguagem e socioemocional, distribuídos em 10 faixas etárias. Foram incluídas questões sobre saúde, nutrição, aprendizagem precoce, proteção e segurança e cuidado responsivo. O instrumento foi aplicado por universitários voluntários a 367 mães de crianças menores de cinco anos, mostrou boa adesão dos cuidadores. O tempo médio de aplicação do questionário foi 20 minutos. As entrevistas cognitivas permitiram ajustar 19 itens do instrumento para melhor compreensão dos cuidadores.
ConclusõesO instrumento construído e validado por especialistas preenche uma lacuna, que permite uma avaliação abrangente do desenvolvimento de crianças menores de cinco anos, em nível populacional, de forma rápida e barata, pode ser útil para o monitoramento de indicadores do desenvolvimento em campanhas de vacinação.
In the early years of a child’s life, the neural circuits of the brain are formed and strengthened through stimuli and bonding relationships, establishing the bases for development throughout life. The physical and emotional health, social skills, and cognitive-language skills that emerge at this stage are important prerequisites for success at school, in the workplace, and in the community.1 Nevertheless, it is estimated that over 250 million children worldwide are at risk of not reaching their full potential due to poverty or chronic malnutrition.2
The United Nations has included early childhood development, the period that comprises the first six full years of a child’s life, in the global political agenda, establishing an objective in the Sustainable Development Goals (SDGs) to ensure access to quality child development (CD) for all, and pointing out the need for interventions. Assessing a young child's skills is essential to understand the long-term impacts of such interventions and to support policies and practices. It can help generate information on the progress and challenges to meet the SDGs. Therefore, the availability of data on the development of children from 0 to 5 years of age is essential, especially in low- and middle-income countries, where disadvantaged children are concentrated.3
In Brazil, despite the recommendation of performing growth and CD surveillance,4 the Unified Health System (Sistema Único de Saúde [SUS]) information systems do not provide data on the development of the treated children and CD surveillance has not been a priority action by primary care teams.5
Consequently, research is an indispensable source for monitoring the situation of early childhood and for evaluating interventions aimed at promoting children’s integral development. However, in Brazil, population-based national surveys on child health do not include questions about CD and available studies representing locoregional realities were carried out in health services or day care centers and used different assessment tools, which makes comparability of results difficult on development problems.6–12
Following the worldwide trend, there is a growing interest in Brazil in promoting early childhood development,13 through the implementation of federal programs such as “Brasil Carinhoso” and, more recently, “Criança Feliz,” which until 2018 involved around 2000 municipalities, in addition to other state and local initiatives.14
In this scenario of strengthening the early childhood agenda and considering the scarcity of information for the formulation and evaluation of interventions in this area, the present study aimed at creating and validating an instrument for monitoring CD indicators.
MethodThis study, originated from the project “Early Childhood for Healthy Adults” (Primeira Infância para Adultos Saudáveis [PIPAS]), is methodological and was developed from a World Bank publication on a set of instruments for measuring CD in low- and middle-income countries. According to the proposed classification, the Child Development Assessment Questionnaire (QAD-PIPAS) was created based on measures of child behavior, obtained from the main caregivers’ reports and with the purpose of performing population monitoring.3 The aim of the questionnaire is to quickly and inexpensively evaluate the development of children aged 0–59 months who are seen during multi-vaccination campaigns, to provide information to local decision-makers, according to the strategy already adopted in Brazil to monitor infant feeding practices.15 The proposal is to apply the questionnaire through sampling, with the following exclusion criteria: children out of the assessed age range and those not accompanied by the main caregivers.
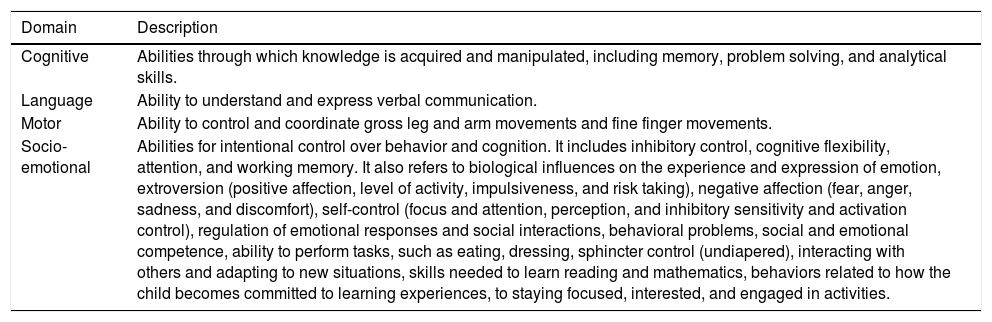
In order to obtain a comprehensive instrument, four CD domains were considered: motor (MD), cognitive (CoD), language (LD), and socio-affective (SD) domains. The definitions are shown in Table 1. These definitions guided the stages of item selection and content validation, which are described below.
Description of the child development domains covered in the study.
| Domain | Description |
|---|---|
| Cognitive | Abilities through which knowledge is acquired and manipulated, including memory, problem solving, and analytical skills. |
| Language | Ability to understand and express verbal communication. |
| Motor | Ability to control and coordinate gross leg and arm movements and fine finger movements. |
| Socio-emotional | Abilities for intentional control over behavior and cognition. It includes inhibitory control, cognitive flexibility, attention, and working memory. It also refers to biological influences on the experience and expression of emotion, extroversion (positive affection, level of activity, impulsiveness, and risk taking), negative affection (fear, anger, sadness, and discomfort), self-control (focus and attention, perception, and inhibitory sensitivity and activation control), regulation of emotional responses and social interactions, behavioral problems, social and emotional competence, ability to perform tasks, such as eating, dressing, sphincter control (undiapered), interacting with others and adapting to new situations, skills needed to learn reading and mathematics, behaviors related to how the child becomes committed to learning experiences, to staying focused, interested, and engaged in activities. |
A search was carried out in the literature for open access tests on CD evaluation used in national research and covering the domains of development of interest. The instruments selected were: a) the Child Health Handbook16; b) the Manual for Child Development Surveillance in the context of Integrated Management of Childhood Illness (IMCI)17; c) the Clinical Risk Indicators in Child Development (CDRI);9 d)the Modified Checklist for Autism in Toddlers (M−CHAT)18; e) the Survey of Well Being of Young Children (SWYC)19; and f) the Multiple Indicator Cluster Surveys: Cognitive Stimulation (MICS).20 Based on these instruments, an inventory was made of items that were grouped by domains and age range: 0 to 12 months; 13–15 months; 16–18 months; 19–24 months; 25–30 months; 31–36 months; 37–48 months; and 49–59 months.
Stage 2: content validityContent validity refers to the adequacy of an instrument’s content regarding the number and scope of the individual questions it contains. It uses the conceptual definition of the constructs being evaluated and consists of revising the instrument to ensure that it is sensible and that it addresses all relevant issues. Thus, content validation involves a critical examination of the basic structure of the instrument, a review of the procedures used to develop the questionnaire, and the consideration of its applicability to the intended research question.3
To validate the QAD-PIPAS, a multidisciplinary group was created, consisting of ten consultants (six pediatricians, one nurse, one occupational therapist, and one statistician), of whom seven were PhDs (three in child and adolescent health and the others in health sciences, medicine, nutrition, and public health), two specialists (neuropediatrics and developmental neurology), and two managers, one from the Ministry of Health and the other from the state health secretariat. The consultants were selected because they had experience in research, clinical practice, or policy formulation on the subject; their work included two phases:
- •
Analysis and score attribution for all items: using the Delphi method,21 an online form was organized by domains and age ranges to be answered by the experts. Each question was judged by two criteria – its relevance to assessing the domain in the child's age range and its viability, considering how easy it was for the caregiver to answer the question, with scores ranging from 0 to 5. The scores were entered into an Excel (Excel®, Microsoft, WA, USA) spreadsheet and then averaged by the experts for each item. Then, the items were categorized as follows: questions indicated for inclusion in the instrument, when they reached an average ≥ 4.25 in the two evaluated criteria (relevance and viability); questions indicated for exclusion, when the average was < 4 in both criteria; and dubious questions, when the average of the items was in the range ≥4 to < 4.25 in one of the criteria.
- •
Consideration and consensus on pending questions: the experts participated in a face-to-face panel to discuss the included and dubious questions until they reached a consensus on whether or not they should remain in the questionnaire. The discussion also addressed whether the questions were sufficient to assess CD and appropriate to the domain and age range. The analysis was based on the assumption that the instrument should be simple, fast to apply, and include milestones of the four domains for each age range.
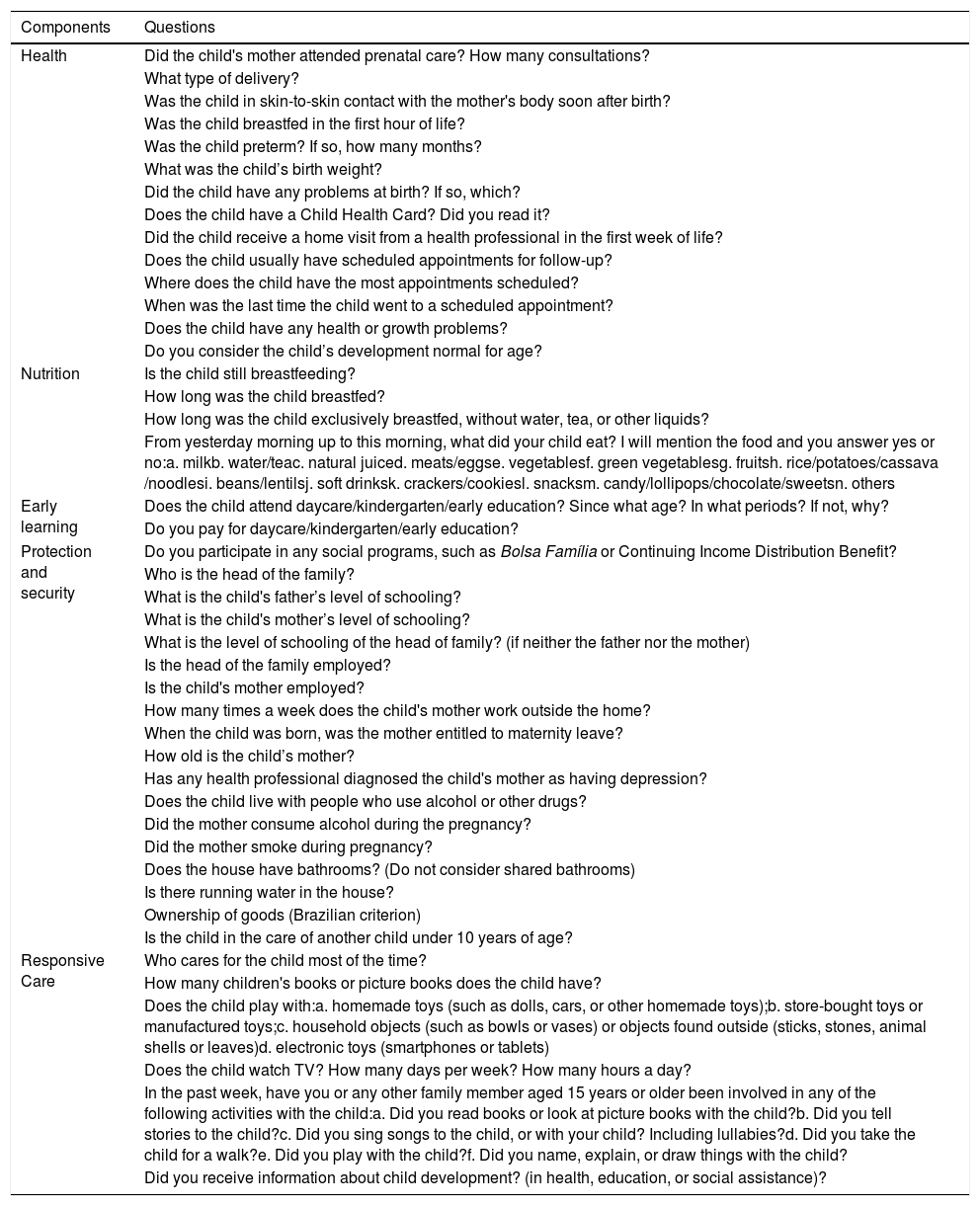
Questions about the profile of the children and their families that could potentially influence CD were included, considering that it is also recommended to monitor the quality and amount of care that the child experiences in their environment to help interpret the scores regarding their development.3 The definition of these questions was based on the theoretical model that proposes that care and attention aimed at full CD include health, nutrition, learning, social protection and safety, and responsive care components, as proposed by the World Health Organization.22
Stage 4: instrument pretestA pre-test of the instrument was performed during the 2016 vaccination campaign to assess caregivers' acceptance, degree of difficulty in understanding the questions, timing, and adequacy of the questionnaire for application in the intended context. The collection took place in two vaccination units in the municipalities of Embu das Artes, state of São Paulo (SP), and Brasília, Federal District, (FD) and in six units in the municipality of Recife, state of Pernambuco (PE), involving local managers and interviewers.
Stage 5: cognitive interviewsThe last step in the instrument creation consisted of cognitive interviews23 to assess the caregivers' understanding of the instrument's questions. The interviews took place in a Basic Health Unit of Embu das Artes, SP, with 36 caregivers of children aged from 0 to 5 years, with at least three from each age range.
The study was approved by the Research Ethics Committee of the Instituto de Saúde under CAAE number 55261616.5.0000.5469.
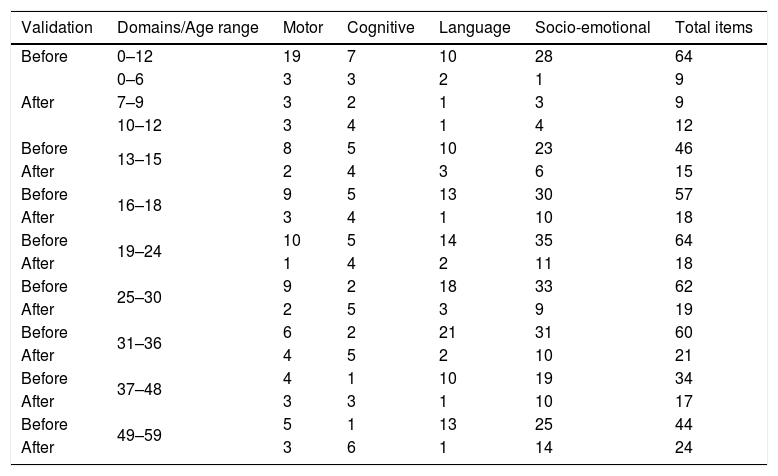
ResultsStage 1: inventory of items for CD assessmentA total of 431 CD assessment items obtained from the selected instruments were submitted to evaluation by the consultant group. Table 2 shows the inventory of items grouped by domains and age range.
Distribution of assessment items according to age range and child development domain, before and after the validation process.
| Validation | Domains/Age range | Motor | Cognitive | Language | Socio-emotional | Total items |
|---|---|---|---|---|---|---|
| Before | 0–12 | 19 | 7 | 10 | 28 | 64 |
| After | 0–6 | 3 | 3 | 2 | 1 | 9 |
| 7–9 | 3 | 2 | 1 | 3 | 9 | |
| 10–12 | 3 | 4 | 1 | 4 | 12 | |
| Before | 13–15 | 8 | 5 | 10 | 23 | 46 |
| After | 2 | 4 | 3 | 6 | 15 | |
| Before | 16–18 | 9 | 5 | 13 | 30 | 57 |
| After | 3 | 4 | 1 | 10 | 18 | |
| Before | 19–24 | 10 | 5 | 14 | 35 | 64 |
| After | 1 | 4 | 2 | 11 | 18 | |
| Before | 25–30 | 9 | 2 | 18 | 33 | 62 |
| After | 2 | 5 | 3 | 9 | 19 | |
| Before | 31–36 | 6 | 2 | 21 | 31 | 60 |
| After | 4 | 5 | 2 | 10 | 21 | |
| Before | 37–48 | 4 | 1 | 10 | 19 | 34 |
| After | 3 | 3 | 1 | 10 | 17 | |
| Before | 49–59 | 5 | 1 | 13 | 25 | 44 |
| After | 3 | 6 | 1 | 14 | 24 |
The experts’ assessment indicated the need to redefine the age range from 0 to 12 months, subdividing it into three periods: 0–6 full months, 7–9 full months, and 10–12 full months. Of the total of 431 evaluated items, 77 were initially excluded and the others were considered by the group in-person; at the end, 162 items were selected. Table 2 shows the selected items by domain and age range.
The application of the QAD-PIPAS allows the creation of a score for each assessed child, in which for each response adequate to the age group, the score of 1 is assigned, and then the points obtained by the child are tallied. Subsequently, the score is standardized by calculating the proportion of adequate responses in relation to the total of items evaluated in the age range. This standardized score ranges from 0 to 1, with “0” expressing non-adequate responses in all items evaluated and “1” representing adequate responses in all items. As this is an instrument aimed at obtaining population indicators, the results are analyzed according to the Z-score distribution.
Stage 3: selection of questions about the profile of the children and their familiesTable 3 shows questions representative of the health, nutrition, early learning, protection and safety, and responsive care dimensions.
Questions related to the components of the “Nutring Care” model and child development care.
| Components | Questions |
|---|---|
| Health | Did the child's mother attended prenatal care? How many consultations? |
| What type of delivery? | |
| Was the child in skin-to-skin contact with the mother's body soon after birth? | |
| Was the child breastfed in the first hour of life? | |
| Was the child preterm? If so, how many months? | |
| What was the child’s birth weight? | |
| Did the child have any problems at birth? If so, which? | |
| Does the child have a Child Health Card? Did you read it? | |
| Did the child receive a home visit from a health professional in the first week of life? | |
| Does the child usually have scheduled appointments for follow-up? | |
| Where does the child have the most appointments scheduled? | |
| When was the last time the child went to a scheduled appointment? | |
| Does the child have any health or growth problems? | |
| Do you consider the child’s development normal for age? | |
| Nutrition | Is the child still breastfeeding? |
| How long was the child breastfed? | |
| How long was the child exclusively breastfed, without water, tea, or other liquids? | |
| From yesterday morning up to this morning, what did your child eat? I will mention the food and you answer yes or no:a. milkb. water/teac. natural juiced. meats/eggse. vegetablesf. green vegetablesg. fruitsh. rice/potatoes/cassava /noodlesi. beans/lentilsj. soft drinksk. crackers/cookiesl. snacksm. candy/lollipops/chocolate/sweetsn. others | |
| Early learning | Does the child attend daycare/kindergarten/early education? Since what age? In what periods? If not, why? |
| Do you pay for daycare/kindergarten/early education? | |
| Protection and security | Do you participate in any social programs, such as Bolsa Família or Continuing Income Distribution Benefit? |
| Who is the head of the family? | |
| What is the child's father’s level of schooling? | |
| What is the child's mother’s level of schooling? | |
| What is the level of schooling of the head of family? (if neither the father nor the mother) | |
| Is the head of the family employed? | |
| Is the child's mother employed? | |
| How many times a week does the child's mother work outside the home? | |
| When the child was born, was the mother entitled to maternity leave? | |
| How old is the child’s mother? | |
| Has any health professional diagnosed the child's mother as having depression? | |
| Does the child live with people who use alcohol or other drugs? | |
| Did the mother consume alcohol during the pregnancy? | |
| Did the mother smoke during pregnancy? | |
| Does the house have bathrooms? (Do not consider shared bathrooms) | |
| Is there running water in the house? | |
| Ownership of goods (Brazilian criterion) | |
| Is the child in the care of another child under 10 years of age? | |
| Responsive Care | Who cares for the child most of the time? |
| How many children's books or picture books does the child have? | |
| Does the child play with:a. homemade toys (such as dolls, cars, or other homemade toys);b. store-bought toys or manufactured toys;c. household objects (such as bowls or vases) or objects found outside (sticks, stones, animal shells or leaves)d. electronic toys (smartphones or tablets) | |
| Does the child watch TV? How many days per week? How many hours a day? | |
| In the past week, have you or any other family member aged 15 years or older been involved in any of the following activities with the child:a. Did you read books or look at picture books with the child?b. Did you tell stories to the child?c. Did you sing songs to the child, or with your child? Including lullabies?d. Did you take the child for a walk?e. Did you play with the child?f. Did you name, explain, or draw things with the child? | |
| Did you receive information about child development? (in health, education, or social assistance)? |
The instrument was applied to 367 mothers of children under 5 years old in the cities of Recife, Brasilia, and Embu das Artes, with the purpose of testing it in different contexts. Overall, the professionals involved in the campaign accepted the research well and understood that the questionnaire application by external interviewers did not interfere with the routine of the vaccination staff. There was good adherence of mothers to the interviews, with approximately 10 % refusal to participate. The dissatisfaction of parents and other caregivers who could not answer the questionnaire was observed, which motivated the decision to include them as respondents.
The duration of the questionnaire application was, on average, 20min, which was considered viable for its application during vaccination campaigns. This information made it possible to estimate the number of interviewers needed to perform data collection at other times. The need to conduct cognitive interviews (Phase 5) to clarify the level of understanding of some questions was identified, as well as the need to redefine the initial age ranges, due to the low participation of children under 6 months in the campaign. This phase also supported the creation of a set of forms (Sampling Worksheet, Refusal Worksheet, and Free and Informed Consent Form) to support the survey during vaccination campaigns.
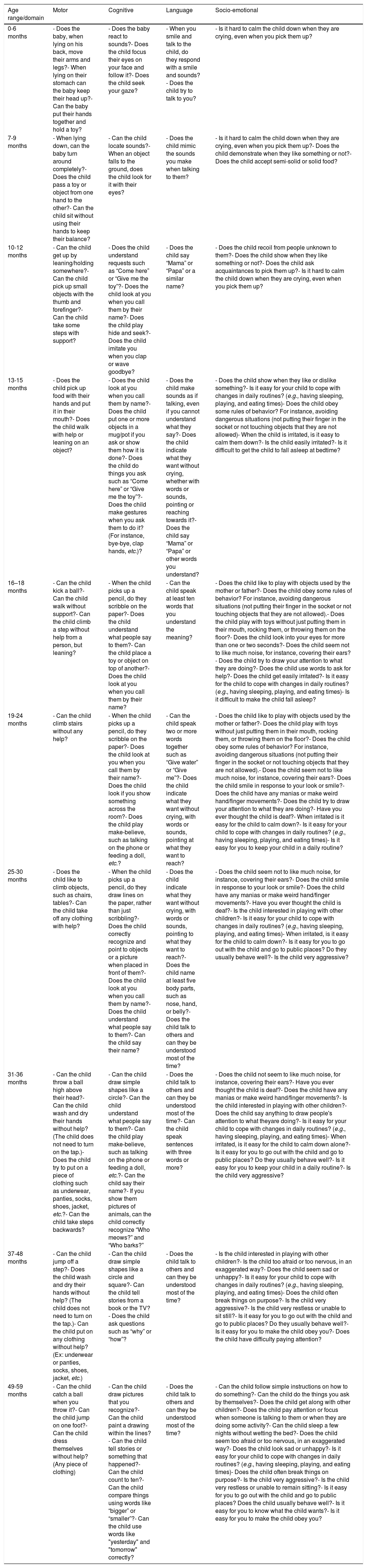
Stage 5: cognitive interviewsThe cognitive interviews showed the need for adjustments in 19 items of the instrument for better understanding by the caregivers, which were subsequently submitted to a specialist’s review. The final configuration of the instrument is shown in Table 4.
Questions related to the four domains of child development according to age range.
| Age range/domain | Motor | Cognitive | Language | Socio-emotional |
|---|---|---|---|---|
| 0-6 months | - Does the baby, when lying on his back, move their arms and legs?- When lying on their stomach can the baby keep their head up?- Can the baby put their hands together and hold a toy? | - Does the baby react to sounds?- Does the child focus their eyes on your face and follow it?- Does the child seek your gaze? | - When you smile and talk to the child, do they respond with a smile and sounds?- Does the child try to talk to you? | - Is it hard to calm the child down when they are crying, even when you pick them up? |
| 7-9 months | - When lying down, can the baby turn around completely?- Does the child pass a toy or object from one hand to the other?- Can the child sit without using their hands to keep their balance? | - Can the child locate sounds?- When an object falls to the ground, does the child look for it with their eyes? | - Does the child mimic the sounds you make when talking to them? | - Is it hard to calm the child down when they are crying, even when you pick them up?- Does the child demonstrate when they like something or not?- Does the child accept semi-solid or solid food? |
| 10-12 months | - Can the child get up by leaning/holding somewhere?- Can the child pick up small objects with the thumb and forefinger?- Can the child take some steps with support? | - Does the child understand requests such as “Come here” or “Give me the toy”?- Does the child look at you when you call them by their name?- Does the child play hide and seek?- Does the child imitate you when you clap or wave goodbye? | - Does the child say “Mama” or “Papa” or a similar name? | - Does the child recoil from people unknown to them?- Does the child show when they like something or not?- Does the child ask acquaintances to pick them up?- Is it hard to calm the child down when they are crying, even when you pick them up? |
| 13-15 months | - Does the child pick up food with their hands and put it in their mouth?- Does the child walk with help or leaning on an object? | - Does the child look at you when you call them by name?- Does the child put one or more objects in a mug/pot if you ask or show them how it is done?- Does the child do things you ask such as “Come here” or “Give me the toy”?- Does the child make gestures when you ask them to do it? (For instance, bye-bye, clap hands, etc.)? | - Does the child make sounds as if talking, even if you cannot understand what they say?- Does the child indicate what they want without crying, whether with words or sounds, pointing or reaching towards it?- Does the child say “Mama” or “Papa” or other words you understand? | - Does the child show when they like or dislike something?- Is it easy for your child to cope with changes in daily routines? (e.g., having sleeping, playing, and eating times)- Does the child obey some rules of behavior? For instance, avoiding dangerous situations (not putting their finger in the socket or not touching objects that they are not allowed)- When the child is irritated, is it easy to calm them down?- Is the child easily irritated?- Is it difficult to get the child to fall asleep at bedtime? |
| 16–18 months | - Can the child kick a ball?- Can the child walk without support?- Can the child climb a step without help from a person, but leaning? | - When the child picks up a pencil, do they scribble on the paper?- Does the child understand what people say to them?- Can the child place a toy or object on top of another?- Does the child look at you when you call them by their name? | - Can the child speak at least ten words that you understand the meaning? | - Does the child like to play with objects used by the mother or father?- Does the child obey some rules of behavior? For instance, avoiding dangerous situations (not putting their finger in the socket or not touching objects that they are not allowed).- Does the child play with toys without just putting them in their mouth, rocking them, or throwing them on the floor?- Does the child look into your eyes for more than one or two seconds?- Does the child seem not to like much noise, for instance, covering their ears?- Does the child try to draw your attention to what they are doing?- Does the child use words to ask for help?- Does the child get easily irritated?- Is it easy for the child to cope with changes in daily routines? (e.g., having sleeping, playing, and eating times)- Is it difficult to make the child fall asleep? |
| 19-24 months | - Can the child climb stairs without any help? | - When the child picks up a pencil, do they scribble on the paper?- Does the child look at you when you call them by their name?- Does the child look if you show something across the room?- Does the child play make-believe, such as talking on the phone or feeding a doll, etc.? | - Can the child speak two or more words together such as “Give water” or “Give me”?- Does the child indicate what they want without crying, with words or sounds, pointing at what they want to reach? | - Does the child like to play with objects used by the mother or father?- Does the child play with toys without just putting them in their mouth, rocking them, or throwing them on the floor?- Does the child obey some rules of behavior? For instance, avoiding dangerous situations (not putting their finger in the socket or not touching objects that they are not allowed).- Does the child seem not to like much noise, for instance, covering their ears?- Does the child smile in response to your look or smile?- Does the child have any manias or make weird hand/finger movements?- Does the child try to draw your attention to what they are doing?- Have you ever thought the child is deaf?- When irritated is it easy for the child to calm down?- Is it easy for your child to cope with changes in daily routines? (e.g., having sleeping, playing, and eating times)- Is it easy for you to keep your child in a daily routine? |
| 25-30 months | - Does the child like to climb objects, such as chairs, tables?- Can the child take off any clothing with help? | - When the child picks up a pencil, do they draw lines on the paper, rather than just scribbling?- Does the child correctly recognize and point to objects or a picture when placed in front of them?- Does the child look at you when you call them by name?- Does the child understand what people say to them?- Can the child say their name? | - Does the child indicate what they want without crying, with words or sounds, pointing to what they want to reach?- Does the child name at least five body parts, such as nose, hand, or belly?- Does the child talk to others and can they be understood most of the time? | - Does the child seem not to like much noise, for instance, covering their ears?- Does the child smile in response to your look or smile?- Does the child have any manias or make weird hand/finger movements?- Have you ever thought the child is deaf?- Is the child interested in playing with other children?- Is it easy for your child to cope with changes in daily routines? (e.g., having sleeping, playing, and eating times)- When irritated, is it easy for the child to calm down?- Is it easy for you to go out with the child and go to public places? Do they usually behave well?- Is the child very aggressive? |
| 31-36 months | - Can the child throw a ball high above their head?- Can the child wash and dry their hands without help? (The child does not need to turn on the tap.)- Does the child try to put on a piece of clothing such as underwear, panties, socks, shoes, jacket, etc.?- Can the child take steps backwards? | - Can the child draw simple shapes like a circle?- Can the child understand what people say to them?- Can the child play make-believe, such as talking on the phone or feeding a doll, etc.?- Can the child say their name?- If you show them pictures of animals, can the child correctly recognize “Who meows?” and “Who barks?” | - Does the child talk to others and can they be understood most of the time?- Can the child speak sentences with three words or more? | - Does the child not seem to like much noise, for instance, covering their ears?- Have you ever thought the child is deaf?- Does the child have any manias or make weird hand/finger movements?- Is the child interested in playing with other children?- Does the child say anything to draw people's attention to what theyare doing?- Is it easy for your child to cope with changes in daily routines? (e.g., having sleeping, playing, and eating times)- When irritated, is it easy for the child to calm down alone?- Is it easy for you to go out with the child and go to public places? Do they usually behave well?- Is it easy for you to keep your child in a daily routine?- Is the child very aggressive? |
| 37-48 months | - Can the child jump off a step?- Does the child wash and dry their hands without help? (The child does not need to turn on the tap.)- Can the child put on any clothing without help? (Ex: underwear or panties, socks, shoes, jacket, etc.) | - Can the child draw simple shapes like a circle and square?- Can the child tell stories from a book or the TV?- Does the child ask questions such as “why” or “how”? | - Does the child talk to others and can they be understood most of the time? | - Is the child interested in playing with other children?- Is the child too afraid or too nervous, in an exaggerated way?- Does the child seem sad or unhappy?- Is it easy for your child to cope with changes in daily routines? (e.g., having sleeping, playing, and eating times)- Does the child often break things on purpose?- Is the child very aggressive?- Is the child very restless or unable to sit still?- Is it easy for you to go out with the child and go to public places? Do they usually behave well?- Is it easy for you to make the child obey you?- Does the child have difficulty paying attention? |
| 49-59 months | - Can the child catch a ball when you throw it?- Can the child jump on one foot?- Can the child dress themselves without help? (Any piece of clothing) | - Can the child draw pictures that you recognize?- Can the child paint a drawing within the lines?- Can the child tell stories or something that happened?- Can the child count to ten?- Can the child compare things using words like “bigger” or “smaller”?- Can the child use words like "yesterday" and "tomorrow" correctly? | - Does the child talk to others and can they be understood most of the time? | - Can the child follow simple instructions on how to do something?- Can the child do the things you ask by themselves?- Does the child get along with other children?- Does the child pay attention or focus when someone is talking to them or when they are doing some activity?- Can the child sleep a few nights without wetting the bed?- Does the child seem too afraid or too nervous, in an exaggerated way?- Does the child look sad or unhappy?- Is it easy for your child to cope with changes in daily routines? (e.g., having sleeping, playing, and eating times)- Does the child often break things on purpose?- Is the child very aggressive?- Is the child very restless or unable to remain sitting?- Is it easy for you to go out with the child and go to public places? Does the child usually behave well?- Is it easy for you to know what the child wants?- Is it easy for you to make the child obey you? |
The methodological trajectory allowed the creation of the first Brazilian instrument for the monitoring of CD indicators of children aged from 0 to 5 years at the population level and to carry out the primary stage of content validation, which will be followed by the reliability, concurrent, and discriminatory validation steps, in a study being conducted by the same research team. The participation of specialists working in research and clinical practice was crucial to address issues that reflected the expected behavior of children at different age ranges and in the cognitive, language, motor, and socio-emotional domains, especially the latter, which is generally neglected in the assessment and early guidance provided to caregivers. The adequacy of the instrument for application during vaccination campaigns suggests the feasibility and usefulness of the QAD-PIPAS.
One limitation of the instrument is that it is not possible to identify CD problems in specific domains, considering the limited number of questions that assess each domain, given the need for the rapid application of interviews during the vaccination campaigns. Although this strategy makes it possible to obtain information within a short period of time, operational issues deserve attention, such as the need to recruit interviewers not working in the campaign, so that the research does not interfere with vaccination activities.
The interest in the creation and validation of tests in different parts of the world is related to the influence of the sociocultural context of CD. Cultures attribute different values for the skills that children should develop and display, which may emerge earlier if they are praised and encouraged.3
In 2009, the World Bank reviewed 41 instruments used to assess CD in low- and middle-income countries, and in 2017 this review was updated to include 106 new instruments for children aged 0–8 years.3
In response to the emphasis placed on CD by the United Nations and its inclusion in the SDGs, several efforts are underway to create and validate universal measures to track the developmental status of children aged 0–6 years. However, to date, there is no globally accepted instrument used to assess the development of children in early childhood.
While global instruments that have been validated in different populations, including Brazil, are not yet available, it is justified to develop an instrument to monitor the indicators of the Brazilian children’s development to be applied during vaccination campaigns, due to the need to establish a viable strategy to obtain information that can support the implementation of early childhood policies. Brazil's experience in conducting surveys on breastfeeding during multi-vaccination campaigns has led to technical-operational learning, and cost and time reduction in relation to home surveys; this motivated the creation of an instrument for monitoring CD to be applied in this context.
Particularly, it is necessary to have an instrument that differs from the individual screening tests used in population surveys in Brazil, such as the Denver,24 the Bayley,25 and the Ages & Stages Questionnaire,26 which have the disadvantage of having access restricted by copyright and the need for specialized personnel for their application, as well as the time required to apply them.
The starting point of this study was to define the instrument’s scope, which should be aimed at monitoring CD population indicators to differentiate it from other types of tests, such as individual screening tests, which raise ethical issues when applied in clinical or educational contexts because screened cases can be referred for diagnostic evaluation, specialized treatments, or special programs.3
The interview with the children’s primary caregivers is supported by evidence that interviews with caregivers from all socioeconomic levels provide valid information, as the classifications are well correlated with the child's direct measurements.3,26–28 Among the advantages of interviews with caregivers, the following should be highlighted: they are easy to apply in comparison with direct tests or observations; they tend to be fast, low-cost, easy-to-complete, and do not require much time or experience to interpret29; and, they are accurate, because parents observe their children's behavior over time in several circumstances, unlike direct observations by health professionals, which are generally single/cross-sectional and depend on the child's collaboration at the time of the assessment.
Choosing a comprehensive approach to CD rather than domain-specific scales has followed the recent global trend. The use of more complete instruments provides a comprehensive overview of CD at the population level, which favors the identification of the necessary interventions.3
QAD-PIPAS also incorporated questions related to health, nutrition, education, and social protection and safety, as well as the children's experiences in the family environment, allowing analysis and comparison of this information between groups. It is well known that children living in stimulating environments are more likely to reach school age with better capacity to learn reading and writing, and that parents who frequently interact with their children promote their socio-emotional development, with these environmental influences being more important than conditions that involve poverty, malnutrition, and disease. Language development is strongly influenced by exposure to words and books at home, so much so that children whose parents are not literate may develop speech and vocabulary more slowly. Thus, by incorporating questions from the MICS,20 simple and essential information will be provided for the planning of interventions aimed at parenting and bond-strengthening.
In conclusion, the present study provides a population-level assessment tool (QAD-PIPAS) to policy makers, managers, and practitioners from different sectors and the general society that takes into account four domains of CD, adjusted to local culture, including items evaluated and validated by a group of specialists from the perspective of clinical practice, research, and policies directed at early childhood. Its application in a pilot study showed the adequacy and feasibility of its use in vaccination campaigns, quickly and at reduced costs. Therefore, the instrument is expected to contribute to the teaching, research, and the creation and implementation of intersectoral policies aimed at early childhood in Brazil.
FundingDirective 047/2014 MCTI/CNPq/MS/DECIT/Bill and Melinda Gates Foundation (Process No. 401721/2015-9).
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Amira Figueiras, Anna Maria Chiesa, Gilvani Pereira Grangeiro, Honorina de Almeida, Janaína Monteiro Chaves, Miriam Guerra, Rudimar Riesgo, and Sophie Eikmann, for their contribution in the validation of the instrument, and the teams from the Federal District, Recife, and Embu das Artes for their support during the pre-test of the instrument.
Please cite this article as: Venancio SI, Bortoli MC, Frias PG, Giugliani ER, Alves CR, Santos MO. Development and validation of an instrument for monitoring child development indicators. J Pediatr (Rio J). 2020;96:778–89.
Study conducted at Instituto de Saúde da Secretaria de Estado da Saúde de São Paulo, São Paulo, SP, Brazil.
articles





