
To evaluate the number of asthma deaths and the temporal trend of the asthma-specific mortality rate in children and adolescents up to 19 years of age in Brazil.
MethodsThis is an ecological time-series study of asthma deaths reported in Brazil, in the population up to 19 years of age, between 1996 and 2015. The specific asthma mortality rate and its temporal trend were analyzed.
ResultsThere were 5014 deaths during the 20 years evaluated, with the majority, 68.1%, being recorded in children under 5 years of age. The specific asthma mortality rate ranged from 0.57/100,000 in 1997 to 0.21/100,000 in 2014, with a significant reduction of 59.8%. Regarding the place of death, 79.4% occurred in a hospital setting. In this sample, the adolescents had a 1.5-fold higher chance of death out-of-hospital than children up to nine years of age. There was no significant difference in the temporal trend between the genders and no significant decrease in out-of-hospital deaths.
ConclusionsThis study found a temporal trend for a reduction in asthma deaths over 20 years in children and adolescents in Brazil. Mortality rates varied across the geographic regions of the country and were higher in the Northeast. The prevalence of deaths under 5 years of age may be associated with the greater vulnerability of this age group in low-income countries. In adolescence, deaths outside the hospital environment are noteworthy. Asthma deaths are rare but unacceptable events, considering the treatable nature of the disease and the presence of avoidable factors in most of fatal outcomes.
Estimar o número de óbitos por asma e a tendência temporal da taxa de mortalidade por asma em crianças e adolescentes no Brasil.
MétodosEstudo ecológico de séries temporais em que foram avaliados os óbitos por asma ocorridos no Brasil entre 1996 e 2015, na população com até 19 anos. Foram analisadas a taxa de mortalidade específica por asma e a sua tendência temporal.
ResultadosOcorreram 5.014 óbitos, a maioria (68,1%) registrada em menores de cinco anos. Observou-se uma oscilação da taxa de mortalidade específica por asma entre 0,57 e 0,21/100.000 habitantes, o que correspondeu a uma redução de 59,8% no período. Quanto ao local dos óbitos, 79,4% ocorreram em ambiente hospitalar. Nesta amostra o adolescente teve 1,5 vez mais chance de óbito por asma fora do ambiente hospitalar do que as crianças até nove anos. Não foi observada diferença significativa da redução da tendência temporal entre os sexos e dos óbitos fora do ambiente hospitalar.
ConclusõesHouve tendência temporal de redução da mortalidade por asma em crianças e adolescentes nos 20 anos avaliados. As taxas de mortalidade variaram nas diversas regiões geográficas do país, foram mais elevadas na Região Nordeste. O predomínio dos óbitos abaixo de cinco anos pode se associar a maior vulnerabilidade desse grupo em países de baixa renda. Na adolescência, ressaltam-se óbitos fora do ambiente hospitalar. As mortes por asma são eventos inaceitáveis, considera-se o caráter tratável da doença e a presença de fatores evitáveis na maioria dos desfechos fatais.
Asthma affects about 334 million individuals worldwide.1 It represents the most common chronic disease in childhood and adolescence, impairs quality of life, and is associated with school absenteeism and parental work absenteeism.2,3 In Brazil, the mean prevalence of active asthma was estimated at 18.5% in adolescents.4
The disease can lead to exacerbations, crises, or acute attacks that result in hospitalizations and, rarely, deaths. The social, emotional, and economic burden of the disease is considerable. It is estimated that a total of 250,000 asthma deaths occur every year worldwide. The asthma mortality rate is a good indicator of the quality of care and, when it is high, it is related to the poor quality of the services provided.1
The epidemiological surveillance at the population level contributes to the creation of strategies and effective public policies to develop and improve the disease approach and to detect early epidemic outbreaks of fatal asthma. Two outbreaks have been reported in the last decades. The first occurred in the 1960s, with an approximately 50% increase in asthma mortality rates between the ages of five and 34 years, which was attributed to the effects of high doses of isoprenaline, a non-specific beta adrenergic bronchodilator. This medication was widely used as a rescue medication in acute asthma and had toxic cardiac effects. The second epidemic outbreak occurred in the 1980s and represented a 38% increase in asthma mortality rates in the same age group.5 In 2016, a major epidemic of acute asthma attacks related to a great thunderstorm was described in Melbourne and nine possible deaths from asthma were reported as being related to this event. Similar cases have been reported in other regions of the world, but not as lethal as this one.6
Asthma deaths are considered as infrequent but unacceptable events, considering the treatable nature of the disease. The aim of this study was to evaluate the deaths and the temporal trend of the specific asthma mortality rate (SAMR) in Brazilian children and adolescents according to gender, age group, geographic region, and place of death.
MethodsThis is an ecological time-series study that evaluated asthma deaths that occurred in Brazil in the period between 1996 and 2015, in children and adolescents up to 19 years of age. Data were collected from the Department of Informatics of the Brazilian Unified Health System (DATASUS), which belongs to the Brazilian Ministry of Health. Data were collected from the General Coordination of Epidemiological Information and Analysis, Health Surveillance Secretariat, Mortality Information System and population projection data from the Brazilian Institute of Geography and Statistics, a public organization responsible for Brazilian data and statistics.
Deaths were identified according to the International Statistical Classification of Diseases and Health Related Problems (ICD), 10th revision, using the codes J-45 (asthma) and J-46 (status asthmaticus) recorded in the death certificate as the underlying cause of death and made available by DATASUS as of 1996. The main variable studied was the specific asthma mortality rate (SAMR), which corresponds to the number of deaths from asthma in a given population, divided by the number of inhabitants and multiplied by 100,000.
The following variables were analyzed: gender, place of death (in-hospital or out-of-hospital setting: home, public street, other health facilities, others, unknown), geographic region (North, Midwest, Northeast, South, and Southeast), and age group (less than 1 year, 1–4 years, 5–9 years, 10–14 years, and 15–19 years).
Simple linear regression analysis was performed to evaluate the temporal trend of change in the overall specific asthma mortality rate (SAMR), by age group, gender, place of death, and its geographic region of occurrence, as well as their confidence intervals. Mortality coefficients were considered dependent variables (Y) and the calendar years the independent variables (X). A centralized variable (X−2005) was considered to prevent autocorrelation between the terms of the equation. The estimated model was Y=β0+β1 (X−2005), where Y=asthma mortality coefficient, β0=mean coefficient in the period, β1=annual mean coefficient change, and X=calendar year. The statistical analysis was carried out with SPSS software (SPSS Statistics for Windows, Version 17.0, Chicago, USA). The accuracy and quality of the model were measured by the coefficient of determination (R2). It is emphasized that the closer to 100% the R2 measurement is, the better and more accurate the adjusted model is, and the closer to 0 the R2 measurement is, the worse and the less accurate the adjusted model is.
The association between two categorical variables was carried out using Pearson's chi-squared test. All results were considered significant for a level of significance (alpha error)<5% (p<0.05).
The present study was approved by the Research Ethics Committee under CAAE number 56856116.7.0000.5149.
ResultsIn Brazil, 5014 asthma deaths occurred in children and adolescents up to 19 years of age in the period between 1996 and 2015, and most (68.1%) occurred in children under 5 years of age. There was an overall prevalence of deaths in males (51.3%), which was statistically significant (p<0.001) in children under 5 years (52.5%) and between 5 and 9 years of age (53.9%). There was a predominance in the female gender (53.7%) in adolescents aged 10–19 years.
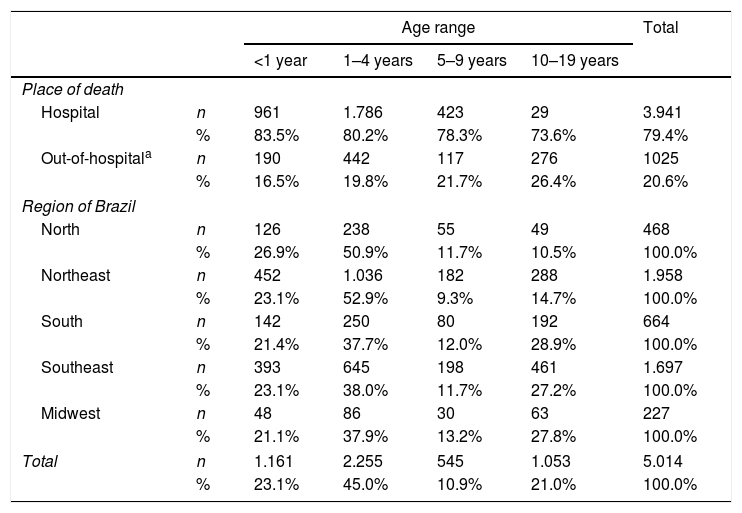
Table 1 shows the distribution of asthma deaths in relation to the age group, place of occurrence, and region of Brazil. It can be observed that 79.4% of deaths occurred in the hospital environment and 20.6% outside the hospital environment (home, public street, other health facilities, others, unknown). Regarding deaths occurring outside the hospital setting, a statistically significant variation was observed between the age groups (p<0.001), being more frequent in adolescents aged 10–19 years (26.4%) than in the other age groups (16.5%, 19.8%, and 21.7% at the age ranges <1 year, 1–4 years, and 5–9 years, respectively). Adolescents showed a 1.5-fold higher chance of death from asthma outside the hospital environment than a child up to the age of 9 (OR=1.5, 95% CI: 1.3–1.8). There was a predominance of deaths in children aged 1–4 years in all Brazilian regions. The highest number of deaths occurred in the Northeast region (1958, 39% of total deaths). In the North and Northeast regions, the number of deaths in children aged 1–4 years was higher than in the other regions, with statistical significance (p<0.001). Among adolescents, the percentage of deaths was significantly higher in the South, Midwest, and Southeast regions than in the North and Northeast regions.
Distribution of deaths from asthma according to age, place of occurrence, and region of Brazil in children and adolescents up to 19 years of age, Brazil, from 1996 to 2015.
| Age range | Total | |||||
|---|---|---|---|---|---|---|
| <1 year | 1–4 years | 5–9 years | 10–19 years | |||
| Place of death | ||||||
| Hospital | n | 961 | 1.786 | 423 | 29 | 3.941 |
| % | 83.5% | 80.2% | 78.3% | 73.6% | 79.4% | |
| Out-of-hospitala | n | 190 | 442 | 117 | 276 | 1025 |
| % | 16.5% | 19.8% | 21.7% | 26.4% | 20.6% | |
| Region of Brazil | ||||||
| North | n | 126 | 238 | 55 | 49 | 468 |
| % | 26.9% | 50.9% | 11.7% | 10.5% | 100.0% | |
| Northeast | n | 452 | 1.036 | 182 | 288 | 1.958 |
| % | 23.1% | 52.9% | 9.3% | 14.7% | 100.0% | |
| South | n | 142 | 250 | 80 | 192 | 664 |
| % | 21.4% | 37.7% | 12.0% | 28.9% | 100.0% | |
| Southeast | n | 393 | 645 | 198 | 461 | 1.697 |
| % | 23.1% | 38.0% | 11.7% | 27.2% | 100.0% | |
| Midwest | n | 48 | 86 | 30 | 63 | 227 |
| % | 21.1% | 37.9% | 13.2% | 27.8% | 100.0% | |
| Total | n | 1.161 | 2.255 | 545 | 1.053 | 5.014 |
| % | 23.1% | 45.0% | 10.9% | 21.0% | 100.0% | |
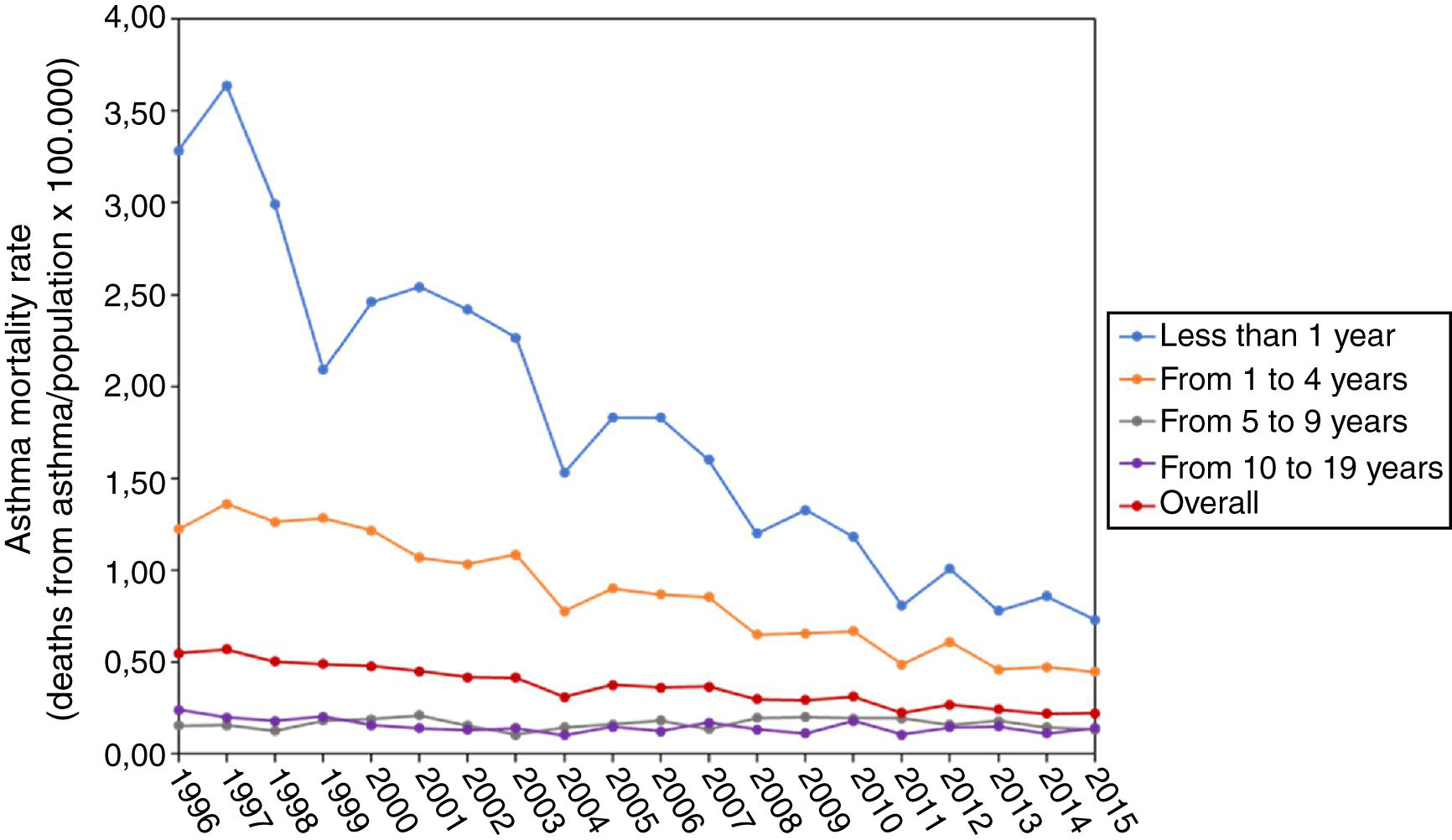
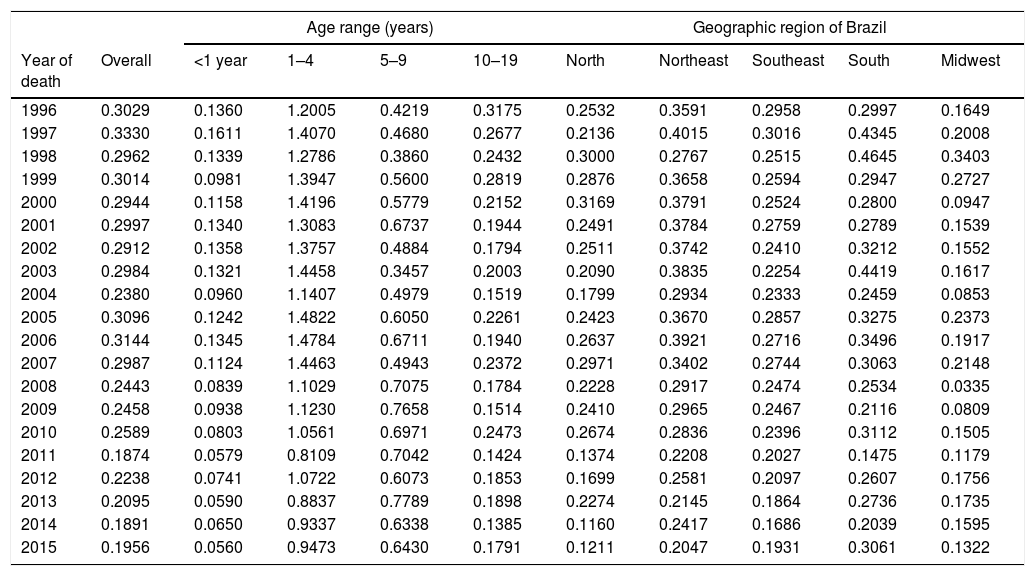
The SAMR in children and adolescents up to 19 years of age in Brazil ranged from a maximum of 0.57 deaths/100,000 inhabitants in 1997 to a minimum of 0.22/100,000 in 2014 and 2015. Table 2 shows the SAMR per year, by age distribution and region of Brazil. The highest SAMR occurred in children under 5 years of age and in the Northeast region during most of the assessed period, except in the years 1997, 1998, 2010, and 2013.
Overall asthma mortality rate, by age group and by geographic region of Brazil in Brazilian children and adolescents, from 1996 to 2015 (per 100,000 inhabitants).
| Age range (years) | Geographic region of Brazil | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Year of death | Overall | <1 year | 1–4 | 5–9 | 10–19 | North | Northeast | Southeast | South | Midwest |
| 1996 | 0.3029 | 0.1360 | 1.2005 | 0.4219 | 0.3175 | 0.2532 | 0.3591 | 0.2958 | 0.2997 | 0.1649 |
| 1997 | 0.3330 | 0.1611 | 1.4070 | 0.4680 | 0.2677 | 0.2136 | 0.4015 | 0.3016 | 0.4345 | 0.2008 |
| 1998 | 0.2962 | 0.1339 | 1.2786 | 0.3860 | 0.2432 | 0.3000 | 0.2767 | 0.2515 | 0.4645 | 0.3403 |
| 1999 | 0.3014 | 0.0981 | 1.3947 | 0.5600 | 0.2819 | 0.2876 | 0.3658 | 0.2594 | 0.2947 | 0.2727 |
| 2000 | 0.2944 | 0.1158 | 1.4196 | 0.5779 | 0.2152 | 0.3169 | 0.3791 | 0.2524 | 0.2800 | 0.0947 |
| 2001 | 0.2997 | 0.1340 | 1.3083 | 0.6737 | 0.1944 | 0.2491 | 0.3784 | 0.2759 | 0.2789 | 0.1539 |
| 2002 | 0.2912 | 0.1358 | 1.3757 | 0.4884 | 0.1794 | 0.2511 | 0.3742 | 0.2410 | 0.3212 | 0.1552 |
| 2003 | 0.2984 | 0.1321 | 1.4458 | 0.3457 | 0.2003 | 0.2090 | 0.3835 | 0.2254 | 0.4419 | 0.1617 |
| 2004 | 0.2380 | 0.0960 | 1.1407 | 0.4979 | 0.1519 | 0.1799 | 0.2934 | 0.2333 | 0.2459 | 0.0853 |
| 2005 | 0.3096 | 0.1242 | 1.4822 | 0.6050 | 0.2261 | 0.2423 | 0.3670 | 0.2857 | 0.3275 | 0.2373 |
| 2006 | 0.3144 | 0.1345 | 1.4784 | 0.6711 | 0.1940 | 0.2637 | 0.3921 | 0.2716 | 0.3496 | 0.1917 |
| 2007 | 0.2987 | 0.1124 | 1.4463 | 0.4943 | 0.2372 | 0.2971 | 0.3402 | 0.2744 | 0.3063 | 0.2148 |
| 2008 | 0.2443 | 0.0839 | 1.1029 | 0.7075 | 0.1784 | 0.2228 | 0.2917 | 0.2474 | 0.2534 | 0.0335 |
| 2009 | 0.2458 | 0.0938 | 1.1230 | 0.7658 | 0.1514 | 0.2410 | 0.2965 | 0.2467 | 0.2116 | 0.0809 |
| 2010 | 0.2589 | 0.0803 | 1.0561 | 0.6971 | 0.2473 | 0.2674 | 0.2836 | 0.2396 | 0.3112 | 0.1505 |
| 2011 | 0.1874 | 0.0579 | 0.8109 | 0.7042 | 0.1424 | 0.1374 | 0.2208 | 0.2027 | 0.1475 | 0.1179 |
| 2012 | 0.2238 | 0.0741 | 1.0722 | 0.6073 | 0.1853 | 0.1699 | 0.2581 | 0.2097 | 0.2607 | 0.1756 |
| 2013 | 0.2095 | 0.0590 | 0.8837 | 0.7789 | 0.1898 | 0.2274 | 0.2145 | 0.1864 | 0.2736 | 0.1735 |
| 2014 | 0.1891 | 0.0650 | 0.9337 | 0.6338 | 0.1385 | 0.1160 | 0.2417 | 0.1686 | 0.2039 | 0.1595 |
| 2015 | 0.1956 | 0.0560 | 0.9473 | 0.6430 | 0.1791 | 0.1211 | 0.2047 | 0.1931 | 0.3061 | 0.1322 |
Fig. 1 shows the decrease in the asthma mortality rate that occurred in the country between the years 1996 and 2015, especially among children under 5 years of age. A reduction of 59.8% in the overall SAMR was observed.

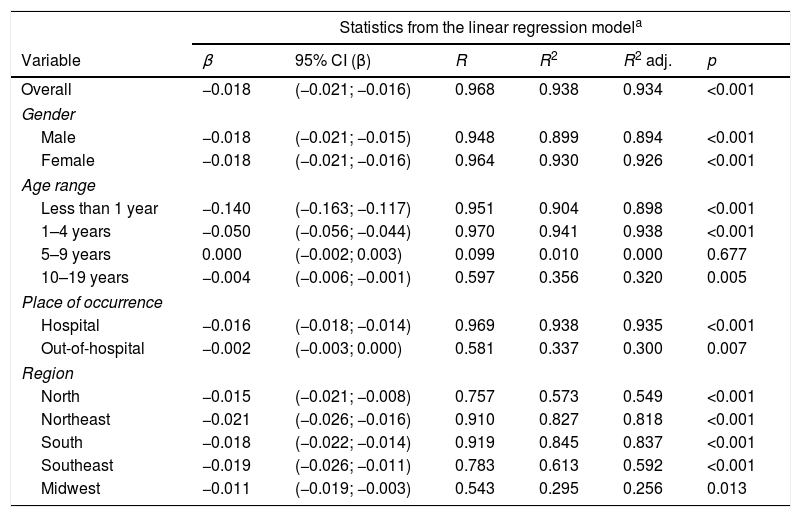
Table 3 shows a simple linear regression analysis; it can be observed that the temporal trend of mortality rate reduction was statistically significant for most of the analyzed categories, except for the age group of 5–9 years. Regarding the place of occurrence, a significant reduction (β coefficient=−0.016, 95% CI: −0.018 to −0.014) was observed in in-hospital deaths, although this trend was not demonstrated for deaths outside the hospital setting. Regarding the temporal trend of mortality in the different geographic regions, a significant reduction (p<0.001) was observed in all regions, corresponding to a reduction in the number of deaths of 66.6%, 62.2%, 58.4%, 43.5%, and 40.1%, respectively, for the Southeast, North, Northeast, Midwest, and South regions.
Mean annual variation of asthma mortality rates (AMR), and according to the variables gender, age, place of occurrence, and region of the country in children and adolescents, from 1996 to 2015.
| Statistics from the linear regression modela | ||||||
|---|---|---|---|---|---|---|
| Variable | β | 95% CI (β) | R | R2 | R2 adj. | p |
| Overall | −0.018 | (−0.021; −0.016) | 0.968 | 0.938 | 0.934 | <0.001 |
| Gender | ||||||
| Male | −0.018 | (−0.021; −0.015) | 0.948 | 0.899 | 0.894 | <0.001 |
| Female | −0.018 | (−0.021; −0.016) | 0.964 | 0.930 | 0.926 | <0.001 |
| Age range | ||||||
| Less than 1 year | −0.140 | (−0.163; −0.117) | 0.951 | 0.904 | 0.898 | <0.001 |
| 1–4 years | −0.050 | (−0.056; −0.044) | 0.970 | 0.941 | 0.938 | <0.001 |
| 5–9 years | 0.000 | (−0.002; 0.003) | 0.099 | 0.010 | 0.000 | 0.677 |
| 10–19 years | −0.004 | (−0.006; −0.001) | 0.597 | 0.356 | 0.320 | 0.005 |
| Place of occurrence | ||||||
| Hospital | −0.016 | (−0.018; −0.014) | 0.969 | 0.938 | 0.935 | <0.001 |
| Out-of-hospital | −0.002 | (−0.003; 0.000) | 0.581 | 0.337 | 0.300 | 0.007 |
| Region | ||||||
| North | −0.015 | (−0.021; −0.008) | 0.757 | 0.573 | 0.549 | <0.001 |
| Northeast | −0.021 | (−0.026; −0.016) | 0.910 | 0.827 | 0.818 | <0.001 |
| South | −0.018 | (−0.022; −0.014) | 0.919 | 0.845 | 0.837 | <0.001 |
| Southeast | −0.019 | (−0.026; −0.011) | 0.783 | 0.613 | 0.592 | <0.001 |
| Midwest | −0.011 | (−0.019; −0.003) | 0.543 | 0.295 | 0.256 | 0.013 |
The present study reveals a temporal trend of reduction in the SAMR in Brazilian children and adolescents, corroborating the findings of other studies carried out in different age groups.7–10
The analysis showed that the number of deaths in children under 5 years of age predominated in all regions but were significantly higher in the North and Northeast regions. The difficulty in defining the disease before the age of 5 years and in the elderly, due to comorbidities, sometimes makes it impossible to determine asthma as the underlying cause of death and results in most studies on asthma mortality excluding children under five and adults older than 34 years.11 However, in the present study, most (68.1%) asthma deaths occurred in children under 5 years of age, 45% of which were observed in children between 1 and 4 years of age, a fact also observed in another Brazilian study.8 Therefore, the authors considered it essential to include this age group in the current analysis. The methodological limitations for a more accurate diagnosis should not lead us to ignore this sad reality, especially in low-income countries and regions, where this group represents a higher proportion of asthma mortality in childhood and adolescence. Chronic respiratory diseases constitute a major burden for health services and more than 80% of asthma deaths worldwide occur in low-income countries, suggesting underdiagnosis, undertreatment, and difficulties in accessing the needed healthcare.12 Other contributing factors include reluctance to diagnose asthma in young children, delay in initiating treatment, prescription of drugs of dubious efficacy, and low parental schooling, which interferes with adherence and inhalation therapy.13,14
There was a predominance of deaths in male children under 1 year of age and in those between 5 and 9 years. Regarding adolescents between 10 and 19 years of age, the predominance was in the female gender. The differences found in relation to gender are not yet well understood and may reflect differences in the incidence and prevalence of the disease.15 In Brazil, a prevalence study observed a slight predominance of males among the children, as well as among adolescents.16
Regarding the place of occurrence, it is reasonable to assume that cases of out-of-hospital deaths can mean difficulty in having access to health services and/or underdiagnosis and undertreatment of the disease. Most deaths (79.4%) occurred in the hospital environment and the reduction in SAMR was more significant in this subgroup. However, the number of deaths outside the hospital environment is still high (20.6%). Other Brazilian studies have also shown that most asthma deaths occur in hospitals, but that rates of death occurring at home remain high.17,18
The higher risk of death from asthma (OR) outside the hospital setting among adolescents cannot be explained by this study. However, asthma at this stage of life is known to be a risk for complications. Lack of knowledge, undertreatment, and erratic self-medication, along with other issues such as denial of disease severity, poor adherence, risk behaviors, and psychosocial factors are possible explanations.19
Considering a more stringent interpretation, it can be speculated that asthma deaths should not occur, since it is a treatable disease. The studies estimate that most fatal outcomes could be prevented if the patients had improved the disease management in the year prior to death.20,21 The main risk factors associated with death were failure to perceive and recognize the severity of the disease and its exacerbations, frequent visits to emergency services, insufficient education and adherence of the patient, his/her family, and/or health professionals related to treatment, overuse of short-acting bronchodilators and administration of long-acting bronchodilators in isolated formulations, lack of or irregular use of inhaled corticosteroids, absence of a written action plan, smoking, presence of psychiatric and emotional disorders, and socioeconomic vulnerability.22
In developed countries, asthma deaths in the hospital environment are less frequent. In Australia, 60% of asthma-related deaths occurred at home.23 In the United Kingdom, most (75%) of deaths in children and adolescents up to 20 years of age occurred before hospital arrival.20 It is difficult to infer the reason for this difference, but it is important to emphasize the importance of adequately applying asthma crisis treatment protocols to ensure the quality of hospital care.
The asthma mortality rate in Brazil has shown a reduction trend. De Souza-Machado et al. identified a reduction in SAMR from 1.68/100,000 inhabitants in 1998 to 1.32/100,000 in 2009 by analyzing all the age groups together. Mortality reduction was observed in the more developed regions of the country, such as the Southeast, South, and Midwest regions, whereas there was an increase in the less developed regions: North (not statistically significant) and Northeast.7
According to Lotufo et al., the mortality rate was higher in white individuals (0.25/100,000), followed by brown, black, and Asian individuals (0.19, 0.05, and 0.01 per 100,000, respectively) and they observed a reduction in the temporal trend of mortality from 1980 to 1992 and from 1997 to 2010 in the age range between 5 and 34 years.10
The SAMR trend analysis by Graudenz et al., performed in the overall population and in two specific age groups, up to 4 years and from 5 to 34 years, showed a reduction of rates in the period from 1980 to 2014.9
Finally, Priestsch et al. described SAMR in children and adolescents up to 19 years of age and recorded a significant decrease during the evaluated period in all age groups from 1980 to 2007. Most deaths were observed in children under five years of age.8
The American Lung Association Epidemiology and Statistics estimates that asthma mortality and hospitalization have decreased since 1999 in the United States of America. In the age groups of 1–4 years, 5–14 years, and 5–24 years, it was, respectively, 0.2, 0.3, and 0.4 per 100,000 inhabitants.24 The present study recorded, in the year 2009, in individuals aged up to 19 years, a SAMR of 0.29, and in those aged 1–4 years, of 0.65 per 100,000 inhabitants, which are higher rates than those of the American investigation.
The temporal trend of asthma mortality in the 5–35-year age group was analyzed in 46 countries from 1993 to 2012. A reduction of 57% in global asthma mortality was estimated, but there was no significant change in the data between 2006 and 2012.11
According to the Global Burden of Disease, asthma mortality has decreased significantly throughout the world over the past few decades. Asthma mortality rates in children range from 0.0 to 0.7 per 100,000 population worldwide and are associated with the prevalence of the severe forms of the disease and hospitalization rates.5 The study reported that SAMR in Brazilian children and adolescents is within the recorded world limits,5 but when the data are stratified by age group, mortality is higher than that reported in an American study in children aged between 1 and 4 years.21
The reasons for the temporal trend of asthma mortality reduction were not investigated. However, it is possible to make some speculations. In the assessed period, there was a consistent overall reduction in infant mortality in all Brazilian regions, due to the decrease in fecundity, as well as public interventions in health, sanitation, and parental education improvement, among other aspects. Nevertheless, the mean values remain high, especially in the Northeast and North regions.25 The introduction of inhaled corticosteroids to control the disease is considered a fundamental milestone in reducing asthma mortality. It is well recognized that the increased use of these drugs reduces hospitalization and mortality rates.26 The experience accumulated by all Brazilian programs to fight asthma has been used as one of the pillars of disease control.27 The availability and supply of the drugs are still heterogeneous, sometimes irregularly distributed, and insufficient in several regions of the country; in addition health professionals may not be prepared to provide directions on inhaled therapy.7
A limitation of ecological studies is related to the use of data collected in population groups and, thus, it is not possible to infer a causal association to explain the increase or reduction in mortality rates.28,29 The inaccurate coding of the underlying cause of death due to lack of knowledge about the medical history can lead to the underreporting and inaccurate estimation of rates. Notwithstanding its limitations, it is known that DATASUS continually improves its database and that its information is essential.18 Even if there was an underreporting of asthma deaths, there is no reason to believe that it was higher in the most recent period and that it would explain the temporal trend for the decrease in the SAMR.
The present study used a single version of the International Coding of Diseases (ICD-10) and demonstrated that the temporal trend of asthma mortality in childhood and adolescence in Brazil showed a decrease in all assessed age ranges, except in the age group of 5–9 years, and it was more significant in children under 5 years of age during the evaluated 20-year period. The decrease in SAMR was observed in all geographic regions of the country. There was a reduction in in-hospital deaths, but there was no reduction in mortality outside the hospital setting. The highest rates were found in the Northeast and North regions, possibly reflecting the socioeconomic inequities that result in access difficulties and quality limitations regarding the health resources available in the country. Despite the imprecision and the difficulties in asthma diagnosis in children under 5, the greater vulnerability of this age group was demonstrated, as well as the need for more attention and priority for health actions. In adolescence, the highest occurrence of deaths outside the hospital environment is highlighted, demonstrating the possibility of underestimating disease severity and the need for treatment. In Brazil, asthma-related mortality is still high and may occur prematurely in childhood and adolescence. To prevent deaths, it is necessary to plan and implement strategies coordinated by the Unified Health System, with special emphasis on the training of primary health care professionals and emergency care teams, since there are not enough specialists to deal with most cases of asthma in the country.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Pitchon RR, Alvim CG, Andrade CR, Lasmar LM, Cruz ÁA, Reis AP. Asthma mortality in children and adolescents of Brazil over a 20-year period. J Pediatr (Rio J). 2020;96:432–8.
Study conducted at Universidade Federal de Minas Gerais, Programa de Pós-Graduação em Ciências da Saúde da Criança e do Adolescente, Belo Horizonte, MG, Brazil.
articles





